Evaluation and analysis of tear fluid volume and surgical outcomes for lacrimal punctum obstructive diseases using anterior segment OCT
Zheng Zhang, Qing Ye

TL;DR
This study shows that anterior segment OCT can effectively measure tear fluid changes and predict successful outcomes after surgery for tear duct blockages.
Contribution
The study introduces AS-OCT as a reliable, non-invasive tool for evaluating tear dynamics and surgical success in punctal obstructive diseases.
Findings
AS-OCT showed significant reductions in tear meniscus height and volume after surgery.
Symptom improvement correlated strongly with objective tear meniscus volume reduction.
82.7% of patients achieved functional success and 88.5% achieved anatomical patency at 6 months.
Abstract
Lacrimal punctum obstructive diseases are a frequent cause of persistent epiphora, leading to discomfort, impaired quality of life, and repeated clinic visits. Accurate and objective assessment of tear dynamics is essential for diagnosis and evaluation of surgical outcomes. To evaluate tear fluid volume using anterior segment optical coherence tomography (AS-OCT) and correlate these objective parameters with surgical outcomes in patients undergoing procedures for punctal obstruction. Fifty-two eyes from 34 patients with punctal stenosis or occlusion were evaluated with baseline symptom assessment (Munk score), fluorescein dye disappearance test (FDDT), and AS-OCT imaging of the lower tear meniscus (height, area, volume). Patients underwent snip punctoplastyS, Kelly-punch punctoplasty, or punctal dilatation with intubation. Follow-up assessments were performed at 1, 3, and 6 months…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
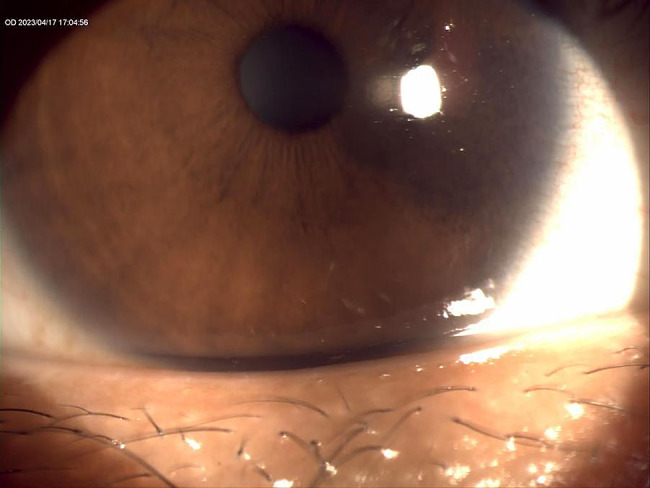 Figure 1
Figure 1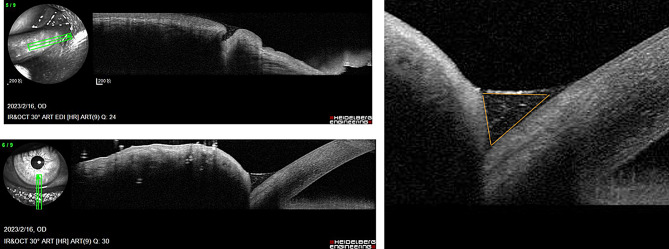 Figure 2
Figure 2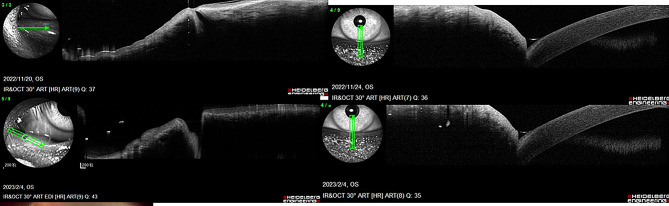 Figure 3
Figure 3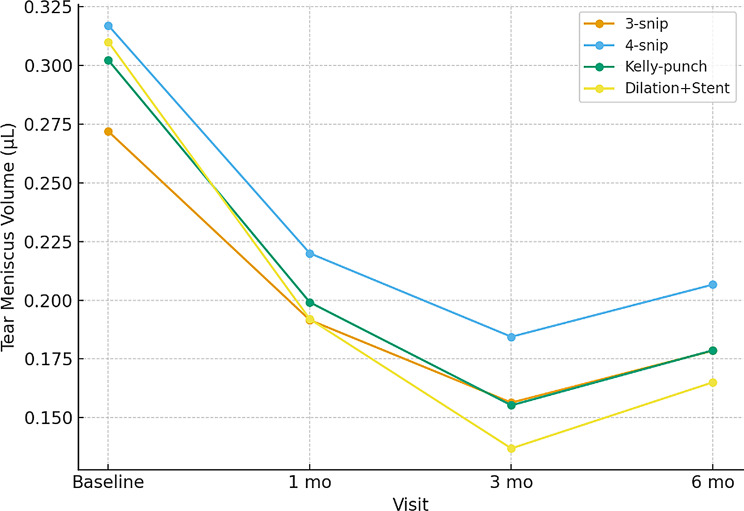 Figure 4
Figure 4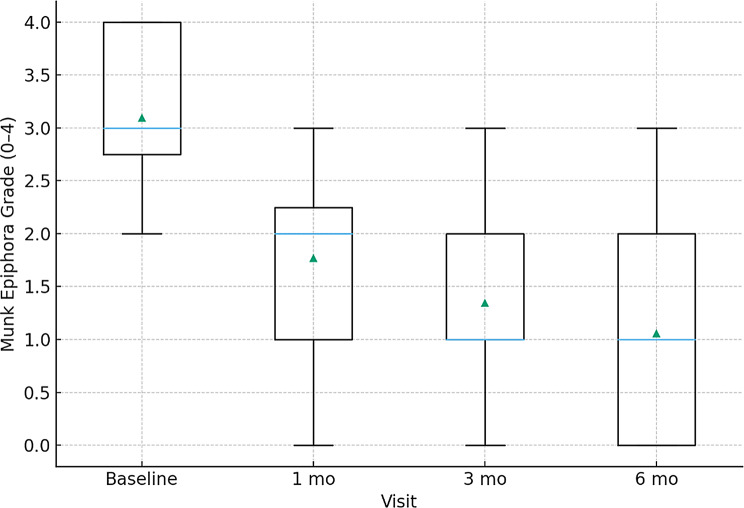 Figure 5
Figure 5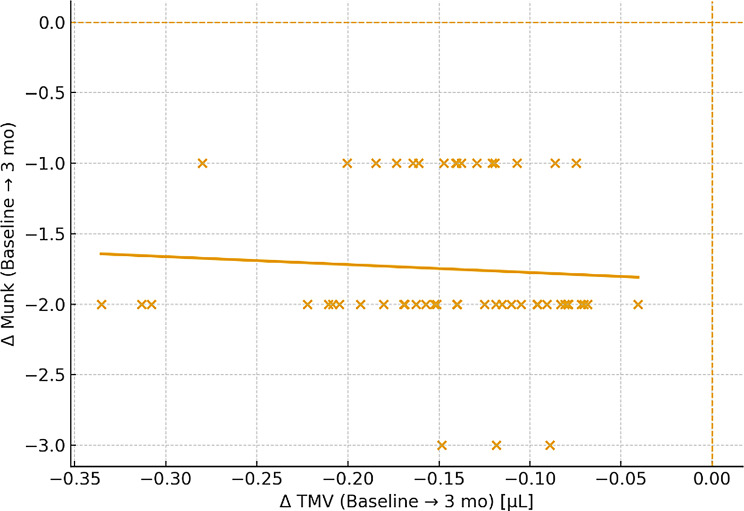 Figure 6
Figure 6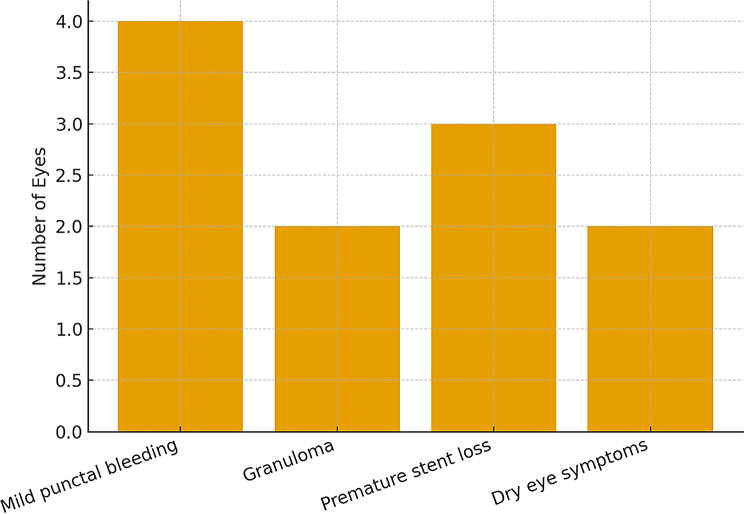 Figure 7
Figure 7- —Clinical research on the diagnosis of lacrimal punctum diseases using anterior segment OCT
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNasolacrimal Duct Obstruction Treatments · Ocular Surface and Contact Lens · Glaucoma and retinal disorders
