Detecting racial and ethnic disparities in study exclusion: screening outcomes from a RCT for pregnant women with insomnia
Carolyn Ponting, Candance Sorensen, Bernadette McClelland, Richelle Mah, John Neuhaus, Rachel Manber, Andrew D. Krystal, Patricia Moran, Jennifer N. Felder

TL;DR
This study found that racial and ethnic disparities exist in the exclusion of pregnant women with insomnia from a clinical trial, potentially limiting diversity in research.
Contribution
The study quantifies racial/ethnic disparities in trial exclusion rates and highlights their impact on diversity in behavioral health research.
Findings
Black participants were more likely to be excluded due to comorbid conditions like sleep apnea.
Asian participants were more likely to be excluded for subclinical insomnia symptoms.
Black participants had significantly higher odds of exclusion compared to White participants for three eligibility criteria.
Abstract
Eligibility criteria are a critical component of a well-designed clinical trial, enhancing trial safety and internal validity. Yet, data suggest that exclusion rates based on these criteria often vary by participant race/ethnicity. This study compared the proportion of participants (n = 4235) from seven racial/ethnic groups, who were included versus excluded from participation in a randomized controlled trial (RCT) testing two digital sleep interventions for the prevention of perinatal depression. Eight 2 × 7 chi-squared tests were conducted to compare the proportion of each racial/ethnic group excluded due to each eligibility criterion. Logistic regressions were fitted to estimate the magnitude of the relationship between racial/ethnic group and exclusion based on each eligibility criterion. The proportion of excluded participants differed by race/ethnicity across all eight…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
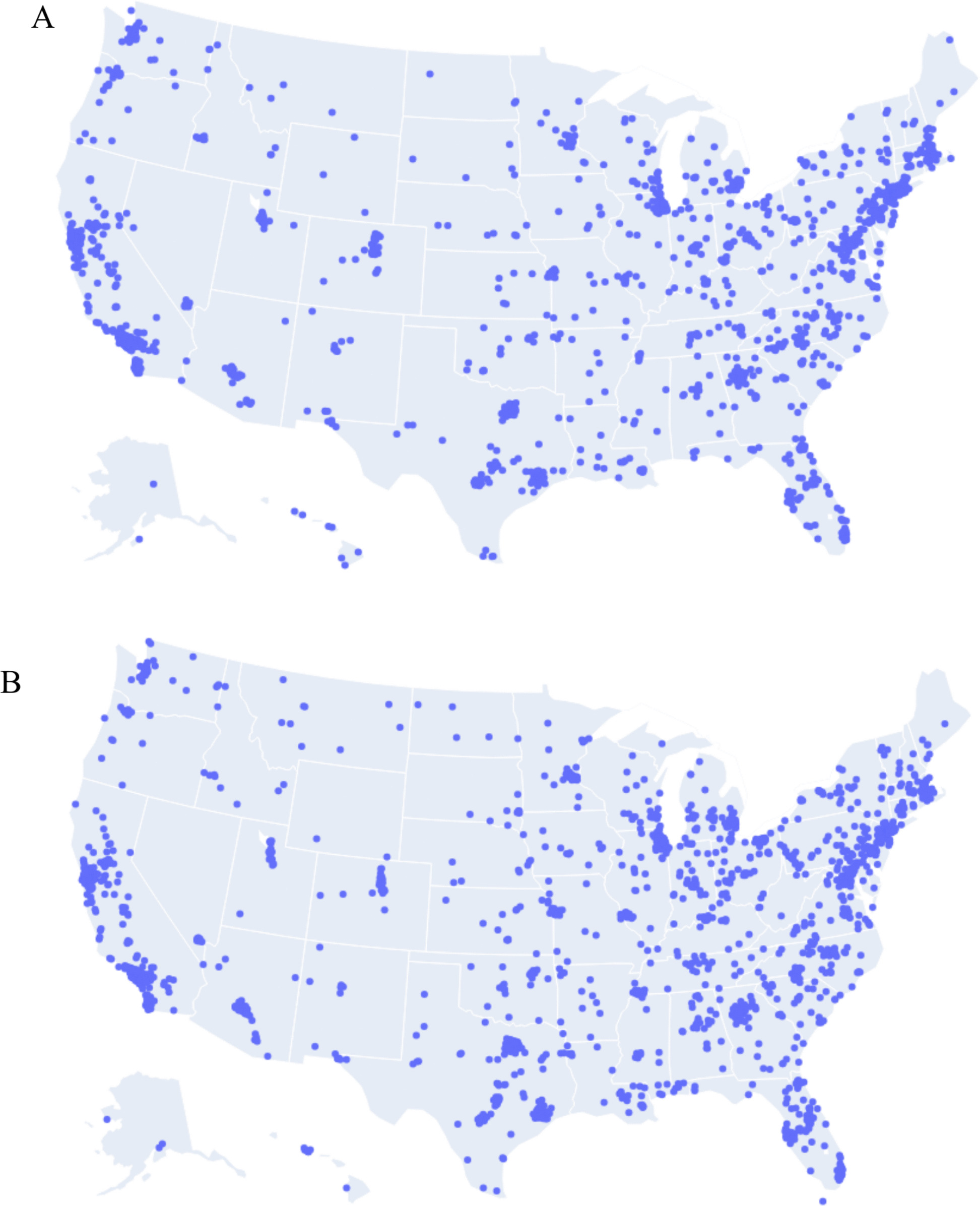 Figure 1
Figure 1- —http://dx.doi.org/10.13039/100000025National Institute of Mental Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · Maternal Mental Health During Pregnancy and Postpartum · Neonatal and fetal brain pathology
Racial and ethnic differences in study exclusion from a CBT-I trial to prevent perinatal depression
Background
Randomized controlled trials (RCTs) are undertaken to establish a causal link between an intervention and clinical outcome (i.e., intervention efficacy). While RCTs are considered the gold standard for evaluating the effects of an intervention, they have long been criticized for failing to adequately enroll diverse samples, including racial and ethnic minorities [1–4]. These critiques are of continued relevance. A review of US-based clinical trials registered in ClinicalTrials.gov from 2000 to 2020, consisting of 20,692 studies, showed that only 43% of trials reported the racial or ethnic makeup of their participant samples [5]. Of the trials that did report race and ethnicity, 80% of participants identified as non-Latinx white [5]. In addition to intervention samples being disproportionately non-Latinx white [6–8], they are also more likely to be of middle to high socioeconomic status [9, 10], and less likely to present with medical or mental health comorbidities [11, 12]. Data from these relatively homogenous participant pools make up the majority of our intervention evidence base, but do not reflect the broader population and thus, clinical guidelines and areas of clinical innovation may lack generalizability for minoritized groups [5, 13].
