Headache as a Predictor of Cryptococcal Meningitis in Ambulatory Patients With Symptomatic HIV-associated Cryptococcal Antigenemia
Sarah M Najjuka, Alexandra Poeschla, Abduljewad Wele, Elizabeth Nalintya, Paul Kirumira, Peruth Ayebale, Grace Nakitto, Fred Turya, Lydia Nankungu, Caleb P Skipper, Ann Fieberg, Biyue Dai, David R Boulware, David B Meya, Radha Rajasingham

TL;DR
Headache is a strong indicator of meningitis in HIV patients with cryptococcal antigenemia, especially when combined with high antigen levels.
Contribution
Identifies headache and high CrAg titer as a reliable predictor of meningitis in HIV patients with antigenemia.
Findings
Headache alone has 95% sensitivity for predicting meningitis but low specificity.
Combining headache with CrAg titer ≥1:160 increases predictive accuracy to 79%.
A logistic regression model with multiple symptoms and CrAg titer achieves an AUROC of 0.86.
Abstract
People with HIV-associated cryptococcal antigenemia are at high risk for meningitis and death. In resource-limited settings, lumbar puncture to evaluate for meningitis is infrequently performed in asymptomatic individuals; therefore, symptomatic individuals are prioritized. We evaluated the predictive value of meningeal symptoms for cryptococcal meningitis in people with cryptococcal antigenemia. We conducted a secondary analysis from 3 randomized clinical trials conducted in Uganda between 2017 and 2024. We included adults with meningeal symptoms who had cerebrospinal fluid cryptococcal antigen (CrAg) testing performed. Logistic regressions and classification trees were used to determine the associations between meningeal symptoms and meningitis. Area under the receiver operating characteristic curve (AUROC) and misclassification rate were used to evaluate model performance. Among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
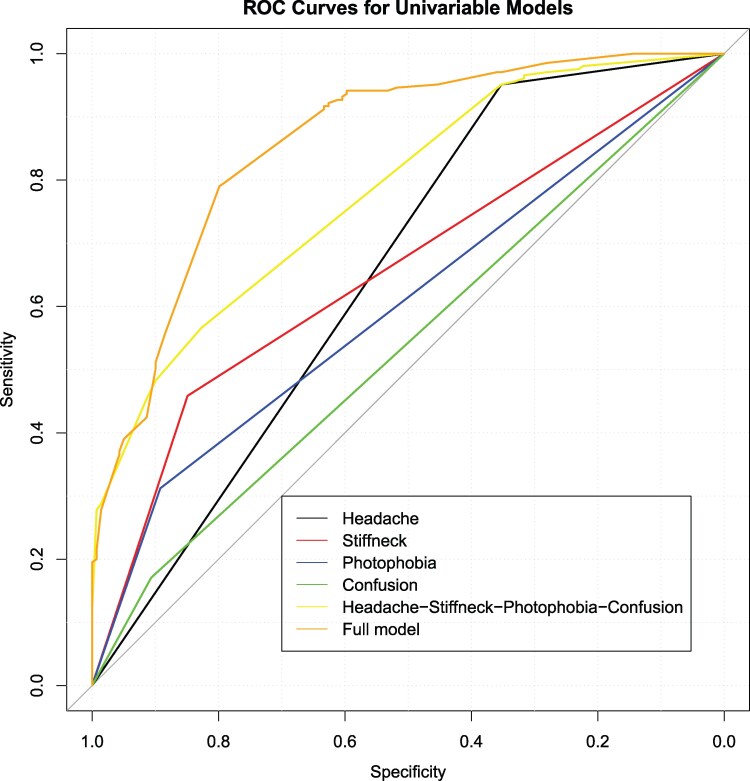 Figure 1
Figure 1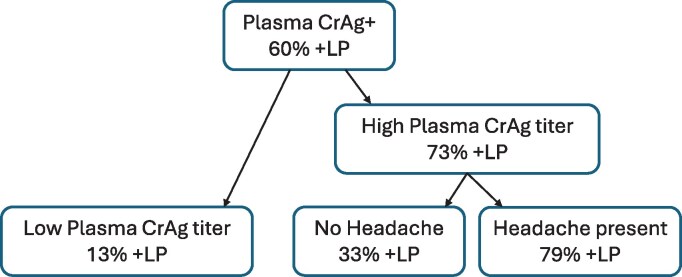 Figure 2
Figure 2| Variable | N With Data | Overall Cohort | Positive CSF CrAg | Negative CSF CrAg |
|
|---|---|---|---|---|---|
| No. per group | 344 | 344 | 205 | 139 | |
| Demographics | |||||
| Age, y | 344 | 36 [30, 41] | 36 [30, 41] | 36 [30, 42] | .77 |
| Male | 344 | 188 (55%) | 109 (58%) | 79 (48%) | <.01 |
| Antiretroviral therapy (ART) | |||||
| Currently on ART | 96 | 96 (28%) | 51 (25%) | 45 (32%) | .31 |
| Never on ART | 223 | 223 (65%) | 139 (68%) | 84 (60%) | |
| Previously on ART | 25 | 25 (7%) | 15 (7%) | 10 (7%) | |
| Duration on ART, m | 94 | 1.6 [0.4, 6.7] | 1.7 [0.5, 4.5] | 1.6 [0.4, 11.5] | .87 |
| Signs and symptoms | |||||
| Glasgow Coma Scale <15 | 283 | 27 (10%) | 18 (10) | 9 (9%) | .67 |
| Headache | 344 | 285 (83%) | 195 (95%) | 90 (65%) | <.001 |
| Stiff neck | 344 | 115 (33%) | 94 (46%) | 21 (15%) | <.001 |