Introduction
Epiphora, the persistent overflow of tears onto the face, is a symptom that appears deceptively simple yet carries a substantial burden on patients and healthcare providers. Among its diverse etiologies, obstruction at the level of the lacrimal punctum is increasingly recognised as a leading cause, particularly in middle-aged and elderly populations [1–3]. The lacrimal puncta are minute but critical gateways to the tear drainage system; any narrowing, membranous occlusion, or acquired stenosis can compromise tear outflow, leading to chronic tearing, ocular irritation, and frequent clinic visits (Fig. 1). For many patients, this condition results not only in functional impairment but also in psychosocial distress due to constant tearing, cosmetic dissatisfaction, and reduced quality of life [4–6].
Fig. 1. Slit-lamp photograph of the right eye showing the lower punctal region with tear meniscus elevation suggestive of punctal obstruction. The anterior segment image illustrates the pooling of tears along the lid margin, corresponding clinically to symptomatic epiphora
Historically, the diagnosis and management of punctal obstruction relied on clinical inspection and simple functional tests. While these methods remain valuable, they are often limited in precision, and do not provide an objective quantification of the tear burden [7]. The growing demand for measurable endpoints in ophthalmology has, therefore, shifted attention to modern imaging tools. Anterior segment optical coherence tomography (AS-OCT), widely used in corneal and angle assessment, has recently emerged as a non-invasive, high-resolution modality capable of quantifying tear meniscus parameters such as height, area, and volume. These parameters directly reflect tear fluid dynamics and can act as surrogate biomarkers for lacrimal drainage efficiency.
Although several previous studies have quantified tear meniscus parameters using AS-OCT in punctal stenosis, our work differs by integrating quantitative tear volume analysis with surgical outcome stratification across three different punctal procedures and by identifying baseline TMV > 0.35 µL as a predictor of functional success. This dual imaging–clinical correlation has not been systematically reported before.
