Where will I end up? Relative location of sports medicine fellowship compared to residency among recent graduates
Jimmy Wen, David Park, Daniel Razick, Mouhamad Shehabat, Burhaan Syed, Muzammil Akhtar, Bhagvat Maheta, Caroline Goswami, Naomi Pai, Apple Zhu, Jose Luis Puglisi, Sarah Preiss-Farzanegan

TL;DR
This study examines where sports medicine fellows choose to train relative to their residency locations, finding that most stay in the same region.
Contribution
The paper provides new insights into geographic trends of sports medicine fellowship placements relative to residency training locations.
Findings
Family Medicine graduates are more likely to stay within 100 miles or the same state for their fellowship.
Emergency Medicine graduates are more likely to move farther from their residency location.
Most fellows train in the same region as their residency.
Abstract
Sports Medicine (SM) fellowships have garnered increased interest over the past several decades as greater emphasis has been placed on physical activity as a cornerstone of well-being. Fellows usually complete a residency in Family Medicine (FM), Physical Medicine & Rehabilitation (PM&R), Pediatrics, Emergency Medicine (EM), or Internal Medicine (IM). This study analyzes the recent geographic trends of SM fellows from 2019 to 2023. SM fellows who graduated between 2019 and 2023 were identified from publicly available data, and the distances between SM fellowship and residency were examined. These were categorized as within 100 miles, same state, same region, or different region. Odds ratios (OR) were calculated for the relative locations of a graduate’s primary specialty. A total of 852 fellows were included. A majority of fellows (64.4%) were from FM, 14.9% from PM&R, 7.1% from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
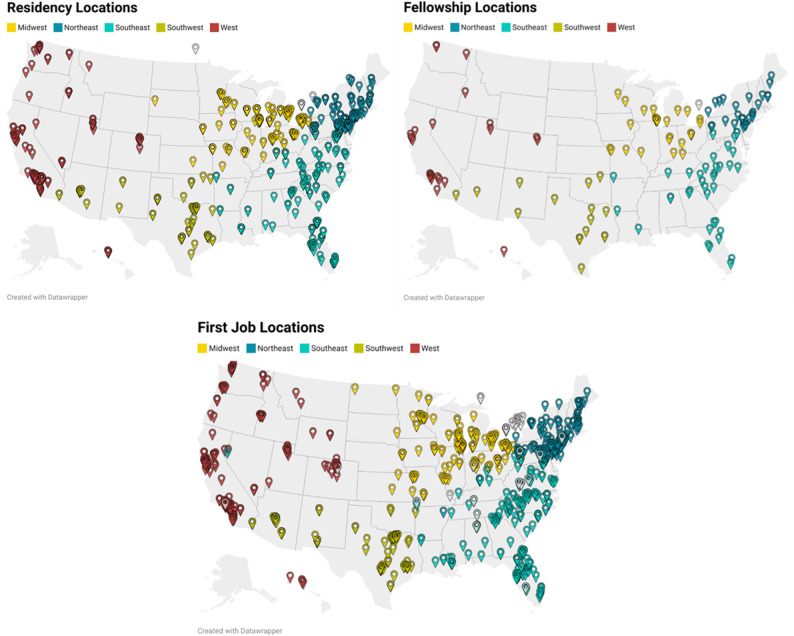 Figure 1
Figure 1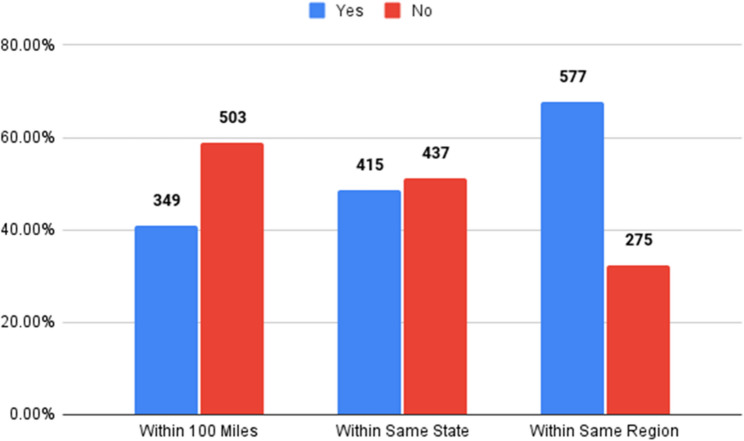 Figure 2
Figure 2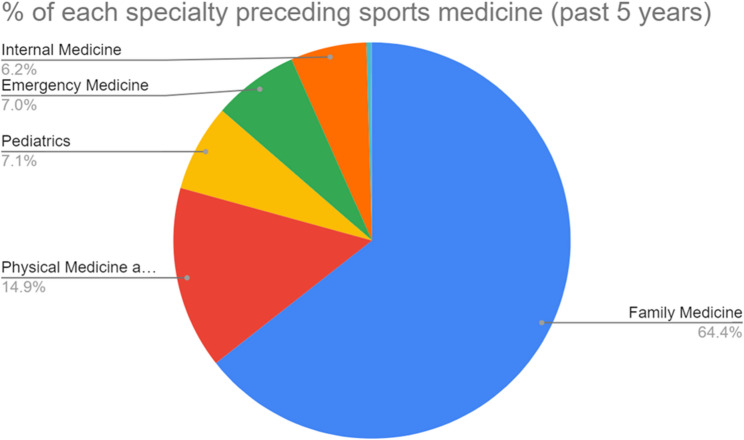 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal Disorders and Rehabilitation · Cardiovascular Effects of Exercise · Physical Activity and Health
Background
Sports medicine (SM) is a comprehensive field that extends beyond the confines of traditional medical practice, serving as the intersection between primary care, orthopedics, physiology, cardiology, nutrition, and rehabilitation. SM is a multidisciplinary field, and SM programs accept applicants from Physical Medicine & Rehabilitation (PM&R), Family Medicine (FM), Internal Medicine (IM), Pediatrics, and Emergency Medicine (EM) [1, 2]. SM fellowships are one year in duration and have become increasingly popular, as seen by the significant increase in match rate and doubling number of accredited programs and positions between 2010 and 2021 [2].
A notable paradigm shift has occurred in recent years within the field of SM due to the American College of Sports Medicine (ACSM) championing the concept of “exercise is medicine”. In 2018, the ACSM published its “Prescription for Health,” stating that 150 min of physical activity per week can prevent chronic diseases, including cardiovascular disease, diabetes mellitus type II, and various cancers [3, 4]. SM has continued to transcend its focus on elite athletes to embrace a wider demographic and promote active lifestyles to enhance general well-being, prevent chronic ailments, and improve quality of life.