| Fever | 344 | 122 (36%) | 74 (36%) | 48 (34%) | .77 |
| Mania | 344 | 18 (5%) | 11 (5%) | 7 (5%) | .89 |
| Confusion | 344 | 48 (14%) | 35 (17%) | 13 (10%) | .04 |
| Seizures | 344 | 17 (5%) | 14 (7%) | 3 (2%) | .05 |
| Photophobia | 344 | 79 (23%) | 64 (31%) | 15 (11%) | <.001 |
| Focal neurologic deficits | 344 | 11 (3%) | 5 (2%) | 6 (4%) | .33 |
| Visual changes | 312 | 14 (5%) | 7 (4%) | 7 (6%) | .41 |
| Other CNS symptoms | 344 | 65 (19%) | 36 (18%) | 29 (21%) | .44 |
| Baseline laboratory results | |||||
| CD4+ cell count/µL | 242 | 33 [16, 68] | 28 [15, 56] | 38 [19, 79] | .07 |
| Plasma CrAg titer, 1:x | 278 | 1280 [100, 2560] | 2560 [640, 2560] | 80 [20, 640] | <.001 |
| Plasma CrAg titer ≥1:160 | 344 | 208 (60%) | 152 (74%) | 56 (40%) | <.001 |
| Sodium, mmol/L | 115 | 134 [130, 137] | 132 [127, 134] | 134 [131, 137] | <.01 |
| Hemoglobin, g/dL | 118 | 11.3 [9.9, 12.7] | 11.7 [10.4, 13.0] | 11.3 [9.9, 12.4] | .47 |
| Potassium, mmol/L | 115 | 4.3 [4.0, 4.6] | 4.0 [3.6, 4.3] | 4.3 [4, 4.6] | <.01 |
| Platelets ×103/µL | 113 | 261 [187, 343] | 252 [171, 335] | 269 [187, 343] | .62 |
| Creatinine, mg/dL | 114 | 0.7 [0.6, 0.9] | 0.6 [0.6, 0.7] | 0.7 [0.6, 0.9] | .12 |
| Univariate Models | |||
|---|---|---|---|
| Symptoms | OR (95% CI) |
| AUC (95% CI) |
| Headache | 10.6 (5.35–23.1) | <.001 | 0.65 (0.61–0.69) |
| Stiff neck | 4.76 (2.82–8.33) | <.001 | 0.65 (0.61–0.70) |
| Photophobia | 3.75 (2.08–7.14) | <.001 | 0.60 (0.56–0.64) |
| Confusion | 2.00 (1.04–4.06) | .045 | 0.54 (0.50–0.57) |
| Clinical characteristics | |||
| Male sex | 1.98 (1.28–3.08) | .002 | 0.58 (0.53–0.64) |
| Crag titer ≥ 1:160 | 17.0 (8.45–38.3) | <.001 | 0.70 (0.65–0.74) |
- —NIAID10.13039/100000060
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Nail Diseases and Treatments · Streptococcal Infections and Treatments
Cryptococcal meningitis is the most common cause of HIV-related meningitis and is estimated to cause 19% of AIDS-related deaths worldwide [1]. Subclinical infection, known as cryptococcal antigenemia, can be identified by detection of cryptococcal antigen (CrAg) in the bloodstream before onset of fulminant meningitis [2]. The World Health Organization recommends screening all people with HIV and CD4 count <100 cells/µL for CrAg in the blood, and subsequent fluconazole preemptive treatment for those who are CrAg positive to mitigate the risk of meningitis and death [3]. Given that ∼30% of blood CrAg-positive people will go on to develop fulminant meningitis, lumbar puncture (LP) is recommended by some national guidelines [4]. Practically, because of limited resources in busy clinics and patient fears of LPs, LPs are often only performed in symptomatic individuals [5, 6], assuming that symptoms are suggestive of meningitis.