There are several contributors that lead to relatively homogenous participant pools in RCTs for behavioral health interventions [2]. Notably, recruitment challenges are commonplace. Many researchers rely on convenience samples or are met with limited buy-in from clinics and community partners, who are rarely compensated for their recruitment efforts and are juggling competing demands [14, 15]. Participants from minoritized backgrounds may also feel warranted skepticism about participating in intervention research given historical abuses by researchers, or may face logistical challenges to participation due to language barriers or time constraints associated with disproportionate caregiving burdens and access to reliable transportation [16, 17]. Less studied, however, are trial design characteristics—like inclusion and exclusion criteria—that can inadvertently keep minoritized people from participating at disproportionate rates [1].
Inclusion and exclusion criteria aim to enhance trial safety and internal validity. Criteria are selected to ensure that participants receiving an intervention have the clinical presentation and severity most likely to benefit from treatment and that additional health conditions or medications do not blunt treatment effects [18]. However, disproportionate exposure to adverse social determinants of health like poverty, racism, access to health care, and safe housing means that ethnic/racial minorities and low-income groups are more likely to have health conditions and life circumstances that commonly exclude them from trial participation [19, 20].
For example, in a smoking cessation study that used purposeful sampling and stratified their randomization so that an equal number of Black, Latina, and non-Latina White participants would be assigned to each treatment arm—study exclusion criteria disproportionately impacted Black and Latina participants [21]. Webb Hooper and colleagues [21] reported that while non-Latina White participants were ineligible at a rate of 24%, Latina participants were ineligible at a rate of 37%, and Black participants at a rate of 42%—differences that were driven by higher rates of exclusionary mental health comorbidities. Aligned with these findings, other smoking-cessation and cancer trials have found that Black prospective participants were disproportionately excluded from trial participation due to residential instability (i.e., not having a home address at intake) [22], or medical comorbidities [23]. Taken together, available data suggest that exclusion criteria do not have equal impacts on prospective participants.
While eligibility criteria may be modified to enhance trial diversity, certain exclusion criteria are well justified and necessary even when they impact groups at different rates. Thus, examining whether racially or ethnically minoritized groups or low-income groups are disproportionately impacted by exclusion criteria can identify demographic groups that ought to be screened at greater numbers to enhance the likelihood of obtaining a representative sample. The present study examined whether the rates of exclusion in an RCT evaluating two digital sleep interventions for the prevention of perinatal depression were different across several distinct criteria, dependent on prospective participants’ race or ethnicity. Findings provide insight into the design characteristics that can contribute to homogenous samples in randomized trials and unintentionally perpetuate a clinical evidence base that lacks generalizability.