As the field of SM continues to grow, its role in preventative care and enhancing athletic performance remains a crucial component of modern healthcare [2, 4]. Thus, the demand for SM physicians will continue to evolve across different settings, including academic centers, hospital systems, and community practices [2, 4]. Despite this growth, there is limited data on the geographical distribution from residency to fellowship and early career practice. Understanding these trends has important implications for SM fellowship program development, recruitment/hiring strategies, and workforce planning, especially as programs/hospitals may aim to find trainees who are more likely to stay within a certain region. In the present study, we seek to evaluate the relative distance of fellowships compared to residency for SM fellows between 2019 and 2023. By analyzing the geographical distribution of SM fellowships in the present study, this data will provide valuable information for medical students and residents to better anticipate possible relocation needs and plan out their future careers in SM.
Methods
Study design
This retrospective study, conducted in 2023, analyzed current and graduated fellows who completed an Accreditation Council for Graduate Medical Education (ACGME)-accredited SM Fellowship program in the United States between 2019 and 2023. This time period was chosen to reflect the most recent trends and data. The data was obtained from published information online by each fellowship program regarding residency specialty and location. For several programs, graduation information was not publicly available, and a standardized process was initiated to procure the requisite details. A maximum of three communication attempts via email were conducted, and if no response was received, graduate data from these programs were not included in this study. This study was determined to be exempt via the home Institutional Review Board (IRB).
Statistical analysis
The relative distance of graduate residency location to fellowship destination was categorized to be within a 100-mile radius, same state, same geographic region, and different geographic region. The 100-mile radius was chosen to signify individuals who remained close to their original training institutions, including hospitals within the city and nearby suburbs. If a fellow completed a fellowship and residency that was within 100 miles but crossed state or regional boundaries, they were categorized as within 100 miles. The closest applicable category was used when more than one category applied to a pairing. Thus, these distance categories were both hierarchical and cumulative. This method was chosen to evaluate geographic proximity rather than mutually exclusive classifications. Geographical regions (West, Midwest, Southwest, Southeast, Northeast) were determined by the National Geographic United States region classification [5].