High plasma CrAg titer is a risk factor for meningitis and death [7, 8]. However, symptoms such as headache that are commonly associated with meningitis have not been thoroughly evaluated as indicators of cryptococcal meningitis among persons with cryptococcal antigenemia. In the clinical setting, people with HIV who are CrAg positive are typically screened for symptoms including headache, fever, neck stiffness, and neurologic changes. People reporting symptoms may be triaged for LP, but it is unknown which symptoms in particular are predictive of meningitis in people with cryptococcal antigenemia.
The objective of this study was to evaluate which symptoms are predictive of meningitis among people with HIV-associated cryptococcal antigenemia. Understanding the symptomatology associated with meningitis among people with cryptococcal antigenemia would allow healthcare workers to provide better counseling for LPs.
METHODS
Study Design, Site, and Population
This is a secondary analysis of data from 3 randomized clinical trials; C-ASSERT (clinicaltrials.gov NCT03002012), ORCAS/ACACIA (NCT03945448), and the ENCORE (NCT05085171) trials conducted in Uganda between November 2017 and August 2024. In this analysis, we included adult (≥18 years) outpatient participants with advanced HIV who were plasma CrAg positive with an LP performed and cerebrospinal fluid (CSF) CrAg result. All participants had clinical assessment for symptoms of meningitis within 7 days of the LP. These included presence of headache, fever, photophobia, visual changes, seizures, confusion, mania, and Glasgow Coma Scale < 15. All CrAg testing (CSF and plasma) was performed using the CrAg lateral flow assay (LFA) (Immy, Norman, OK).
Study Variables
The primary outcome of interest was a CSF CrAg-positive result indicating cryptococcal meningitis. Baseline characteristics of interest include symptoms presentation, specifically presence of headache, neck stiffness, fever, confusion, visual disturbances, and focal neurologic deficits. Additionally, baseline CD4 cell count, plasma CrAg titer, antiretroviral therapy (ART) status (naive or experienced) and duration on ART were summarized. Baseline laboratory values were collected including serum creatinine, sodium, potassium, hemoglobin, and platelet count.
Statistical Analysis
Baseline characteristics and laboratory characteristics were summarized for the overall cohort, as well as by CSF CrAg test results. Continuous variables were summarized using medians and interquartile ranges (IQR). Categorical variables, including presence of signs and symptoms, were summarized using frequencies and percentages. Statistical comparisons between the CSF CrAg-positive and CSF CrAg-negative groups were made using the Kruskal-Wallis test for medians and chi-squared test or Fisher exact test for proportions. CrAg titer was categorized using a cutoff of 1:160, based on prior evidence showing that patients with a titer of 1:≥160 have a 3-fold increased risk of death than those with low titers (<1:160) [9, 10]. The overall distribution of each meningeal sign and symptom was summarized.
For symptoms that were associated with CSF CrAg status in the univariate categorical analysis with a P value less than a prespecified cutoff 0.10, unadjusted and adjusted odds ratios were obtained via univariate and multivariable logistic regression models to evaluate the magnitude of their association with positive CSF CrAg results. Baseline characteristics and clinical variables were adjusted in the multivariable models to account for confounding. Model selection for the full multivariable model was conducted via a backward stepwise algorithm based on Akaike Information Criterion. Areas under the receiver operating characteristic curves (AUROC) were reported to evaluate the discriminating ability of the signs and symptoms for positive CSF CrAg results. DeLong's method was used to compare ROC curves from different models and to construct confidence intervals for the AUC statistics.