Obstructive diseases of the lacrimal punctum are not rare. Studies suggest that punctal stenosis contributes to up to 30% of patients presenting with symptomatic epiphora in tertiary clinics. Prevalence varies geographically, influenced by environmental exposure, ageing demographics, chronic blepharitis, and inflammatory ocular surface disease. In countries with larger ageing populations, the burden is expected to rise substantially, mirroring trends seen in other chronic ocular surface conditions [2–6]. The socioeconomic impact extends beyond direct medical expenses; patients often report loss of productivity, social embarrassment, and repeated expenditure on lubricants or antibiotics due to associated conjunctival irritation.
Global healthcare systems are increasingly attentive to the burden of chronic ophthalmic conditions, yet punctal obstruction remains underrepresented in epidemiological research. Unlike cataract or glaucoma, which have well-established registries and global initiatives, punctal disease is often overlooked, despite its high prevalence and quality-of-life implications. As with chronic wounds in dermatology, this condition represents a “silent epidemic”: under-reported, yet significant in terms of personal discomfort and cumulative healthcare costs [4–9].
The lacrimal puncta are delicate openings positioned at the medial lid margin, bordered by a complex fibrovascular and epithelial structure. Obstruction can be primary, often due to age-related epithelial hyperkeratinisation and fibrosis, or secondary to inflammatory and infectious causes. Blepharitis, trachoma, cicatrising conjunctivitis, chronic use of topical medications, and dermatological conditions such as Stevens–Johnson syndrome can precipitate narrowing or occlusion [10].
Histopathological studies reveal that stenotic puncta show squamous metaplasia, epithelial overgrowth, subepithelial fibrosis, and loss of normal elastic tissue, leading to functional impairment [11]. Over time, the compromised punctum fails to drain tears efficiently, leading to tear stasis, secondary infections, and exacerbation of ocular surface inflammation. This cyclical process mirrors the “hard-to-heal” nature of chronic wounds, where initial insult perpetuates a self-sustaining pathological state that becomes difficult to reverse without intervention.