Odds ratios (OR) were calculated to generate forest plots for each specialty. To determine the OR, the number of fellows specific to each category was calculated. Geographic proximity was determined hierarchically for OR calculations. For the OR analysis, each specialty was compared separately against all the other specialties combined. For example, for FM residency graduates, the exposure group consisted of FM residency graduates, while the reference groups consisted of residency graduates from all other specialties pooled together. Therefore, the OR evaluated the odds of staying within a certain geographical proximity for a given specialty relative to all other specialties. Fisher’s exact test was used to calculate a p-value of 0.05. Thus, p-values less than 0.05 were considered statistically significant. Confidence intervals were calculated via the Baptista-Pike method. Calculations were computed using the GraphPad software (Dotmatics, San Diego, CA).
Map rendering
Pinpoint location maps of the longitudinal coordinates for both residency and fellowship locations were generated via Datawrapper Maps Service (Datawrapper GmbH, Berlin, Germany). Each pinpoint location represents a resident’s location and was color-coded by geographical location, which mirrored the fellowship maps and displayed the origin of each individual.
Results
This study included data from 135 of 207 ACGME-accredited SM fellowships, accounting for 65.2% of all SM programs in the United States. The programs excluded from the study had either opted out of data collection or did not respond to communication attempts made to the institution. From the participating programs, 838 fellows from 2019 to 2023 were included, with first job data available for 792 fellows. Geographic distribution of the responding programs was broad and slightly more concentrated in the West and Southeast, with slightly less in the Southwest.
Program locations
The largest proportion of fellows (25.6%) completed a residency program in the Midwest. Other common locations for residency programs were the Southeast (24.2%), Northeast (22.1%), West (16.4%), and Southwest (10.0%) (Fig. 1).
Fig. 1. Residency, sports medicine fellowship, and first job pinpoint locations of included fellows
These trends are echoed in the fellowship and first job location maps and Table 1 as well. Similarly, these locations are illustrated using pinpoint maps, showing the locations where SM fellows completed their fellowship and their first job location after graduation (Fig. 1).
Table 1. Residency, Fellowship, and first job location regional distributionRegionResidency Location (%)Fellowship Location (%)First Job Location (%)Northeast22.119.420.3Southeast24.428.424.7Southwest10.011.910.1Midwest25.622.419.1West16.417.223.0Other1.50.72.8
Relative distances
A large proportion of the fellows (40.96%) completed an SM fellowship program within a 100-mile radius of their residency program, 48.71% in the same state, 67.72%within the same region (Fig. 2).
Fig. 2. Sports medicine fellowship location
Although the greatest proportion of fellows chose to complete their fellowship within the same region (67.7%) as their residency location, most fellows did not stay within the same state, nor did they complete their fellowship within 100 miles of their residency location. The distribution from residency to fellowship distances was right-skewed. The 10th percentile is 0 miles, the 25th percentile is 2 miles, the 50th percentile is 123 miles, the 75th percentile is 639.8 miles, and the 90th percentile is 1245.5 miles.
Following the SM fellowship, a large proportion of the graduates stayed within 100 miles (41.6%) for their first job, 51.3% stayed within the same state, and 69.9% stayed within the same region. Distribution for fellowship to first job distances was also right-skewed but broader. The 10th percentile was 3.1 miles, the 25th percentile was 19 miles, the 50th percentile was 183 miles, the 75th percentile was 781 miles, and the 90th percentile was 1472.4 miles. These percentiles are listed in Table 2.
Table 2. Distance percentiles traveled for fellowship and first jobPercentilesResidency to Fellowship (miles)Fellowship to First Job (miles)Minimum0010th03.125th21950th12318375th639.878190th1245.51472.4Maximum46936503.2
Specialties before SM
The vast majority of fellows (64.4%) specialized in FM, whereas other fellows had prior training in PM&R (14.9%), Pediatrics (7.1%), EM (7.0%), and IM (6.2%). Three fellows pursued a Neuromusculoskeletal specialty, and one fellow trained in Preventive Medicine. Fig. 3 illustrates the primary residencies that the SM fellows completed.
Fig. 3. Percentage of residency matching into fellowship
In all three categories, FM residency graduates were highly likely to stay within 100 miles (OR: 1.47, p = 0.009), same state (OR: 1.81, p < 0.0001), or same region (OR: 1.61, p = 0.002) for their SM fellowship. In contrast, EM residency graduates were more likely not to remain within 100 miles (OR: 0.47, p = 0.013) or in the same state (OR: 0.52, p = 0.0214). No other significant differences regarding the distance between fellowship and residency location were found among PM&R, Pediatrics, IM, and EM fellows. (Table 3).