Continuous variables with missing values were imputed with the medians of the complete data. As sensitivity analysis, we used the Multiple Imputation by Chained Equations. Using the mice package in R [11], we generated 15 complete data sets. Then a logistic regression for the predicting positive LP was performed on each of the 15 complete datasets. The area under the curve (AUC) for each model was calculated. The resulting odds ratio estimates, AUC values, and their associated variances were then pooled using Rubin's rules [12]. The final pooled AUC estimate was then used to generate the presented performance ROC plot.
To assess the accuracy and performance of the logistic regression models, the dataset was randomly partitioned into training and testing sets at a 4:1 ratio. A model was fitted to the training set to obtain model estimates, and the optimal probability cutoff was determined using the threshold that maximized the Youden Index. The resulting model and probability cutoff was then applied to the test set. Using data from the test set, calibration plots with calibration intercepts and slopes were generated using R package CalibrationCurves [13, 14]. An additional ROC curve was also constructed only using the test dataset. Positive predictive value and negative predictive value of the optimal probability cutoff was assessed over outcome prevalences using Bayes’ Rule [15]. A classification tree was constructed using the Classification And Regression Tree algorithm with the rpart R package in R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria) [16]. The dataset was partitioned into a training set and a test set, with an 80% to 20% ratio. The classification tree was first fitted on the training set, where the default 10-fold cross-validation error was used for model pruning and to protect against overfitting. After the final pruned model was selected, the independent test set was then used to calculate the misclassification rate. Additional model calibrations and evaluations were also conducted on the test set.
Ethical Considerations
The clinical trials from which data for this study was extracted conformed to the U.S. and international standards of Good Clinical Practice, the Declaration of Helsinki, and international ethical guidelines for biomedical research involving human subjects. They were also conducted in compliance with the relevant government regulations for Uganda, the United States, and international and institutional research policies and procedures. All study protocols were approved by relevant research and ethics committees, the Uganda National Council for Science and Technology, Uganda National Drug Authority, and the University of Minnesota. All participants provided written informed consent before enrollment into the studies and the funder had no role in the study conduct or data analysis. Study data were accessible to all the authors of this study.
RESULTS
Of 365 serum CrAg-positive participants who had CSF CrAg testing performed, 344 had complete data for the presence or absence of symptoms of meningitis within 7 days of lumbar puncture and were included in this analysis. The median age of participants was 36 years (IQR 30, 41), and 45% were female (Table 1). Overall, 65% were ART-naive, and the median CD4 cell count was 33 cells/µL (IQR 16, 68). The median CrAg titer was 1:1280 (IQR 1:100, 1:2560). Headache was the most common presenting symptom (83%), followed by fever (35%), stiff neck (33%), photophobia (23%), and confusion (14%) (Supplementary Figure 1). Baseline characteristics of participants who were excluded are summarized in Supplementary Table 1.
Overall, 60% (205/344) of participants were CSF CrAg-positive. Among CSF CrAg-positive participants, the median plasma CrAg titer was 1:2560 (IQR 1:640, 1:2560), whereas among CSF CrAg-negative participants, the median plasma CrAg titer was 1:80 (IQR 1:20, 1:640) (Table 1). Participants who were CSF CrAg-positive were more likely to report a baseline headache (95% vs 65%, P < .001), stiff neck (46% vs 15%, P < .001), photophobia (31% vs 11%, P < .001), or confusion (17% vs 10%, P = .04). All 4 symptoms were positively associated with CSF CrAg-positive status in both the univariate model and multivariable logistic regression models, indicating that presence of any of these symptoms would increase the odds of having a CSF CrAg-positive result (Table 2).
Univariate AUC statistics of headache alone was 0.65 (95% confidence interval [CI], .61–.69), indicating that the predictive accuracy of headache alone for a positive CSF CrAg result was poor; headache was 95% sensitive and only 35% specific for predicting meningitis. However, the overall AUC increased to 0.78 (95% CI, .74–.82) when all four symptoms (headache, neck stiffness, photophobia, confusion) were combined in a multivariable model (DeLong's test P value < .001) (Figure 1). The AUC was further improved to 0.86 (95% CI, .82–.90) when additional clinical characteristics of male sex and CrAg titer ≥1:160 were included in the model.