Traditional diagnostic approaches include slit-lamp inspection, dye disappearance tests (FDDT), and syringing. These methods provide qualitative or semi-quantitative information. However, their reproducibility is limited, and inter-observer variability is high. For example, the FDDT is influenced by environmental lighting, blink rate, and observer experience. While simple and inexpensive, such tools are often inadequate in differentiating subtle cases or in objectively documenting improvement following surgery [12–15].
AS-OCT has transformed this landscape by enabling reproducible measurement of tear meniscus height (TMH), tear meniscus area (TMA), and derived tear meniscus volume (TMV). These parameters correlate strongly with tear film stability and outflow function. Unlike invasive techniques, AS-OCT imaging is rapid, requires minimal patient cooperation, and provides quantifiable outcomes that can be tracked longitudinally. Literature from Kim et al. demonstrated that after 4-snip punctoplasty, TMH decreased from 452 μm preoperatively to 362 μm at six months, paralleling symptomatic improvement. Abdallah et al. similarly showed a reduction from 325 μm to 205 μm after punctal plug insertion, with corresponding improvement in Munk epiphora scores. These studies highlight the clinical utility of AS-OCT metrics as both diagnostic and outcome tools [13–16].
Multiple surgical techniques exist for the management of punctal stenosis, including the traditional 3- or 4-snip punctoplasty, Kelly-punch punctoplasty, and punctal dilatation with monocanalicular stenting. Functional and anatomical success rates often exceed 80–90%, but recurrence and restenosis remain concerns. Long-term follow-up reveals variability in outcomes, influenced by surgical technique, adjunctive use of stents or mitomycin-C, and baseline patient characteristics [17].
Despite these generally high success rates, the lack of objective outcome measures has limited comparative effectiveness research. Most series report “anatomical patency” or “symptomatic relief” as endpoints, both of which are subject to bias. By introducing AS-OCT–derived metrics into outcome evaluation, clinicians gain a reproducible, quantifiable, and patient-relevant endpoint. Such integration mirrors broader trends in ophthalmology, where imaging-based endpoints (e.g., OCT in macular diseases) have revolutionised treatment monitoring.
The burden of punctal obstruction extends beyond clinical symptoms. Patients frequently report embarrassment in professional and social interactions due to constant tearing. Chronic tearing can impair reading, driving, and outdoor activities, especially in windy or cold climates. Repeated healthcare visits, coupled with frequent use of artificial tears or topical medications, generate ongoing costs for patients and healthcare systems alike [18–20].
From a socioeconomic perspective, the parallels with chronic wound care are striking. As highlighted in wound epidemiology, the “hidden costs” of disease often exceed direct treatment expenses, encompassing lost productivity, caregiver burden, and psychological strain. In resource-limited settings, the impact is magnified by poor access to surgical services, lack of trained ophthalmic surgeons, and limited availability of advanced diagnostic tools like OCT. This underscores the need for affordable, accessible technologies that can be integrated into standard care [21].
The current study is built on the premise that modern imaging can bridge critical diagnostic and evaluative gaps in the management of lacrimal punctum obstructive diseases. By quantifying tear meniscus parameters pre- and post-surgery, AS-OCT provides an objective measure of treatment efficacy. Correlating these parameters with subjective symptom scales (Munk score) and functional tests (FDDT) creates a comprehensive assessment framework that is clinically meaningful and scientifically rigorous.
This approach aligns with the global movement towards evidence-based, data-driven medicine, where objective metrics complement clinical judgment. Just as wound registries and cost analyses have reshaped chronic wound care policy, integrating AS-OCT into lacrimal practice can standardise outcome reporting, facilitate comparative studies, and strengthen patient counselling.
Materials and methods
Study design and setting
This was a prospective observational cohort study conducted at the Department of Ophthalmology. Ethical approval was obtained from the institutional review board, and the study adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from all participants prior to enrolment.
Eligibility criteria
Inclusion criteria were:
- Adults (≥ 18 years) presenting with symptomatic epiphora.
- Clinical evidence of primary punctal stenosis or occlusion (membranous or acquired narrowing).