Table 3. Percentage of PM&R, FM, IM, EM, and pediatrics relative locationResidencyLocation of Fellowship Relative to ResidencyPercentage Within Location (n)Percentage NOT Within Location (n)OR (95% CI)p-valuePhysical Medicine and RehabilitationWithin 100 Miles39.2% (49)60.8% (76)0.92 (0.62–1.35)0.695Within Same State41.6% (52)58.4% (73)0.71 (0.49–1.04)0.099Within Same Region64.8% (81)35.2% (44)0.86 (0.57–1.27)0.469Family MedicineWithin 100 Miles44.3% (240)55.7% (302)1.47 (1.10–1.95) 0.009 Within Same State54.1% (293)45.9% (249)1.81 (1.37–2.42) < 0.001 Within Same Region71.6% (388)28.4% (154)1.61 (1.20–2.16) 0.002 PediatricsWithin 100 Miles32.8% (20)67.2% (41)0.69 (0.40–1.20)0.224Within Same State37.7% (23)62.3% (38)0.61 (0.36–1.06)0.084Within Same Region59.0% (36)41.0% (25)0.67 (0.39–1.14)0.155Internal MedicineWithin 100 Miles36.2% (17)63.8% (30)0.81 (0.45–1.47)0.544Within Same State40.4% (19)59.6% (28)0.70 (0.38–1.27)0.294Within Same Region57.4% (27)42.6% (20)0.63 (0.35–1.14)0.148Emergency MedicineWithin 100 Miles25.4% (15)74.6% (44)0.47 (0.25–0.85) 0.013 Within Same State33.9% (20)66.1% (39)0.52 (0.30–0.91) 0.021 Within Same Region61.0% (36)39.0% (23)0.73 (0.43–1.25)0.252Bolded p-values are statistically significantOR (95% CI), Odds Ratio (95% Confidence Interval)
First job location
Following their SM fellowship, graduates from an FM background were more likely to stay within 100 miles (OR: 1.44, p = 0.016) and within the same state (OR: 1.63, p = 0.001). Contrastingly, graduates from a PM&R background were less likely to stay within 100 miles (OR: 0.50, p = 0.002) and the same state (OR: 0.48, p = 0.0006). No significant differences were found for the other specialties (Table 4).
Table 4. Percentage of fellows concerning specialty relative location to first jobResidencyLocation of Fellowship Relative to First JobPercentage Within Location (n)Percentage NOT Within Location (n)OR (95% CI)p-valuePhysical Medicine and RehabilitationWithin 100 Miles27.9% (31)72.1% (80)0.50 (0.32–0.77) 0.002 Within Same State36.0% (40)64.0% (71)0.48 (0.32–0.73) 0.0006 Within Same Region65.8% (73)34.2% (38)0.80 (0.52–1.22)0.302Family MedicineWithin 100 Miles44.7% (230)55.3% (284)1.44 (1.10–1.95) 0.016 Within Same State55.6% (286)44.4% (228)1.63 (1.22–2.19) 0.001 Within Same Region71.6% (368)28.4% (146)1.25 (0.91–1.71)0.168PediatricsWithin 100 Miles35.0% (21)65.0% (39)0.74 (0.43–1.28)0.280Within Same State43.3% (26)56.7% (34)0.71 (0.42–1.20)0.200Within Same Region63.3% (38)36.7% (22)0.72 (0.42–1.25)0.248Internal MedicineWithin 100 Miles37.8% (17)62.2% (28)0.84 (0.45–1.57)0.590Within Same State48.9% (22)51.1% (23)0.90 (0.49–1.65)0.737Within Same Region68.9% (31)31.1% (14)0.95 (0.50–1.82)0.875Emergency MedicineWithin 100 Miles51.7% (30)48.3% (28)1.55 (0.91–2.65)0.110Within Same State55.2% (32)44.8% (26)1.18 (0.69–2.02)0.543Within Same Region70.7% (41)29.3% (17)1.04 (0.58–1.87)0.897Bolded p-values are statistically significantOR (95% CI), Odds Ratio (95% Confidence Interval)
Discussion
This analysis of SM fellowship program locations compared to residency program locations provides insights into geographic trends notable for medical students, residents, advisors, and program directors. More than half of the fellows stayed within the same geographical region, which illustrates the possibility of a disproportionate spread of fellowships across the United States. Furthermore, this trend was observed with the first job placement after graduation. Most fellows appear to stay within their preferred regions; however, this highlights that regions without programs can remain underserved if trainees in these areas have fewer professional opportunities to stay close by. Geographic regions with more residency programs may have easier access to subsequent fellowships through networking and other opportunities. The Western and Southwestern regions had fewer residency and fellowship programs overall, highlighting the regional variations in training locations [6]. Programs may have incentives to retain fellowship graduates to practice in the same region as well, further contributing to a disproportionate spread of SM physicians. However, relocating to a different region can be attributed to personal factors such as the desire to return home, geographic preferences, limited personal or professional connections to the area, and quality of life considerations.
