The Journey to Hepatitis C Elimination in Taiwan: Insights From the Hemodialysis Population
Ming-Yan Jiang, Yi-Chan Lee, Tsung-Hsueh Lu

TL;DR
This study examines progress in eliminating hepatitis C in Taiwan's hemodialysis patients, finding that RNA testing remains a major barrier despite improved treatment rates.
Contribution
The study identifies RNA confirmation as the largest gap in HCV care for hemodialysis patients in Taiwan's DAA era.
Findings
Only 48.2% of HCV antibody-positive patients underwent RNA testing, the largest drop in the care cascade.
Treatment initiation rates rose to 73.4% among viremic patients by 2021.
Regional disparities in RNA testing ranged from 38% to 67% across different areas of Taiwan.
Abstract
Hemodialysis patients are a priority population for hepatitis C virus (HCV) elimination in Taiwan, where HCV prevalence and end-stage kidney disease burden are high. The introduction of direct-acting antivirals (DAAs) has accelerated elimination efforts. This study evaluated HCV care cascade and identified gaps among Taiwan's hemodialysis patients in the DAA era. We conducted a retrospective cohort study using National Health Insurance Research Database from 2015 to 2021. Adult patients receiving long-term hemodialysis were included. HCV infection was defined as positive RNA test, and treatment initiation as receipt of ≥7 days of DAA therapy. We assessed the care cascade, annual and cumulative treatment rates, and disparities by demographic and facility characteristics. Among 14 755 HCV antibody-positive patients, 48.2% underwent confirmatory RNA testing. Of 4783 viremic patients,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
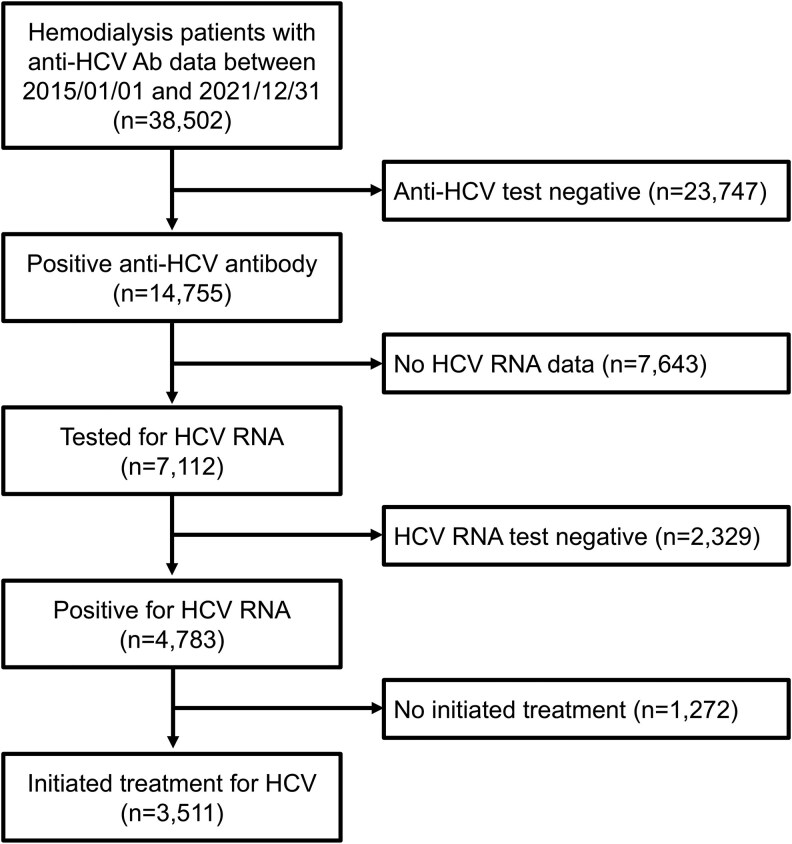 Figure 1
Figure 1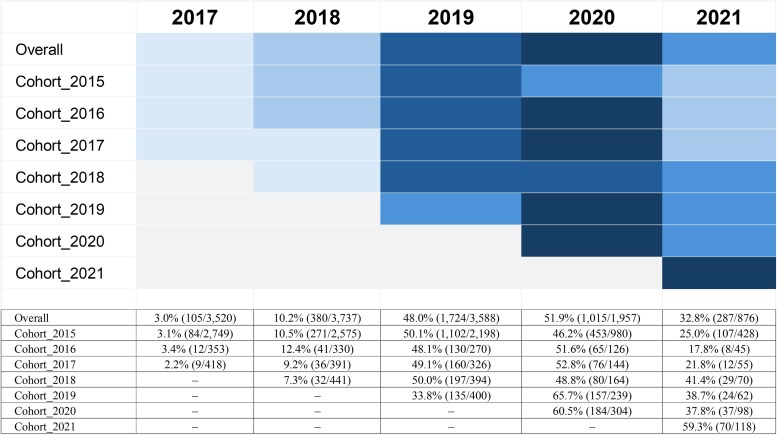 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · Hepatitis B Virus Studies · HIV/AIDS drug development and treatment
Hepatitis C virus (HCV) infection remains a major global health challenge [1, 2], including in Taiwan [3, 4]. In 2016, the World Health Organization (WHO) set a goal to eliminate HCV as a public health threat by 2030 [5]. In response, Taiwan launched a comprehensive national strategy aiming to eliminate HCV by 2025, 5 years ahead of the WHO target [6–8]. This strategy focused on early detection, expanded access to direct-acting antivirals (DAAs), and optimized care delivery across diverse populations [6–8].