- Baseline Munk score ≥ 2.
- Positive fluorescein dye disappearance test (FDDT ≥ grade 2).
Exclusion criteria included:
- Secondary punctal obstruction due to trauma, tumour, or previous surgery.
- Concomitant canalicular or nasolacrimal duct obstruction (ruled out by syringing).
- Cicatrising ocular surface disease (e.g., Stevens–Johnson syndrome, ocular cicatricial pemphigoid).
- Significant dry eye disease requiring primary treatment.
- Contact lens wear within the preceding 72 h.
Baseline assessment
All patients underwent comprehensive ophthalmic evaluation, including visual acuity, slit-lamp biomicroscopy, and eyelid margin inspection. Symptom severity was graded using the Munk epiphora scale (0–4). Functional patency was assessed with the FDDT, scored from 0 (normal clearance) to 3 (severe retention).
Anterior segment OCT imaging
Tear meniscus imaging was performed with a spectral-domain AS-OCT system. Scans were obtained in a standardized setting under ambient room illumination, with the patient in primary gaze, avoiding manipulation of the eyelids. For each eye, three high-quality scans were captured, and the best image was analysed. TMH and TMA were measured at the central lower eyelid directly inferior to the corneal apex, which corresponds to the most stable segment of the meniscus. Three consecutive horizontal scans (nasal, central, temporal) were obtained; only central values were analyzed to maintain consistency, as prior reports confirm minimal inter-segment variability [13, 20].
Measured parameters included:
- Tear Meniscus Height (TMH): vertical distance from the lower lid margin to the apex of the meniscus.
- Tear Meniscus Area (TMA): cross-sectional polygonal area of the tear meniscus.
- Tear Meniscus Volume (TMV): calculated as TMA × lid length imaged (~ 8–10 mm). TMV was computed as TMA × a fixed 10 mm lid length, consistent with convention in previous AS-OCT studies [13, 31]. It is worth noting that the actual horizontal extent of the functional tear reservoir may differ between individuals based on palpebral fissure width, age, sex, or ethnicity.
Two independent observers analysed OCT images to evaluate inter-grader reproducibility.
Surgical interventions
Surgical procedure was determined by surgeon preference and punctal anatomy:
- Rectangular 3- or 4-snip punctoplasty with mucosal marsupialization.
- Kelly-punch punctoplasty, performed using standardized punch forceps.
- Punctal dilation with monocanalicular intubation (Mini-Monoka stent).
In selected cases, adjunctive measures such as mitomycin-C 0.02% or temporary stenting were used.
Postoperative follow-up
Patients were examined at 1 month, 3 months, and 6 months postoperatively. Follow-up assessments included:
- Symptom evaluation (Munk grading).
- Functional testing (FDDT).
- OCT tear meniscus parameters (TMH, TMA, TMV).
- Anatomical patency confirmed by slit-lamp examination and irrigation.
Outcome definitions
- Anatomical success: patent punctum on irrigation without restenosis.
- Functional success: improvement by ≥ 1 grade in Munk scale and FDDT ≤ grade 1.
Statistical analysis
All analyses were performed using SPSS (IBM Corp., Armonk, NY) and R. Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range), while categorical variables were reported as frequencies and percentages.
- Changes in OCT parameters across visits were compared using paired t-tests or Wilcoxon signed-rank tests as appropriate.
- Associations between ΔTMV and ΔMunk /FDDT were assessed with Spearman’s correlation.
- Predictors of functional success at 6 months were evaluated using multivariable logistic regression.
- Interobserver reliability for OCT measurements was assessed with intraclass correlation coefficients (ICC).
A P value < 0.05 was considered statistically significant.
Results
Cohort characteristics
A total of 52 eyes from 34 patients (mean age 56.7 ± 11.2 years; 61.5% female) were included. Bilateral disease was present in 18 patients (52.9%). Primary punctal stenosis accounted for 76.9% of eyes, while complete membranous occlusion was observed in 23.1%.Table 1 summarises baseline demographic and clinical features. AS-OCT images of the lower tear meniscus in the right eye were shown in Fig. 2.