Personal and family considerations may sway a residency graduate’s preferences for fellowship location, but limited professional factors in certain regions or programs with a curriculum/resources that don’t match up with the residency graduates’ interests also play a significant role. Moving for residency and a subsequent fellowship can make settling down with a family, building community ties, and maintaining social and professional networks more difficult [7]. Recent studies have found that lifestyle factors such as family/vacation time, location, and scheduling become more important as individuals progress through their careers [8–10]. Several other recent studies evaluating factors towards the selection of primary care and surgical residencies likewise place a heavy emphasis on location, with a trend towards staying in the same region or the same institution [11–16]. The location of a residency can be an important predictor of future practice location, as mentioned by the Association of American Medical Colleges (AAMC) in reports available between 2012 and 2021, where more than half (55.2%) of the graduates were found to practice in the same state as their residency program [17]. Thus, this data further demonstrates the increased likelihood of fellows staying within their same geographic region and encourages the creation of more programs in areas that seek more SM physicians. However, it must be acknowledged that although applicants ultimately determine their rank list, the National Resident Matching Program (NRMP) match has an applicant-favored algorithm that assigns positions based on these preferences.
The primary specialty training that SM fellows completed before fellowship was: FM (64.4%), PM&R (14.9%), Pediatrics (7.1%), EM (7%), IM (6.2%), Neuromusculoskeletal medicine (0.3%), and Preventive medicine (0.1%). FM residents may have an advantage when applying for SM fellowships, given their high predominance amongst SM fellows. However, this may be attributed to some SM programs only being available to FM residency graduates [18]. This trend has evolved over the years, with fellowship programs increasing acceptance and consideration for more specialties. Due to the multidisciplinary aspects of SM, fellowship programs will ideally continue to accept and promote applicants with residency training in various disciplines [1].
As this study has found, there is a trend for fellows to remain within the same geographical region as their residency. Although our study did not directly evaluate healthcare disparities, previous literature has shown that rural areas do not have the same level of access to healthcare services and specialists compared to urban areas [12]. One factor that can affect geographical inequity is student background, as students from rural backgrounds or who have experience in a rural community have a higher likelihood of practicing in a rural community [12]. A similar trend is observed for students from an urban background who are more likely to remain in urban areas. A majority of SM fellowships are concentrated in large cities [6]. Thus, health equity is an issue due to the unequal distribution of providers. This encourages programs to recruit qualified individuals from rural backgrounds and promote more exposure for students in different environments [19]. Fellows from rural backgrounds can be a proposed strategy, as these individuals may be more likely to return to and practice in rural areas. Specialty choices ultimately have profound effects on healthcare delivery, as seen through the imbalance between the supply of physicians in particular specialties and demand in patient care, especially in rural areas. Geographical inequality can lead to reduced access to physicians, resulting in a ripple effect towards unsatisfactory patient outcomes and reduced health equity. SM has evolved from centering around athletes to encompassing the general population. As a result, the patient population in need of SM is everywhere. As advocacy of physical activity has increased over the years to combat risk for chronic diseases, the demand for SM physicians will also continue to increase, necessitating the need for equal distribution of physicians [20].
Implications
Understanding these geographic trends has implications for both applicants and programs. This is especially pertinent information as most primary care SM websites do not provide comprehensive program information [21]. Location is a major consideration during the application process for both medical students and residents, especially if they have certain long-term goals in mind. Applicants can place more emphasis on particular residency programs if they have a specific fellowship program in mind. The proximity of fellowship programs can be a deciding factor for students when choosing a specific residency and acts as a guide for future medical students and residents when considering program selections. Fellowship training can require a fairly quick relocation, and understanding the national trends can help applicants plan out personal, financial, and logistical factors. For fellowship programs, geographic proximity patterns provide insight into where the applicant pool tends to originate from, which can support targeted recruitment strategies. On a broader scale, analyzing how physicians relocate throughout different stages of training can help provide context for workforce distribution trends and identify areas that can benefit from targeted training expansion. Although these regional variations are notable, we did not have data on population size, actual SM physician distribution, or regional SM needs. Thus, our analysis is strictly limited to describing the geographic patterns.