Methods
Participants
Participants in this study were pregnant people (n = 4235) who took an online screening survey to determine their potential eligibility for a randomized controlled trial testing the efficacy of two sleep interventions—digital cognitive behavioral therapy for insomnia (CBT-I) and Sleep Hygiene Education (SHE)—for the prevention of perinatal depression. The clinical trial is registered at Clinicaltrial.gov (Protocol: NCT05596318, uploaded 10/24/2022). Participants were recruited nationwide through advertisements on Meta (i.e., Facebook, Instagram) and two popular pregnancy planning apps, BabyCenter and What to Expect. Over half of prospective participants (n = 2340; 55.3%) were excluded based on the results of this initial screener. The present study reports on differences in study exclusion among participants who took the online screening between November 2022 and August 2024.
Design
Prospective participants who clicked on the online study advertisements were directed to a study landing page that provided a brief summary of the study goals and procedures, and a detailed screening consent form. Prospective participants who signed the screening consent form were directed to complete the screening survey. All screening procedures were approved by the Institutional Review Board at the University of California, San Francisco, IRB # 21–35440. The first screening questions asked participants whether they were currently pregnant and, if so, asked for their gestational age and due date. Participants between 14 and 25 weeks pregnant were invited to continue with the screening survey. See Table 1 for eligibility questions, response options, and rationale for each screening criterion. In addition to responding to eligibility questions, prospective participants were also asked to provide basic demographic data. This included their age, household income, number of people supported by their household income, educational attainment, zip code of residence, and race/ethnicity. The present study used U.S. Census Bureau definitions of race and ethnicity. Race was defined as a person’s self-identification with one or more social groups based on physical characteristics, ancestry, or shared history; these categories are understood to represent social constructions as opposed to biological or genetic classifications. Ethnicity was defined as an individual’s self-identification of the origin of their nationality, culture, or language, and is distinct from race. Participants indicated their racial identity by responding to the question: “Which of the following categories best describes your race? (Select all that apply) (i.e., American Indian or Alaskan Native, Asian, White, Black or African American, Native Hawaiian or Other Pacific Islander, A race not described here).” Participants indicated their ethnicity by responding to the question: “Are you of Hispanic, Latino/a/x or Spanish origin? (i.e., yes, no).” Table 1. Eligibility survey items administered to prospective participants and their rationaleQuestionResponse optionsEligible responseExclusion rationaleAre you currently on bed rest?A. YesB. NoNoParticipants placed on bedrest would not be able to engage in the time in bed restriction component of CBT-IWhat is your age (in years)?Open text ≥ 18Adolescents have unique sleep needsDo you have daily access to a computer, phone, or tablet that is connected to the internet?A. YesB. NoYesInterventions are delivered digitallyAre you able to read and speak English?A. YesB. NoYesThe digital CBT-I app is currently available in English onlyHas a healthcare provider every diagnosed you with bipolar disorder, or told you that you were manic or hypomanic?A. YesB. NoNoThe time in bed restriction component of CBT-I could precipitate or exacerbate symptoms of maniaHave you ever experienced psychosis (hallucinations or delusions) or been diagnosed with a psychotic disorder, like schizophrenia?A. YesB. NoNoSymptoms of psychosis could be exacerbated by the time in bed restriction component of CBTHas a healthcare professional ever diagnosed you with any of the following sleep disorders? Check all that applyA. Insomnia disorderB. Sleep apneaC. NarcolepsyD. ParasomniaE. Circadian rhythm disorderF. Restless leg syndromeG. None of the aboveInsomnia disorderORNone of the aboveExclusionary sleep disorders are unlikely to benefit from digital CBT-IDo you work the night shift?A. YesB. NoNoCBT-I would likely be ineffective or the effect would be difficult to interpretAre you currently taking an antidepressant? (e.g., SSRI, SNRI, TCA, MAOI)A. YesB. NoC. Not sureNoORNot sureAntidepressant medication use would make the effect of CBT-I on preventing depression difficult to interpretAre you planning to begin taking an antidepressant before you are 12 months postpartum?A. YesB. NoC. Not sureNoORNot sureAntidepressant medication use would make the effect of CBT-I on preventing depression difficult to interpret
Data analysis
The objective of the statistical analysis was to compare the proportion of each racial/ethnic group excluded due to each eligibility criterion. For the purposes of these analyses, seven ethnic and racial categories were compared: (a) Black, (b) American Indian/Alaska Native/Native Hawaiian or Other Pacific Islander (AI/AN/NHPI), (c) Asian, (d) White, (e) Multiracial (i.e., individuals who selected more than one race), (f) Latina (i.e., inclusive of individuals who indicated their race was White or “other” as well as Latino/a/x ethnicity), and (g) Latina Black (i.e., individuals who reported Black race and Latino/a/x ethnicity). A 2 × 7 chi-squared test was conducted to compare the proportion of each racial/ethnic group excluded due to each of the eight eligibility criteria. All eight exclusion criteria were coded dichotomously (i.e., yes, no); the criteria assessed were:
- Being on bedrest,
- A self-reported history of mania or bipolar disorder,
- A self-reported history of sleep apnea,
- A self-reported history of restless leg syndrome,
- Current night shift work,
- Current antidepressant medication use,
- Planned antidepressant use prior to the first year postpartum, and
- Subclinical insomnia severity scores (i.e., score < 11 on the Insomnia Severity Index [24]).