Table 1. Baseline characteristics of the study cohortVariableOverall (n = 52 eyes)Age, years (mean ± SD)56.7 ± 11.2Female, n (%)32 (61.5%)Laterality (Right/Left)26/26Diagnosis: stenosis/occlusion, n (%)40 (76.9) / 12 (23.1)Munk grade (median [IQR])3 [2–4]2-FDDT grade (median [IQR])2 [1–3]TMH (µm), mean ± SD0.45 ± 0.12TMA (mm²), mean ± SD0.030 ± 0.010TMV (µL), mean ± SD0.32 ± 0.15
Fig. 2AS-OC) images of the lower tear meniscus in the right eye. (Left panels) Cross-sectional scans acquired at the lower eyelid margin demonstrate elevation of the tear meniscus. (Right panel) Quantitative measurement of tear meniscus area outlined in orange, representing the tear fluid reservoir adjacent to the punctum
Surgical distribution
Procedures included rectangular 3- or 4-snip punctoplasty (38.4%), Kelly-punch punctoplasty (32.7%), and punctal dilatation with Mini-Monoka stenting (28.8%) (Table 2). AS-OCT was used to measure the punctal diameter and depth before and after surgery as shown in Fig. 3. Punctal diameter and depth measurements were exploratory and confirmed anatomical enlargement post-surgery; these were not included in regression analysis but visually demonstrate structural change.
Table 2. Surgical techniques and adjunctive measuresProcedureEyes n (%)Stented n (%)MMC used n (%)Rectangular 3-snip10 (19.2)4 (40.0)2 (20.0)Rectangular 4-snip10 (19.2)5 (50.0)2 (20.0)Kelly-punch punctoplasty17 (32.7)8 (47.0)2 (11.8)Dilation + Mini-Monoka15 (28.8)15 (100.0)—
Fig. 3. Anterior segment OCT was used to measure the punctal diameter and depth before and after surgery
Tear meniscus changes
Tear meniscus parameters showed significant reduction postoperatively (Table 3; Fig. 4). The greatest decline occurred within the first month, with stabilisation by the third month.
Table 3. Tear meniscus metrics over timeMetricBaseline1 month3 months6 monthsP (trend)TMH (µm)0.45 ± 0.120.32 ± 0.100.29 ± 0.090.30 ± 0.10< 0.001TMA (mm²)0.030 ± 0.0100.021 ± 0.0080.019 ± 0.0070.020 ± 0.008< 0.001TMV (µL)0.32 ± 0.150.22 ± 0.110.19 ± 0.100.20 ± 0.10< 0.001
Fig. 4TMV over time by surgical technique
Symptom and functional outcomes
Symptom burden (Munk scale) and functional patency (FDDT) both improved significantly (Table 4; Fig. 5). At 6 months, 82.7% achieved functional success and 88.5% achieved anatomical patency (Tables 5 and 6).
Table 4. Symptom and functional outcomesOutcomeBaseline1 month3 months6 monthsMunk grade (median [IQR])3 [2–4]1 [0–2]1 [0–1]1 [0–1]FDDT grade (median [IQR])2 [1–3]1 [0–2]0 [0–1]0 [0–1]Functional success, %—65.480.882.7Anatomical patency, %—76.984.688.5
Fig. 5. Symptom burden (Munk Grade) over time
Table 5. Predictors of functional success (Multivariable logistic Regression)PredictorAdjusted OR (95% CI) P Age (per decade)1.12 (0.89–1.43)0.31Female sex1.28 (0.60–2.75)0.52Baseline TMV > 0.35 µL2.45 (1.15–5.22)0.0214-snip vs. Kelly-punch1.31 (0.55–3.12)0.48Stent use2.89 (1.22–6.84)0.015
Table 6. Postoperative complicationsComplicationEyes n (%)ManagementMild punctal bleeding4 (7.7)ConservativeGranuloma formation2 (3.8)Excision/steroid dropsPremature stent loss3 (5.8)Re-intubation (2), observation (1)Dry eye symptoms2 (3.8)Lubricants
Correlations and predictors
Multivariable logistic regression identified baseline tear meniscus volume (TMV) and stent use as significant predictors of functional success. Eyes with TMV > 0.35 µL had 2.5-fold higher odds of achieving symptomatic and functional improvement (OR 2.45, 95% CI 1.15–5.22, P = 0.021), reflecting greater potential benefit when excess tear burden was present. Similarly, stenting nearly tripled the likelihood of success (OR 2.89, 95% CI 1.22–6.84, P = 0.015), likely by maintaining punctal patency during healing. In contrast, age, sex, and surgical technique (4-snip vs. Kelly-punch) were not independently associated with outcomes, underscoring that baseline tear dynamics and adjunctive measures are key determinants of prognosis. Variables with P < 0.10 on univariate analysis and those of clinical relevance (age, sex, baseline TMV, surgical type, stent use) were entered into the multivariable model after collinearity assessment (VIF < 2) (Figs. 6 and 7).
