Abemaciclib-induced myocarditis in early breast cancer: a case report
Alexander JP Fulton, Mun Cheang, Maria TA Wetscherek, Paul Cacciottolo, Jean E Abraham

TL;DR
A patient with early breast cancer developed abemaciclib-induced myocarditis, and a genetic variant in RHBDF2 may have contributed to the condition.
Contribution
This is one of the first reports of abemaciclib-induced myocarditis in early breast cancer, suggesting a potential genetic predisposition via RHBDF2.
Findings
Abemaciclib was linked to acute myocarditis in a patient with early breast cancer.
A germline RHBDF2 missense variant was identified, potentially affecting growth factor signaling and cardiomyocyte injury.
Discontinuation of abemaciclib and initiation of cardiac treatment led to rapid recovery of cardiac function.
Abstract
Abemaciclib, a selective cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor, is standard adjuvant therapy for hormone receptor (HR)-positive, HER2-negative early breast cancer. While gastrointestinal and haematologic toxicities are well recognised, cardiotoxicity—particularly myocarditis—is extremely rare. To our knowledge, myocarditis has not previously been reported in early breast cancer. This case describes a case of acute abemaciclib-induced myocarditis and explores a potential genetic predisposition involving an RHBDF2 germline variant affecting growth factor signalling pathways. A 39-year-old female with high-risk HR-positive, HER2-negative early breast cancer commenced adjuvant abemaciclib with letrozole following completion of chemotherapy and radiotherapy. Within 24 h, she developed acute chest pain with an elevated troponin I (8457 ng/L), new T-wave inversion on her ECG, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
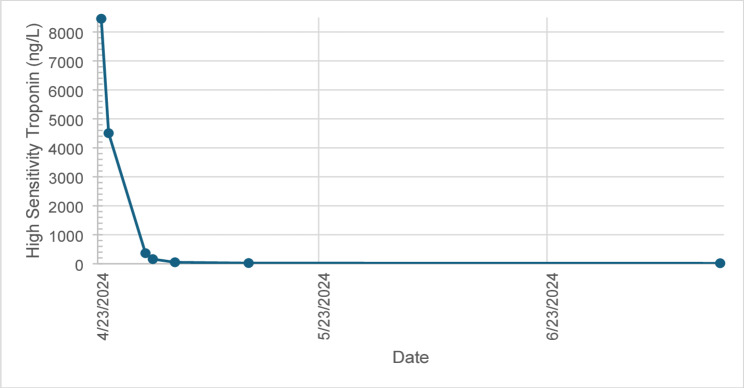 Figure 1
Figure 1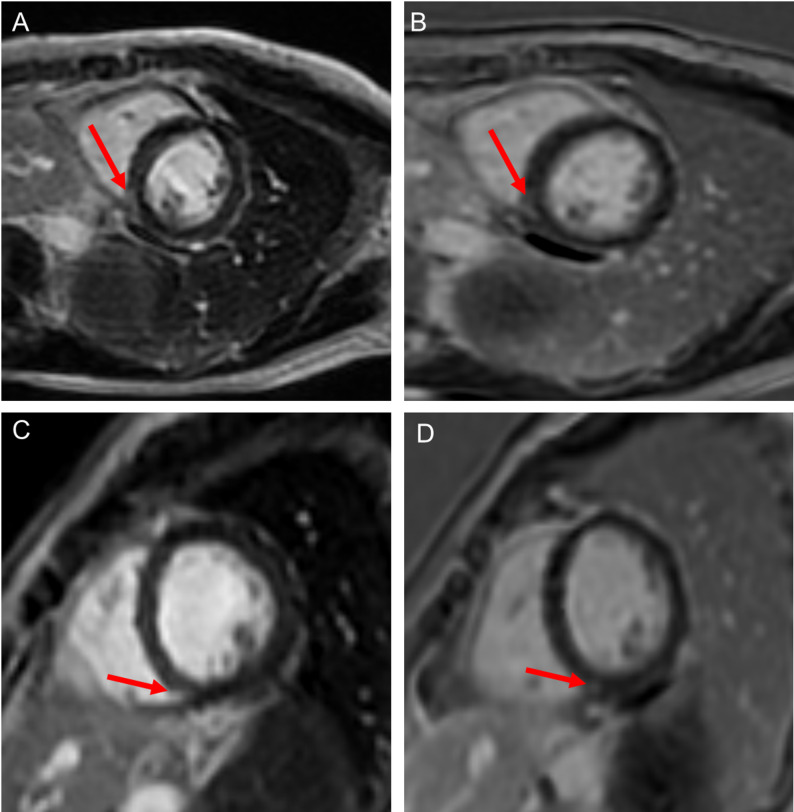 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Breast Cancer Therapies · HER2/EGFR in Cancer Research · Breast Cancer Treatment Studies
Introduction
Targeting of cyclin-dependent kinases 4 and 6 (CDK4/6) has improved clinical outcomes in hormone receptor (HR) positive breast cancer. Abemaciclib, a selective CDK 4/6 inhibitor, is used as the standard of care adjuvant treatment of high-risk HR-positive, HER2-negative early breast cancer. While commonly associated with gastrointestinal and hematologic toxicities, cardiotoxicity, particularly myocarditis, is a rare but potentially life-threatening adverse effect. To date, cardiotoxicity from CDK4/6 inhibitors is infrequently reported and as such is rarely listed as a potential toxicity [1]. Here we describe a patient with early breast cancer that developed acute myocarditis after commencing adjuvant abemaciclib.