While each exclusion criterion was examined independently, participants excluded at the screening stage may have been disqualified from participating for multiple reasons. An additional 2 × 7 chi-squared test was conducted to assess whether there were differences in the proportion of each racial or ethnic group who were excluded for multiple reasons compared to those who were not.
To assess the magnitude of the independent associations between each racial/ethnic group and the likelihood of being excluded by each eligibility criterion, we fitted eight binary logistic regression models. The same racial/ethnic groups tested in the chi-squared analyses were dummy coded and entered as independent variables, with White participants serving as the reference group. The dependent variable was study exclusion, where study inclusion served as the reference group. About 2% of participants (n = 84) did not report race or ethnicity data and was not included in chi-squared or logistic regression analyses, leaving a sample of 4151.
We did not adjust models for income or education because the goal of the study was to document and quantify the extent to which trial eligibility criteria differentially impact racial/ethnic groups. Socioeconomic variables are themselves shaped by structural racism and systemic inequities; therefore, accounting for them in regression models has the potential to underestimate the effect of racial/ethnic structural disadvantage [25]. Moreover, from a practical standpoint, unadjusted models may offer greater utility for clinical trialists who are unlikely to have access to recruitment pools in which socioeconomic status is evenly distributed across racial/ethnic groups. Systemic inequities in the USA have shaped the economic and educational attainment of racially/ethnically minoritized populations, contributing to persistent disparities across these domains [26, 27]. Data were analyzed using IBM SPSS (version 29) software.
Results
For detailed demographic characteristics of included and excluded participants, see Table 2 and Fig. 1. Overall, the proportion of participants excluded from the study at screening differed depending on race and ethnicity X^2^ (df = 6, N = 4151) = 17.23, p = 0.008. Latina participants were least likely to be excluded (48.0%), while Multiracial participants were most likely to be excluded (60.4%). The proportion of participants who were excluded due to multiple reasons differed by racial or ethnic group X^2^ (6, N = 4151) = 28.146, p < 0.001. Multiracial (21.7%) and Black participants (21.4%) were most likely to be excluded for multiple reasons, while American Indian/Alaska Native/Native Hawaiian and Pacific Islander (11.5%) and Asian participants (12.1%) were least likely to be excluded for multiple reasons. Table 3 compares the proportion of participants from each racial/ethnic group who were eligible or ineligible across each criterion. Table 2. Sample Characteristics of prospective participants who were included versus excluded following initial screening surveyIncluded (n, %)Excluded (n, %)Chi-squaredRace/ethnicityX^2=^17.23, p =.008 Asian (n = 338)153 (45.3%)185 (54.7%) American Indian, Alaska Native, Native Hawaiian or Other Pacific Islander (n = 78)38 (48.7%)40 (51.3%) Black (n = 739)327 (44.2%)412 (55.8%) Latina Black (n = 71)36 (50.7%)35 (49.3%) Latina (n = 667)347 (52.0%)320 (48.0%) Multiracial* (n = 217)86 (39.6%)131(60.4%) White (n = 2041)904 (44.3%)1,137 (55.7%)Total family income before taxesX^2=^22.16, p <.001 Less than 25,000–50,000–100,000–200,000 or more (n = 674)315 (46.7%)359 (53.3%) Don’t know/prefer not to say (n = 266)86 (32.3%)180 (67.6%)EducationX^2=^32.10, p <.001 Less than a high school degree (n = 81)20 (24.7%)61 (75.3%) High school graduate/GED (n = 451)451 (39.5%)273 (60.5%) Some college (n = 904)423 (46.8%)481 (53.2%) Bachelor’s degree (n = 1,316)665 (49.8%)661 (50.2%) Professional/graduate degree (n = 1403)619 (44.1%)784 (55.9%)Relationship statusX^2^ = 3.18, p =.20 Married/living with partner (n = 3669)1649 (44.9%)2020 (55.1%) Partnered, living separately (n = 295)138 (46.8%)157 (53.2%) Single, not involved with partner (*n *= 271)108 (39.9%)163 (60.1%)*Multiracial participants included 59.4% of participants who identified as Black and another race and 37.8% that identified as American Indian/Alaska Native and another raceFig. 