Fig. 6. Relationship between change in TMV and change in Munk score
Fig. 7. Postoperative complication profile
Complications
Postoperative complications were infrequent and minor across the study cohort. Mild punctal bleeding occurred in 4 eyes (7.7%) and resolved with conservative management. Granuloma formation was noted in 2 eyes (3.8%) and successfully treated with excision or topical steroids. Premature stent loss was observed in 3 eyes (5.8%), requiring re-intubation in 2 cases, while 1 was managed conservatively without adverse effect. Dry eye symptoms developed in 2 eyes (3.8%) and were relieved with lubricants. Importantly, no canalicular injuries, infections, or vision-threatening events occurred, highlighting that punctal surgery is a safe procedure with manageable postoperative risks and favorable outcomes.
Discussion
This study demonstrates that anterior segment optical coherence tomography (AS-OCT) provides an objective and reproducible method for evaluating surgical outcomes in patients with lacrimal punctum obstructive disease. Our findings confirm that tear meniscus parameters, including height, area, and volume, show significant postoperative reduction, which closely parallels improvements in symptom burden and functional tear clearance.
At baseline, the mean tear meniscus height (TMH) was 0.45 ± 0.12 mm, which decreased significantly to 0.30 ± 0.10 mm at 6 months after surgery (P < 0.001). Similarly, tear meniscus volume (TMV) declined from 0.32 ± 0.15 µL preoperatively to 0.20 ± 0.10 µL at 6 months. These reductions occurred predominantly within the first postoperative month and stabilized by 3 months, suggesting that surgical improvement in tear drainage is both rapid and sustained. Symptom scores showed parallel improvement: median Munk grade decreased from 3 [IQR 2–4] at baseline to 1 [0–1] at 6 months, and functional patency (FDDT ≤ 1) was achieved in 82.7% of eyes. Anatomical patency rates were similarly high, with 88.5% remaining patent at 6 months. Unlike earlier studies that reported descriptive TMH/TMA changes, this work integrates volumetric analysis, identifies predictive baseline TMV thresholds, and provides procedure-stratified outcomes, thus extending prior findings into prognostic and clinical domains.
Importantly, reductions in TMV correlated strongly with improvements in symptoms and functional outcomes (Spearman r = 0.68 for Munk score, r = 0.62 for FDDT; both P < 0.001). This supports the concept that excess tear fluid burden, as quantified by OCT, is a key determinant of patient discomfort and functional impairment. In multivariable analysis, higher baseline TMV (> 0.35 µL) and use of adjunctive stenting were independent predictors of functional success, highlighting potential markers for surgical planning and prognosis.
Our results are consistent with previously published international studies. Some of the previous research reported a reduction in TMH from 452 μm to 362 μm following four-snip punctoplasty, with a functional success rate of 93% [22–25]. The previous conducted research studies showed similarly observed a decrease in TMH from 325 μm to 205 μm after punctal plug implantation, with corresponding improvement in Munk scores [26–30]. While the absolute baseline values in our cohort (450 μm → 300 μm) were somewhat higher, the relative degree of reduction and functional improvement are comparable, reinforcing the validity and reproducibility of AS-OCT measurements across different populations and interventions [31–33].
The clinical relevance of objective imaging cannot be overstated [34]. Traditional endpoints in punctal surgery have relied heavily on subjective symptom reporting or anatomical patency on irrigation [35]. While useful, these assessments are prone to variability and do not always reflect true functional success. By integrating AS-OCT, clinicians can provide measurable, quantitative evidence of improved tear clearance, offering both scientific rigor and reassurance to patients [36]. This parallels the transformation seen in retinal diseases, where OCT has become indispensable in objectively monitoring therapeutic response.