Clinical background
A 39-year-old female with a history of early breast cancer (T2 N3 M0, grade 3 invasive carcinoma, HR-positive, HER2-negative) was initiated on adjuvant letrozole (2.5 mg once daily) in February 2024 and abemaciclib (150 mg twice daily) on 22nd April 2024. She had recently completed adjuvant paclitaxel, epirubicin and cyclophosphamide chemotherapy followed by 40 Gy in 15 fractions of right chest wall and right axilla radiotherapy. She had no anthracycline exposure prior to her breast cancer diagnosis. As such, her total epirubicin exposure was 360mg/m^2^ between 19th December 2023 and 30th January 2024.
Her past medical history included a bicuspid aortic valve and an aneurysmal atrial septum. She had no known history of coronary artery disease. Her uncle had hypertrophic cardiomyopathy but she had no personal or family history of myocardial infarction. Baseline echocardiography at the time of diagnosis demonstrated normal cardiac function with no regional wall motion abnormalities. She notably had a germline missense variant in RHBDF2, a gene that plays a role in the modulation of growth factor signalling such as epidermal growth factor (EGF) and tumour necrosis factor alpha (TNFα) [2, 3]. This variant had not previously been reported but was predicted to have a functional consequence using Polyphen modelling.
Clinical course
One day after starting abemaciclib, she presented to the emergency department with gradual onset heavy central chest pain radiating into her left arm and associated with intermittent palpitations. Her symptoms then eased over 1.5 h. On examination, her vital signs were within normal limits: BP 114/65 mmHg, HR 76 bpm, RR 14/min, temperature 36.5 °C, and oxygen saturation 100%. Cardiac auscultation revealed an ejection systolic murmur. Her respiratory examination was unremarkable, and she had no notable peripheral oedema.
She had no preceding viral symptoms and had not experienced similar symptoms previously.
Diagnostic workup
Initial laboratory investigations demonstrated a normal white cell count and C reactive protein but an elevated troponin I level at 8457 ng/L (normal < 39 ng/L), indicating myocardial injury. An electrocardiogram (ECG) demonstrated normal sinus rhythm with new T wave inversion in leads V5, V6, II, III, AVF. Transthoracic echocardiogram (TTE) imaging revealed a left ventricular ejection fraction (LVEF) of 47% (reduced from a baseline of 61%, GLS − 20%) with basal, midinferior and inferolateral wall hypokinesis. CT aorta imaging with contrast demonstrated no acute aortic syndrome, pulmonary emboli or evidence of significant coronary artery plaque or stenosis. Serial troponin I levels rapidly reduced until normalisation post abemaciclib discontinuation (Fig. 1). Subsequent cardiac magnetic resonance imaging (CMR) demonstrated an improved systolic function (LVEF 64%) with evidence of late gadolinium enhancement in the mid-inferoseptum, consistent with resolving acute myocarditis (Fig. 2). Given the clinical presentation, imaging findings, and recent initiation of abemaciclib, a diagnosis of abemaciclib-induced acute myocarditis was made.
Fig. 1. Serial high sensitivity troponin levels demonstrate a raised level at the onset of chest pain, followed by normalisation after discontinuation of abemaciclib on 24/04/2024
Fig. 2. Cardiac magnetic resonance (CMR) imaging at baseline (A, B) and 3-month follow-up (C, D). (A) Late gadolinium enhancement (LGE) short-axis (SAX) image of the mid-inferoseptum. (B) Single-shot LGE SAX of the mid-inferoseptum. (C) LGE SAX at follow-up. (D) Single-shot LGE SAX at follow-up
Management
Abemaciclib was immediately discontinued and cardioprotective bisoprolol (1.25 mg daily) and ramipril (1.25 mg daily) were commenced. She was admitted to the inpatient cardiology unit after her initial high sensitivity troponin I was raised.
Cardiac telemetry monitoring demonstrated no evidence of significant arrhythmia.
Following exclusion of acute coronary or aortic syndromes, she was diagnosed with acute myocarditis associated with transient LV dysfunction and she received standard of care cardioprotective management. She was discharged home on day 10 of admission after the CMR demonstrated a resolving myocarditis, along with no recurrence of her symptoms and a normalising high sensitivity troponin I.