1Location of included (top; panel A) and excluded (bottom; panel B) participants plotted by zip codeTable 3Frequencies and percentages of participants (n = 4145) from each racial/ethnic group excluded from study participation based on each eligibility criterionBlackAI/AN/NHPIAsianWhiteMulti-racialLatinaLatina BlackBed rest Yes82 (11.1%)1 (1.3%)16 (4.7%)28 (1.4%)9 (4.1%)27 (4.0%)3 (4.2%)Lifetime history of bipolar disorder or mania Yes53 (7.2%)7 (9.0%)4 (1.2%)113 (5.5%)21 (9.7%)28 (4.2%)9 (12.7%)Lifetime history of sleep apnea Yes45 (6.1%)1 (1.3%)10 (3.0%)70 (3.4%)14 (6.5%)18 (2.7%)5 (7.0%)Lifetime history of restless leg syndrome Yes18 (2.4%)2 (2.6%)2 (0.6%)98 (4.8%)7 (3.2%)15 (2.2%)1 (1.4%)Current night shift work Yes58 (7.8%)3 (3.8%)10 (3.0%)58 (2.8%)15 (6.9%)29 (4.3%)4 (5.6%)Current antidepressant medication use Yes55 (7.4%)8 (10.3%)27 (8.0%)390 (19.1%)24 (11.1%)65 (9.7%)3 (4.2%)Planned antidepressant medication use Yes66 (8.9%)7 (9.0%)18 (5.3%)265 (13.0%)21 (9.7%)47 (7.0%)4 (5.6%)Subclinical insomnia severity score Yes95 (12.9%)8 (10.3%)117 (34.6%)437 (21.4%)46 (21.1%)124 (18.6%)4 (5.6%)Total739 (100%)78 (100%)338 (100%)2041 (100%)217 (100%)667 (100%)71 (100%)AI/AN/NHPI American Indian, Alaska Native, Native Hawaiian or Other Pacific Islander
Table 4 presents results from eight logistic regressions, showing odds ratios, and 95% confidence intervals, for exclusion likelihood by eligibility criterion across racial and ethnic groups. Regarding eligibility criteria that assessed for health concerns and comorbidities that may have impacted the cost-benefit analysis of the sleep programs, exclusion differed by race and ethnicity. For example, the proportion of participants excluded due to bedrest differed by race or ethnicity X^2^ (6, N = 4,151) = 135.65, p < 0.001. Logistic regressions demonstrated that compared to their White counterparts**,** Black participants had over six times the odds of being excluded due to current bedrest (OR = 6.86), while Asian (OR = 2.73), Multiracial (OR = 2.37), and Latina (OR = 2.32) women had more than twice the odds of exclusion for the same reason. The proportion of participants excluded due to self-reported history of mania or bipolar disorder X^2^ (6, N = 4151) = 33.28, p < 0.001, and self-reported history of sleep apnea* X*^2^ (6, N = 4151) = 20.94, p = 0.002 also differed by participant race or ethnicity. Logistic regressions demonstrated that compared to their White counterparts, Latina Black participants had 2.42 times the odds and Multiracial participants had 1.74 times the odds of being excluded due to self-reporting a history of mania or bipolar disorder, while Asian participants had one fifth the odds (OR = 0.20) of being excluded for the same reason. Multiracial participants had 1.81 times the odds and Black participants 1.70 times the odds of being excluded due to self-reporting a history of sleep apnea compared to their White counterparts. Table 4. Odds ratios and 95% confidence intervals assessing the magnitudes of association of participant race/ethnicity with study exclusion for each eligibility criterionOdds Ratio95% CILLULBed rest Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi^2$$\end{document} [6,4235] = 102.55, p <.001 White1.00 AI/AN/NHPI.71.105.26 Asian2.731.50****4.95 Black6.864.62****10.17 Multiracial2.371.13****4.98 Latina2.321.40****3.83 Latina Black2.42.738.04Lifetime history of bipolar disorder or mania Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 36.01, p <.001 White1.00 AI/AN/NHPI1.61.723.56 Asian**.20****.07****.53** Black1.26.901.76 Multiracial1.741.07****2.83 Latina.71.471.09 Latina Black2.361.154.87Lifetime history of sleep apnea Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 18.55, p <.005 White1.00 AI/AN/NHPI.34.052.48 Asian.80.411.56 Black1.701.17****2.48 Multiracial1.811.01****3.26 Latina.73.431.22 Latina Black1.99.785.07Lifetime history of restless leg syndrome Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 34.31, p <.001 White1.00 AI/AN/NHPI.49.122.03 Asian**.11****.03****.45** Black**.47****.28****.77** Multiracial.62.291.36 Latina**.43****.25****.74** Latina Black.27.041.94Current night shift work Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 27.54, p <.001 White1.00 AI/AN/NHPI1.14.353.70 Asian.87.441.70 Black2.431.70****3.47 Multiracial2.121.19****3.76 Latina1.30.842.01 Latina Black1.70.604.80Current antidepressant medication use Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 105.90, p <.001 White1.00 AI/AN/NHPI.48.231.01 Asian**.37****.24****.55** Black**.34****.25****.46** Multiracial**.53****.34****.82** Latina**.46****.35****.60** Latina Black**.19****.06****.60Planned antidepressant medication use** Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 39.05, p <.001 White1.00 AI/AN/NHPI.66.301.44 Asian**.38.23****.61** Black**.65****. 