ROC curves for univariate analysis along with full model. Area under the receiver operating characteristic curves (AUROC) for univariate along with multivariate analysis. Headache has the highest sensitivity of about 0.95 and lowest specificity of about 0.36. Other symptoms when considered in isolation are less sensitive but highly specific for meningitis. A combination of all 4 symptoms increases the specificity compared to headache alone. The full model further increases the specificity at the same sensitivity of headache alone.
The variables used in the full multivariable logistic regression model were further evaluated using a classification tree. The final pruned model, with a misclassification rate of 0.21, consists of 2 splits, with the first split by plasma CrAg titer status and the second split of headache among those with high plasma CrAg titer (Figure 2). Participants who had high plasma CrAg titer ≥1:160 and headache had a 79% probability of a CSF CrAg-positive result in the final pruned model compared to the 18% probability for participants who had headache and a low CrAg titer ≤1:160.
Classification tree for full model. The final pruned model, with a misclassification rate of 0.21, consists of 2 splits, with the first split by plasma CrAg titer status and second split by headache among participants with high plasma CrAg titer. Participants who had both high plasma CrAg titer and headache, which consists of 67% of the cohort, had the highest probability (79%) for having a CSF CrAg-positive result in the final pruned model, whereas the probability for having a CSF CrAg-positive result is only 13% and 33% in the other 2 groups. +LP in the figure denotes CSF CrAg-positive.
Participants with a positive CSF CrAg had lower serum sodium levels (hyponatremia) compared to those who had a negative CSF CrAg. There were no significant differences in other laboratory findings among the two populations. Please see Supplementary Figures 2–9 for results from multiple imputation analysis, calibration plots, and model valuations.
DISCUSSION
We assessed the predictive value of meningeal symptoms for cryptococcal meningitis in an ambulatory population with symptomatic cryptococcal antigenemia. In our cohort, where 60% of participants had meningitis (CSF CrAg-positive), headache was the most common presenting symptom. Having a combination of headache, stiff neck, photophobia, confusion, male sex, and CrAg titer ≥1:160 demonstrated the highest AUC. A combination of headache and CrAg titer ≥1:160 demonstrated a 79% probability of meningitis using a classification tree.
Similar to our study findings, a study conducted at 2 national referral hospitals in Uganda indicated that 56% of people with HIV-associated cryptococcal antigenemia had meningitis [17], although this study was conducted in an inpatient population. Headache is a common complaint prompting people to seek medical care [18]; it is also one of the most frequent symptoms of cryptococcal meningitis with prevalence above 75% [18–20]. This is consistent with the current study that identified headache in 83% of participants. Despite the high sensitivity of headache for predicting cryptococcal meningitis, headache alone is nonspecific for predicting meningitis [21].
The addition of stiff neck, photophobia, and confusion increased the specificity of headache and improved the overall AUC. When compared to the univariate headache model, the improvement in the AUC of the full model, which includes symptoms, male sex, and CrAg titer ≥1:160, was greatly attributed to the improved specificity from about 0.36 to 0.60 at the threshold that leads to the same 0.95 sensitivity. The combination of headache and high plasma CrAg titer had the highest probability of finding a positive CSF CrAg in our study, according to the classification tree model. This is consistent with findings by Wake and colleagues that suggested that a combination of headache and high blood CrAg titer highly predict a positive CSF CrAg [8]. In addition, high plasma CrAg titer alone has been associated with a positive CSF CrAg and death among those with a positive plasma CrAg [22, 23].
CrAg titers can be determined by a serial dilution technique using CrAg LFA, a process that requires technical expertise and with a relative long turnaround time for clinical decision making [24]. A rapid, point-of-care CrAg semiquantitative LFA presents a cost-effective alternative with the ability to determine CrAg titers in real time [25]. However, both methods of plasma CrAg titer determination are still widely inaccessible and may only be available in clinical trial settings, which presents a challenge in ambulatory HIV care settings where most patients with cryptococcal antigenemia initially present. Where CrAg titers are unavailable, clinicians should consider presence of the 4 symptoms (ie, headache, neck stiffness, photophobia, and confusion) to inform their decision to perform a lumbar puncture for those with a positive plasma CrAg, rather than considering headache in isolation.