Different surgical techniques were used in our cohort, including snip punctoplasty, Kelly-punch punctoplasty, and punctal dilatation with intubation [37–40]. All yielded satisfactory outcomes, but the adjunctive use of stenting was associated with greater likelihood of functional success, particularly in severe or membranous cases. This suggests that stenting may play a protective role against early restenosis by maintaining lumen patency during the healing process [40–45]. Future studies with larger cohorts and randomized comparisons are needed to determine whether stenting should be routinely recommended in high-risk cases. A baseline TMV >0.35 µL may identify patients most likely to benefit from punctal surgery, while postoperative TMV ≤ 0.20 µL may represent successful tear clearance. AS-OCT could complement or partially replace FDDT in follow-up, especially where quantitative thresholds guide stenting decisions. Although AS-OCT units are costlier than slit-lamp tests, targeted use can reduce repeated visits and unnecessary interventions, improving cost-effectiveness in resource-limited centers.
Our study also highlights the broader socioeconomic implications of punctal disease. Although not vision-threatening, chronic epiphora significantly impairs quality of life by interfering with reading, driving, and social interactions. The objective documentation of surgical success through OCT may reduce unnecessary follow-up visits, improve patient counseling, and optimize resource allocation in healthcare systems.
Limitations
The present study has certain limitations. It was conducted at a single center with a modest sample size, and surgical techniques were not randomized, introducing potential selection bias. Tear meniscus measurements, while standardized, may still be influenced by patient cooperation, blinking, or reflex tearing. Follow-up was limited to 6 months; longer-term data are required to evaluate recurrence and durability of outcomes. Despite these limitations, the high inter-observer reliability and consistency with external studies strengthen the robustness of our findings. Another limitation of this study lies in the economy and accessibility of AS-OCT. Although AS-OCT can provide important anatomical information, its equipment cost and limited availability may restrict its wide application in resource-scarce areas. The results of this study mainly reflect the application effect under the condition of AS-OCT, and its economic feasibility in low-resource environments still needs further research.
Future directions
Future research should aim to standardize AS-OCT imaging protocols, including scan location, lighting, and automated analysis software, to enhance reproducibility. Randomized trials comparing surgical techniques and adjunctive measures (e.g., stents, mitomycin-C) should use OCT-derived tear meniscus parameters as primary outcome measures [45–47]. Integration with complementary modalities such as ultrasound biomicroscopy and lacrimal endoscopy may provide a more comprehensive assessment of lacrimal outflow physiology. Longitudinal registries incorporating both imaging and patient-reported outcomes will be essential for establishing OCT as a gold standard in the evaluation of punctal surgery [48–50].
In summary, our study demonstrates that AS-OCT is a reliable, non-invasive, and objective tool for monitoring outcomes in lacrimal punctum obstruction surgery. Significant postoperative reductions in TMH, TMA, and TMV closely mirrored symptomatic and functional improvement, validating these parameters as biomarkers of success. Our findings align with international literature, underscoring the reproducibility of this approach. Incorporating AS-OCT into routine practice has the potential to standardize outcome assessment, guide surgical decision-making, and improve the quality of care for patients with punctal disease.
Conclusion
This study demonstrates that anterior segment optical coherence tomography (AS-OCT) is a valuable and objective tool for assessing outcomes in patients with lacrimal punctum obstructive disease. Postoperative reductions in tear meniscus parameters — with tear meniscus height decreasing from 0.45 mm to 0.30 mm and tear meniscus volume from 0.32 µL to 0.20 µL — closely mirrored improvements in symptoms and functional tear clearance. At six months, 82.7% of eyes achieved functional success and 88.5% achieved anatomical patency, confirming the effectiveness of punctal surgery across different techniques.
The strong correlation between reduction in tear meniscus volume and improvement in symptom scores highlights the physiological basis of surgical success and validates OCT-derived parameters as reliable biomarkers. Incorporating AS-OCT into clinical practice allows clinicians to document measurable changes, improve patient counseling, and standardize outcome reporting.
While our results are consistent with international literature, the study’s single-center design, modest sample size, and limited follow-up duration underscore the need for larger, multicenter trials with longer observation periods. Future research should focus on protocol standardization, automated imaging analysis, and integration with complementary modalities to enhance reproducibility and expand clinical utility.
In conclusion, AS-OCT offers a rapid, non-invasive, and reproducible method for quantifying tear dynamics and evaluating surgical success in punctal obstruction. Its integration into routine practice has the potential to transform outcome assessment in lacrimal surgery, bridging the gap between subjective symptom relief and objective physiological improvement.