49****.87** Multiracial.72.451.14 Latina**.51****.37****.70** Latina Black.40.141.10Subclinical Insomnia Severity Score Omnibus test \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\chi$$\end{document} ^2^(6, 4235) = 84.90, p <.001 White1.00 AI/AN/NHPI**.43****.21****.90** Asian2.001.56****2.56 Black**.56****.44****.71** Multiracial1.02.721.43 Latina.86.691.08 Latina Black**.23****.08****.62**AI/AN/NHPI American Indian, Alaska Native, Native Hawaiian or Other Pacific IslanderBolded effects are significant at a threshold of p <.05. The reference group is White
Some participants were excluded due to working conditions that would have required specific adaptations to the sleep intervention. The proportion of participants excluded due to current night shift work X^2^ (6, N = 4151) = 38.88, p < 0.001 differed among racial or ethnic groups. A logistic regression demonstrated that compared to White participants, Black participants had 2.43 times the odds of exclusion due to night shift work, while Multiracial participants had 2.12 times the odds of being excluded for the same reason.
Participants were also excluded for antidepressant medication use, which would have obscured preventive effects of the interventions on depression. The proportion of participants excluded due to current antidepressant medication use X^2^ (6, N = 4151) = 100.06, p < 0.001, and planned antidepressant use prior to the first year postpartum* X*^2^ (6, N = 4151) = 35.99, p < 0.001, differed based on participant race or ethnicity. Logistic regressions demonstrated that Latina Black (OR = 0.19), Black (OR = 0.34), Asian (OR = 0.37), Latina (OR = 0.46), and Multiracial (OR = 0.53) participants all had reduced odds of exclusion due to current antidepressant medication use compared to their White counterparts. Asian (OR = 0.38), Latina (OR = 0.51), and Black (OR = 0.65) participants also had reduced odds of exclusion due to reported plans to begin antidepressant medication prior to the first year postpartum compared to their White counterparts.
Finally, many participants were excluded because their insomnia symptoms were subclinical, which would have limited the detection of symptom improvement. The proportion of participants excluded due to subclinical severity scores differed by race and ethnicity X^2^ (6, N = 4151) = 85.99, p < 0.001. A logistic regression demonstrated that compared to their White counterparts, Asian women had 2.00 times the odds of exclusion due to subclinical severity scores on a validated insomnia screening measure, while Black (OR = 0.56), Latina Black (OR = 0.23), and AI/AN/NHPI (OR = 0.43) participants had reduced odds of exclusion for the same reason.
Discussion
The present study examined racial/ethnic differences in eligibility for a randomized trial testing two digital sleep interventions for the prevention of perinatal depression. Overall, Multiracial participants (a majority of whom identified as Black and another race) were excluded at the highest rates following initial screening, while Latina participants were excluded at the lowest rates. Further, across all eight eligibility criteria assessed, participants were excluded at different rates based on their race or ethnicity, and Multiracial and Black participants were most likely to be excluded for multiple reasons. Multiracial and Black participants had significantly higher odds (odds ratios ranging from 1.70 to 6.86) of study exclusion across three of the eight eligibility criteria (i.e., bed rest, night-shift work, and lifetime sleep apnea). These data suggest that even among individuals demonstrating interest in participating in a clinical trial for prenatal insomnia, eligibility criteria can exclude participants of particular racial/ethnic identities at different rates.