In our study, participants with a positive CSF CrAg had lower serum sodium levels (hyponatremia) compared to those who had a negative CSF CrAg. Hyponatremia has been reported as a predictor of Cryptococcal meningitis and death among asymptomatic persons with Cryptococcal antigenemia and should inform clinicians of the increased risk of morbidity and mortality in this ambulatory population [26].
Limitations of our analysis are related to the retrospective nature of this study. We included participants enrolled in clinical trials, which excludes those who were too sick for study participation. Additionally, we included only participants who had lumbar punctures performed; those who declined or who died before having an LP were excluded from the study. This resulted in an unusually high prevalence of meningitis (60%), which limits generalizability of our findings. Furthermore, asymptomatic CrAg-positive participants were also excluded. Additionally, headache is a subjective experience, and reporting is dependent on multiple factors, including severity, presence of other symptoms, manner of asking, and documentation. It is therefore difficult to ascertain whether the reported absence of headache in individuals with symptoms like neck stiffness, photophobia, or confusion can be relied on.
In summary, headache alone is a nonspecific predictor of meningitis in persons with cryptococcal antigenemia in the outpatient setting. The presence of both headache and a high CrAg titer serves as the most reliable predictor for meningitis. In the absence of plasma CrAg titration, clinicians should consider a combination of symptoms such as headache, stiff neck, photophobia, and confusion, along with male sex, when deciding which patients to prioritize to perform a lumbar puncture to exclude cryptococcal meningitis among individuals with cryptococcal antigenemia.
Supplementary Material
ofag027_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rajasingham R, Govender NP, Jordan A, et al The global burden of HIV-associated cryptococcal infection in adults in 2020: a modelling analysis. Lancet Infect Dis 2022; 22:1748–55.36049486 10.1016/S 1473-3099(22)00499-6PMC 9701154 · doi ↗ · pubmed ↗
- 2Levin AE, Bangdiwala AS, Nalintya E, et al Outpatient cryptococcal antigen screening is associated with favorable baseline characteristics and improved survival in persons with cryptococcal meningitis in Uganda. Clin Infect Dis 2023; 76:e 759–65.35859045 10.1093/cid/ciac 599PMC 10169421 · doi ↗ · pubmed ↗
- 3Organization WH . Guidelines for diagnosing, preventing and managing cryptococcal disease among adults, adolescents and children living with HIV. World Health Organization, Geneva, Switzerland. 2022.35797432 · pubmed ↗
- 4Govender NP, Meintjes G, Mangena P, et al Southern African HIV Clinicians Society guideline for the prevention, diagnosis and management of cryptococcal disease among HIV-infected persons: 2019 update. South Afr J HIV Med 2019; 20:1–16.10.4102/sajhivmed.v 20i 1.1030 PMC 708162532201629 · doi ↗ · pubmed ↗
- 5Lofgren S, Abassi M, Rhein J, Boulware DR. Recent advances in AIDS-related cryptococcal meningitis treatment with an emphasis on resource limited settings. Expert Rev Anti Infect Ther 2017; 15:331–40.28111998 10.1080/14787210.2017.1285697 PMC 5602588 · doi ↗ · pubmed ↗
- 6Nalintya E, Meya DB, Lofgren S, Hullsiek KH, Boulware DR, Rajasingham R. A prospective evaluation of a multisite cryptococcal screening and treatment program in HIV clinics in Uganda. J Acquir Immune Defic Syndr 2018; 78:231–8.29509588 10.1097/QAI.0000000000001669 PMC 5953806 · doi ↗ · pubmed ↗
- 7Jarvis JN, Tenforde MW, Lechiile K, et al Evaluation of a novel semiquantitative cryptococcal antigen lateral flow assay in patients with advanced HIV disease. J Clin Microbiol 2020; 58.10.1128/JCM.00441-20PMC 744866232461286 · doi ↗ · pubmed ↗
- 8Wake RM, Britz E, Sriruttan C, et al High cryptococcal antigen titers in blood are predictive of subclinical cryptococcal meningitis among human immunodeficiency virus-infected patients. Clin Infect Dis 2018; 66:686–92.29028998 10.1093/cid/cix 872PMC 6220350 · doi ↗ · pubmed ↗