Limitations
Our study provides a general understanding of the locations that residents matched into for SM fellowships over the past five years, but it must be considered within the context of its limitations. First, we selected this time range for data collection as it provides the most recent trends and data, but is limited by the range of the total available data. This also limits the generalizability as it includes both pre- and post-pandemic data. Future studies would be needed to validate whether these trends persist post-pandemic. Second, we were unable to obtain data from all programs listed in the American Medical Society for Sports Medicine (AMSSM) directory, with programs either not responding or declining to participate, thus rendering our results susceptible to non-responder bias. Although the programs included were generally evenly spread, there was a regional variation, with more responses from programs in the West and Southeast, and fewer from the Southwest. This can limit the generalizability of our region-specific trends.
Additionally, applicant-level geographic data was not available, which prevents comparison of the geographical diversity of applicants with that of the matched fellows. Thus, the determination of the cause of the observed regional retention could not be ascertained due to program selection or applicant preferences. Third, we did not analyze the number of fellowships that only accepted graduates from specific primary residencies. Therefore, the predominance of FM residency graduates in our study may be due to fewer programs admitting graduates from other specialties, but also mirrors national patterns in which SM fellowship positions are mainly filled by FM applicants. Furthermore, residency programs are not evenly distributed across the primary residencies evaluated here. For example. FM has substantially more programs nationwide compared to EM and PM&R. The greater program density can increase geographic proximity between fellowships and subsequent first job opportunities. This can also influence the geographic trends, as FM applicants may have more flexibility to apply regionally compared to other specialties. Thus, the geographic clustering found in this study can reflect fellowship selection trends, the underlying baseline characteristics of the applicant pool, and the training infrastructure rather than causal specialty effects. Finally, our data collection focused primarily on objective data on the relative location between residency and SM fellowship. The factors and motives associated with the fellows’ choices were not collected. SM workforce density, regional SM healthcare needs, and population size were not assessed as well, which prevents the determination of whether these geographic patterns are leading to geographical inequity. Future studies in this field can be conducted by analyzing the specific factors, motives, and rationale that influence residency graduates’ choice of a particular fellowship. This qualitative information can be elicited through surveys or personal interviews, but will be insightful in understanding the different factors that influence a residency graduate’s choice of fellowship, not only in SM but also compared to other specialties.
Conclusion
Our study concludes that residency graduates are more likely to remain in the same geographic region for their SM fellowship. FM had the highest continuity close to their training location as well as their first job, while EM had the lowest likelihood of staying close by. Interestingly, for PM&R, these graduates had a low probability of staying in the area for their first job. This data provides insights into the geographic mobility of recent SM fellows for interested applicants. Understanding these trends allows applicants to set expectations, anticipate relocation, and make informed choices when planning their potential training pathways.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Exercise is Medicine. ACSM_CMS. https://www.acsm.org/news-detail/2018/05/02/exercise-is-medicine. Accessed November 3. 2023.
- 2United States regions. Nationalgeographic.org. https://education.nationalgeographic.org/resource/united-states-regions/. Accessed November 3. 2023.
- 3The job market for sports medicine physicians in the United States. Careerexplorer.com. Published April 11, 2017. https://www.careerexplorer.com/careers/sports-medicine-physician/job-market/. Accessed November 4. 2023.
- 4Ladha FA, Pettinato AM, Perrin AE. Medical student residency preferences and motivational factors: a longitudinal, single-institution perspective. BMC Med Educ. 2022;22(1). 10.1186/s 12909-022-03244-7.10.1186/s 12909-022-03244-7PMC 892926535300656 · doi ↗ · pubmed ↗
- 5Report on residents. AAMC. https://www.aamc.org/data-reports/students-residents/data/report-residents/2022/executive-summary. Accessed November 4. 2023.
- 6Sports Medicine Fellowships in the USA and Canada. Amssm.org. https://www.amssm.org/Fellowships Positions.html. Accessed November 4. 2023.
- 7Jaret P. Attracting the next generation of physicians to rural medicine. AAMC. Published February 3, 2020. https://www.aamc.org/news/attracting-next-generation-physicians-rural-medicine. Accessed November 4, 2023.