Compared to other racial and ethnic groups, Black and Multiracial participants—most of whom identified as Black—had increased odds of being excluded due to comorbid conditions such as sleep apnea or prescribed bed rest. A wide range of clinical trials, including those that test non-surgical treatments for cancer [28], rheumatoid arthritis [29], and cardiovascular disease [30], also report high rates of exclusion of Black participants due in part to comorbid health conditions. Inequities, including systemic racism, socioeconomic disparities, and poorer quality health care [31, 32], contribute to the high rates of mental and physical comorbidities experienced by Black communities in the USA [31, 33]. These findings highlight trial design features that may unintentionally exclude Black participants. Specifically, the greater the number of exclusionary criteria based on co-morbid mental and physical health conditions, the higher the likelihood that Black participants will be excluded.
This study showed that a larger proportion of Latina Black participants reported a history of bipolar disorder or sleep apnea than any other racial or ethnic group. Further, logistic regressions revealed that Latina Black participants had significantly greater odds of exclusion due to a history of bipolar disorder compared to White participants. While Latina ethnicity is often examined without attention to race, preliminary evidence suggests that Latina Black (also referred to as Afro-Latina) women have worse maternal health and birth outcomes than their White or Latina counterparts [34]. Disparities in health outcomes are partly driven by the compounded social stressors such as discrimination associated with holding multiple minority identities [35, 36] and less access to healthcare. Increasingly, scholars in maternal mental health equity have encouraged race data be disaggregated from Latina ethnicity [37] to more accurately characterize the heterogeneity in Latinx communities and better understand the health needs of each subpopulation. Present findings showed differential exclusion rates between Latina and Latina-Black participants dependent on eligibility criteria. Criteria that disproportionately exclude Black women, including those of Latinx ethnicity, from perinatal intervention research warrant particular scrutiny, given that these groups face significantly higher risks of adverse maternal and infant health outcomes [38, 39] that could be mitigated by psychological intervention [40].
Black participants, and Multiracial participants were also most likely to be excluded from participation due to night shift work. While both interventions tested in the present RCT were self-guided and app-based, allowing for intervention content to be delivered at participants’ convenience, the app did not have a tailored version of insomnia intervention techniques (e.g., sleep restriction) required for shift workers. Occupational demands, particularly shift work and job-related inflexibility, are social determinants of health that disproportionately impact Black individuals and are likely to limit their ability to meet scheduling requirements for many clinical trials [41].
White participants were the racial group most likely to be excluded due to current or planned use of antidepressant medication during the study. Further, Asian, Black, and Latina participants had smaller odds of exclusion due to current or planned antidepressant medication use compared to their White counterparts. This was unsurprising; in the USA, White individuals [42], including those who are pregnant [43], use antidepressants at higher rates than non-white racial groups or those of Latinx ethnicity. Several studies have documented that ethnic and racial minorities find psychiatric medications undesirable due to stigma and concerns about drug dependency, preferring psychotherapy instead [44–47]. While the relatively high exclusion rate of White participants at screening (55.7%) was primarily due to current or planned antidepressant use, White participants were screened at significantly higher rates than any other racial or ethnic group. Thus, White participants were still the largest group represented among eligible screeners. Given the much higher rate of screening response from White women across clinical trials, it is unlikely that eligibility criteria that exclude White women at higher rates will lead to the under-enrollment of this racial group [5].
Finally, just over half of Asian participants were excluded (54.7%) at screening, most often because their insomnia symptoms were not severe enough. Despite responding to an advertisement specifically recruiting pregnant people who were struggling to sleep, compared to their White counterparts, Asian participants had 2 times the odds of exclusion due to insomnia symptoms that did not reach clinical significance. Extant research suggests that underreporting of health issues—including sleep disorders—is prevalent among Asian Americans, a pattern often attributed to cultural stigma and norms [48, 49]. Many Asian cultures emphasize stoicism and resilience, leading individuals to minimize personal struggles or avoid acknowledging them altogether [50]. Further, the “model minority” stereotype perpetuates the expectation that Asian Americans are less likely to experience health challenges, adding pressure to conform to societal ideals of success and well-being [51] and may result in under-reporting of insomnia symptoms. Additionally, there may be a need for existing insomnia screening tools to be evaluated for cultural invariance to ensure their validity across diverse groups, or to develop more sensitive screening tools. While confirmatory factor analyses of the ISI have demonstrated the screener performed equally well across White and Black participants [52], similar analyses have not been conducted with Asian participants or other racial groups.