A pivotal advancement in Taiwan's national strategy was the phased introduction and expansion of DAA therapy coverage through the National Health Insurance (NHI) system [6–8]. The NHI covered the full cost of HCV diagnosis including anti-HCV antibody testing and RNA confirmation, and the DAA medications, effectively eliminating patient financial barriers such as copayments or coinsurance, a model vital for achieving high treatment uptake. To further enhance treatment access and equity, Taiwan systematically decentralized HCV care by integrating screening and treatment into local health facilities and empowering nonspecialist healthcare providers, including general practitioners, to prescribe DAAs. Specific efforts were made to encourage provider participation through educational initiatives and to optimize service delivery via microelimination programs targeting high-risk groups such as hemodialysis patients. While DAA therapy in Taiwan was initially prescribed predominantly by gastroenterology/hepatology specialists, an increasing proportion of prescriptions were later provided by trained nonspecialist physicians as decentralized treatment pathways and educational initiatives expanded. These system-level changes, supported by robust national surveillance for data-driven policy adjustments, provided the foundation for effective care delivery [6–8].
Given Taiwan's high burden of treated end-stage kidney disease, which has the highest global prevalence at 3806 cases per million population in 2022 [9], and the high prevalence of HCV in this population [10–12], hemodialysis patients have been identified as a priority for elimination efforts [6–8]. Local initiatives have demonstrated the success of targeted approaches [13, 14]. For example, the Changhua Integrated Program to Stop HCV Infection (CHIPS-C) program, a collaborative care model led by the local health authority, showed that targeted microelimination strategies increased DAA treatment uptake among dialysis patients in Changhua County from 25% to nearly 90% [13]. This program utilized a cross-sectoral, multidisciplinary partnership to integrate HCV care into existing health services, simplify care processes, and optimize delivery to affected populations [13]. Similarly, the ERASE-C Campaign in Southern Taiwan, which combined mass screening with on-site group treatment across 18 hemodialysis units, demonstrated the feasibility of achieving HCV microelimination in dialysis facilities [14].
Prior to the DAA era, the treatment rate for HCV among hemodialysis patients in Taiwan was historically low, with only 6% receiving interferon-based therapy [15]. Despite the recent progress demonstrated by local microelimination programs [13, 14], uncertainties remain regarding the national implementation of HCV therapy among the dialysis population. It is unclear whether expanded policies have translated into equitable access and improved treatment uptake nationwide. Using the National Health Insurance Research Database (NHIRD), this study aimed to characterize trends in the HCV care cascade among hemodialysis patients in Taiwan and to identify gaps in diagnostic testing and treatment uptake from the beginning of the DAA era in 2015 through 2021.
METHODS
Data Source and Study Population
We conducted a retrospective cohort study using the Taiwan NHIRD, a nationwide claims database maintained by the Ministry of Health and Welfare [16, 17]. The NHI operates a single-payer, universal coverage system, covering over 99% of Taiwan's population, including all citizens and legal foreign residents. The NHIRD is derived from this system, containing deidentified demographic information, longitudinal medical records, prescription claims, and selected laboratory test results from the National Health Insurance Laboratory Database [18].
We used the viral hepatitis dataset, which identifies patients with hepatitis B or C using ICD-9-CM (070, 570–573) and ICD-10-CM (B15–B19, K70–K77) codes between 2015 and 2021 (Supplementary Figure 1). Eligible participants were adults (≥18 years) who had received hemodialysis for at least 3 consecutive months, identified by a specific reimbursement code (n = 46 644). We excluded patients who died in 2015–2016 (n = 4201) and those who received HCV treatment prior to dialysis initiation (n = 585). We further excluded 3356 patients who lacked both anti-HCV antibody and HCV RNA test results, resulting in a final analytic cohort of 38 502 hemodialysis patients (Supplementary Figure 1).
Supplementary Material
ofag039_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization . Global Health Observatory data: chronic viral hepatitis. Available at: https://www.who.int/data/gho/data/themes/chronic-viral-hepatitis. Accessed 13 September 2025.
- 2Polaris Observatory HCV Collaborators . Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: a modelling study. Lancet Gastroenterol Hepatol 2022; 7:396–415.35180382 10.1016/S 2468-1253(21)00472-6 · doi ↗ · pubmed ↗
- 3Bennett H, Waser N, Johnston K, et al A review of the burden of hepatitis C virus infection in China, Japan, South Korea and Taiwan. Hepatol Int 2015; 9:378–90.26071238 10.1007/s 12072-015-9629-x · doi ↗ · pubmed ↗
- 4Chen YY, Chen CL, Chen JW, et al Secular trends and geographic maps of hepatitis C virus infection among 4 million blood donors in Taiwan from 1999 to 2017. Hepatol Commun 2020; 4:1193–205.32766478 10.1002/hep 4.1531 PMC 7395065 · doi ↗ · pubmed ↗
- 5World Health Organization . Combating hepatitis B and C to reach elimination by 2030: advocacy brief. WHO/HIV/2016.04. Geneva: World Health Organization, 2016.
- 6Ministry of Health and Welfare, Executive Yuan Taiwan . Taiwan Hepatitis C policy guidelines 2018–2025. Taipei City: Ministry of Health and Welfare, 2019.
- 7Chien RN, Lu SN, Pwu RF, Wu GH, Yang WW, Liu CL. Taiwan accelerates its efforts to eliminate hepatitis C. Glob Health Med 2021; 3:293–300.34782872 10.35772/ghm.2021.01064 PMC 8562095 · doi ↗ · pubmed ↗
- 8Chien RN, Lu SN, Wu GH, et al Policy and strategy for hepatitis C virus elimination at the national level: experience in Taiwan. J Infect Dis 2023; 228:S 180–8.37703347 10.1093/infdis/jiad 016 · doi ↗ · pubmed ↗