She subsequently restarted letrozole on 30/4/24 and discontinued abemaciclib indefinitely.
Follow-up and outcome
Repeat CMR imaging on 11th August 2024, after four months of bisoprolol and ramipril therapy, showed an improvement in LVEF to 68% and almost complete resolution of subepicardial LGE (Fig. 2). Her bisoprolol and ramipril are ongoing as cardioprotective treatment. She continued letrozole and did not restart abemaciclib. To date, she has no evidence of breast cancer recurrence.
Discussion
We report a case of acute myocarditis occurring within 24 h of initiating abemaciclib. Prior to this treatment, she had normal cardiac function and no identifiable risk factors for acute cardiac dysfunction. Following discontinuation of abemaciclib and commencement of cardioprotective therapy with bisoprolol and ramipril, her cardiac function improved and ultimately returned to baseline. Importantly, no changes or persistent reductions in cardiac function were observed during prior letrozole monotherapy.
Abemaciclib is a selective inhibitor of cyclin‑dependent kinases 4 and 6 (CDK4/6). By blocking phosphorylation of the retinoblastoma protein, it prevents cell cycle progression from G1 to S phase, resulting in cell cycle arrest, inhibition of tumour proliferation, and ultimately cell death. CDK4/6 inhibitors in combination with endocrine therapy are licensed for hormone receptor‑positive, HER2‑negative breast cancer. Abemaciclib, when used alongside endocrine therapy, has become the standard adjuvant treatment for patients at high risk of recurrence. This includes those with ≥ 4 positive lymph nodes or 1–3 positive nodes with either grade 3 disease or tumour size ≥ 50 mm. The addition of abemaciclib significantly improved invasive disease‑free survival at 48 months from 78.6% to 85.5% when compared with endocrine therapy alone [4].
CDK4/6 inhibitor toxicity and discontinuation are often associated with diarrhoea, myelosuppression, liver dysfunction and fatigue [4]. Cardiac toxicity has been previously reported as a ‘rare’ toxicity from abemaciclib and, in the metastatic setting, heart failure/cardiomyopathy have been observed in 5.8% of patients receiving this treatment [5]. However, abemaciclib associated acute myocarditis, to our knowledge, has not been previously reported in early breast cancer [1]. It is therefore important to highlight this potentially long term detrimental cardiovascular toxicity as an associated risk of abemaciclib treatment.
The exact underlying mechanism of abemaciclib induced myocarditis is unclear. Preclinical studies have suggested CDK4/6 inhibition leads to alteration in potassium and sodium channel activity, vascular inflammation and left ventricular remodelling [5]. Recent preclinical data suggests that CDK4/6 inhibition leads to cardiomyocyte apoptosis secondary to activation of the Hippo signalling pathway [6]. In this context, one possible explanation for the cardiomyocyte toxicity observed in this patient is the presence of a germline RHBDF2 missense variant. This could influence growth factor signalling pathways, including TNFα signalling. Enhanced TNFα signalling has been reported to interact with and potentially amplify Hippo pathway activity [7]. It is possible that this could have contributed to the patient’s presentation, however, this remains a speculative hypothesis based on limited evidence and would require dedicated mechanistic studies to explore further. In our case, 24–48 h of exposure to abemaciclib led to acute myocardial dysfunction, perhaps implicating a direct cardiomyocyte toxicity of abemaciclib. Early recognition and discontinuation enabled recovery in cardiac function within days. It is unclear, however, if more prolonged treatment may have led to irreversible reduction in cardiac function in an individual without prior cardiac risk factors.
Conclusion
This case highlights a serious complication of abemaciclib therapy that may not be as rare as previously thought. Clinicians should be aware of the potential for abemaciclib-induced myocarditis and consider it in the differential diagnosis when patients present with new cardiac symptoms. Prompt intervention and supportive care can result in favourable outcomes within days of commencing abemaciclib, though the long-term effects of more extended use remain unclear. Multidisciplinary oncology and cardiology input is essential, and CMR imaging may assist in identifying myocarditis as the underlying cause. Further research into the mechanism of CDK4/6 inhibitor induced cardiomyocyte injury is warranted. This would enable identification of individuals particularly at risk of cardiotoxicity with abemaciclib and perhaps a subsequent tailored approach to their treatment.
Patient perspective
As a patient facing cancer treatment, knowing both the benefits and potential risks of therapy is deeply important. Experiencing unexpected side effects, like heart inflammation from abemaciclib, can be frightening and overwhelming. Greater understanding and reporting of these rare toxicities are vital—not only so doctors can monitor and manage them promptly, but also so patients can make truly informed decisions about their care. I hope that sharing my experience can help future patients feel safer and better prepared as they navigate their treatment journey.
The reference list from the paper itself. Each links out to its DOI / PubMed record.