The analysis of screening data has inherent limitations. For example, all psychiatric disorders and medical data (e.g., gestational age) were measured via self-report. At later, more intensive screening steps prior to randomization, participants provide pregnancy documentation (e.g., an ultrasound) and participate in a diagnostic clinical interview to ensure these eligibility criteria are corroborated. However, at this initial screening step, there are necessarily fewer ethically allowable ways of confirming self-reported data. The use of targeted recruitment efforts to identify pregnant women, rates of exclusion similar to those of other prenatal insomnia trials [53], and recent validation studies demonstrating that the generally high accuracy of self-reported psychiatric history [54] temper these concerns. Additionally, two of the racial/ethnic groups in our sample—Latina Black (n = 71) and American Indian/Alaska Native/Native Hawaiian and Pacific Islander (n = 72)—had substantially smaller sample sizes compared to other groups. While representation of these groups—each 1.7% of the sample—reflect national demographics, the smaller sample sizes resulted in wider confidence intervals for estimates of trial eligibility. Trials with higher screening rates of Latina Black and American Indian or Indigenous participants may be needed to achieve sufficient power to detect statistically significant differences in odds of study exclusion.
Conclusion
While the disparities in eligibility identified in the present study can be interpreted within the context of prenatal intervention trials, the process of evaluating racial/ethnic differences in eligibility criteria has much broader implications. Differences in trial exclusion can contribute to the under-enrollment of minoritized pregnant people in RCTs for behavioral health. Examining the impact of eligibility criteria on sample diversity can help investigators weigh decisions about the rigor of their criteria against sample representativeness. When disparities in exclusion are found, trialists can assess whether the eligibility criteria are justified or if specific criteria are too strict, unintentionally leading to homogeneous samples. An additional possibility is to alter recruitment plans to better reach specific ethnic or racial groups found to be excluded at high rates [55] with the goal of enhancing screening to make up for lower conversion (i.e., eligibility) rates. Our findings and those of others [21–23] identify that Black individuals—including those who are Multiracial or Latina—are more likely to be excluded from clinical trials despite demonstrating interest. Given the persistent under-enrollment of non-White individuals [5], examining racial and ethnic differences in eligibility criteria is a data-driven strategy that can be leveraged to improve participant diversity in RCTs and promote more equitable clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Turner BE, Steinberg JR, Weeks BT, Rodriguez F, Cullen MR. Race/ethnicity reporting and representation in US clinical trials: a cohort study. Lancet Reg Health - Am. 2022;11:100252.10.1016/j.lana.2022.100252 PMC 930276735875251 · doi ↗ · pubmed ↗
- 2Peter SC, Pfund RA, Ginley MK. Increased demographic representation in randomized control trials for gambling disorder in the United States is needed: a systematic review. J Gambl Stud. 2021;37(3):1025–41.10.1007/s 10899-021-10055-w 34255242 · doi ↗ · pubmed ↗
- 3Jean-Louis G, Seixas AA. The value of decentralized clinical trials: Inclusion, accessibility, and innovation. Science. 2024;385(6711):eadq 4994.10.1126/science.adq 499439172847 · doi ↗ · pubmed ↗
- 4Hughson J anne, Woodward-Kron R, Parker A, Hajek J, Bresin A, Knoch U, et al. A review of approaches to improve participation of culturally and linguistically diverse populations in clinical trials. Trials. 2016;17(1):263.10.1186/s 13063-016-1384-3PMC 488098527229153 · doi ↗ · pubmed ↗
- 5Evaluating inclusion and exclusion criteria in clinical trials. U.S. Food and Drug Adminstration. 2018:1–10. Available from: https://www.fda.gov/media/134754.
- 6Rodríguez-Torres E, González-Pérez MM, Díaz-Pérez C. Barriers and facilitators to the participation of subjects in clinical trials: an overview of reviews. Contemp Clin Trials Commun. 2021;23:100829.10.1016/j.conctc.2021.100829 PMC 835864134401599 · doi ↗ · pubmed ↗
- 7Lebron CN, Mitsdarffer M, Parra A, Chavez JV, Behar-Zusman V. Latinas and maternal and child health: research, policy, and representation. Matern Child Health J. 2023. Available from: https://link.springer.com/10.1007/s 10995-023-03662-z. Cited 2025 Feb 21.10.1007/s 10995-023-03662-z PMC 1056031437029892 · doi ↗ · pubmed ↗
- 8Valerio VC, Downey J, Sgaier SK, Callaghan WM, Hammer B, Smittenaar P. Black-White disparities in maternal vulnerability and adverse pregnancy outcomes: an ecological population study in the United States, 2014–2018. Lancet Reg Health – Am. 2023;20. Available from: https://www.thelancet.com/journals/lanam/article/PIIS 2667-193X%2823%2900030-3/fulltext?stream=top. Cited 2025 Mar 4. 10.1016/j.lana.2023.100456 PMC 1012211537095772 · doi ↗ · pubmed ↗