Relationship between maternal lipid profile during the third trimester and the risk of small-for-gestational-age birth: exploring inadequate gestational weight gain as a mediator
Maissam Ghanem, Weiming Wang, Huaqi Zhang, Jin Liu, Qian Liang, Nianhong Yang

TL;DR
High maternal HDL-C levels in the third trimester are linked to a higher risk of small-for-gestational-age births, especially when combined with low triglycerides.
Contribution
This study identifies a novel association between maternal lipid profiles and SGA risk, independent of inadequate gestational weight gain.
Findings
High HDL-C levels were associated with a 1.54-fold increased risk of SGA infants.
The combination of high HDL-C and low TG levels significantly predicted SGA (aRR, 1.77).
Inadequate gestational weight gain did not mediate the observed associations.
Abstract
Lipids play crucial roles in maternal and foetal metabolism; however, their effects on birth weight remain unclear. Moreover, the potential mediating role of inadequate gestational weight gain (iGWG) in this association remains unexplored. The objective of this study was to assess maternal lipid profiles in the third trimester and their associations with the risk of small-for-gestational-age (SGA) infants, focusing on the combined effects of high-density lipoprotein cholesterol (HDL-C) and triglycerides (TG). This study also examined whether iGWG influenced this relationship. Data were sourced from the Tongji Maternal and Child Health Cohort. Maternal fasting lipid levels were measured during the third trimester and birth information was retrieved from medical records. Log-Poisson regression analysis was performed to assess the relationship between lipid tertiles and SGA risk. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
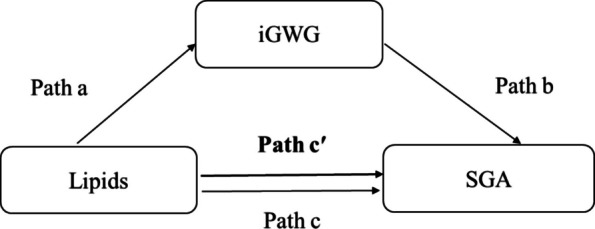 Figure 1
Figure 1- —National Program of the Basic Research Project of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Birth, Development, and Health · Pregnancy and preeclampsia studies
Background
Pregnancy induces profound changes in the body, primarily driven by the growing demand for metabolic fuels required to support foetal growth and development. Concurrently, hormonal changes lead to modifications in the lipid profile across pregnancy trimesters [1]. Between weeks 9 and 13, lipid components, including total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C), begin to rise and continue to increase gradually as pregnancy progresses [2].
Disruptions in maternal lipid metabolism, including those associated with gestational diabetes mellitus [3] and preeclampsia, have been reported as potential contributors to unfavourable pregnancy outcomes [4]. These disturbances may jeopardise foetal growth, thereby increasing the risk of adverse birth outcomes [5, 6]. Among these, small-for-gestational-age (SGA) at birth poses a critical challenge to infant health and has been linked to an increased risk of neonatal mortality [7]. SGA reflects impaired foetal growth and is associated with perinatal complications such as hyperbilirubinemia and hypoglycaemia. Additionally, it may lead to long-term consequences, including poor academic performance in adolescence and an increased risk of metabolic syndrome in adulthood [8, 9]. Evidence indicates that children born SGA, even those who subsequently achieved normal weight in early childhood, commonly exhibit abnormal lipid profiles [10], which may predispose them to future cardiovascular disorders.
The associations of SGA with smoking [11], low pre-pregnancy body mass index (BMI) [12], and reduced height thresholds have been well characterised [13]. Moreover, gestational dyslipidaemia has been identified as a potential risk factor for SGA [14]. The substantial risk of SGA, along with its largely irreversible nature, underscores the urgent need for effective strategies to predict and prevent its occurrence.
Birth weight and gestational weight gain (GWG) are closely linked, as GWG is a key indicator of maternal nutritional status throughout pregnancy. Adequate GWG is crucial for foetal growth and development, whereas inadequate GWG (iGWG) has been associated with unfavourable delivery outcomes, including low birth weight, SGA, and preterm birth [15]. Additionally, associations between GWG and altered lipid profiles, placental weight, and placenta-to-birth weight have been documented [16]. However, whether iGWG mediates the relationship between altered lipid profiles and birth outcomes remains unclear. It is hypothesised that iGWG mediates the association between lipid profile disturbances and SGA birth. Understanding this relationship is vital for improving prenatal care strategies and supporting risk mitigation.
The present study aimed to (1) explore the association between maternal lipid profiles during the third trimester and SGA risk, with a focus on the combined effects of HDL-C and TG levels, and (2) investigate whether iGWG mediates this association.
Methods
Study population and design
Data were obtained from the Tongji Maternal and Child Health Cohort (TMCHC), a prospective cohort study designed to investigate the effects of maternal lifestyle and nutrition on maternal and neonatal outcomes in Wuhan, Hubei Province, China [17]. Recruitment was conducted at three research hospitals in Wuhan from January 2013 to May 2016. Pregnant women attending their first antenatal visit before 16 weeks of gestation were enrolled and followed up at regular intervals throughout pregnancy.
Participants were eligible if they met the following criteria: (1) singleton pregnancy; (2) provision of blood samples during the third trimester for lipid assessment; and (3) availability of follow-up data on birth outcomes. Women with multiple gestations and pre-existing conditions, such as diabetes, hypertension, thyroid disorders, and known infectious diseases (e.g. viral hepatitis, tuberculosis, etc.) were excluded. A flowchart of participant selection is provided in Supplementary Fig. S1.
Lipid assessment
Throughout the third trimester, fasting maternal blood samples were collected by trained nurses. TG, TC, LDL-C, and HDL-C were measured using the glycerol phosphate oxidase-p-aminophenazone (GPO-PAP), cholesterol oxidase–peroxidase and 4-aminoantipyrine phenol (CHOD-PAP), surfactant scavenging, and catalase scavenging methods, respectively. All measurements were performed using a Mindray BS-200 automatic biochemical analyser (Shenzhen, China) in accordance with standard procedures.
Birth outcomes
Data on newborn characteristics, including birth weight, sex, and gestational age at delivery (in weeks), were obtained from medical records. Infants with birth weights below the 10th percentile for sex- and gestational-age–specific standards were classified as SGA, according to Chinese reference standards [18].
Covariates
At enrolment, data on maternal obstetric and medical histories, socioeconomic status, and lifestyle characteristics were collected using a face-to-face questionnaire. Recorded variables included maternal age, educational level, parity, ethnicity, smoking habits, average monthly income, physical activity, and alcohol consumption. Moderate-intensity physical activity (≥ 30 min, at least three times per week) was considered regular during pregnancy.
Gestational age was initially estimated using the date of the last menstrual period and was adjusted using ultrasonography when discrepancies were identified during early pregnancy. Pre-pregnancy BMI was calculated as the weight before pregnancy (kg) divided by the square of the height (m^2^). According to the Working Group on Obesity in China, participants were classified into four BMI categories: (1) underweight, BMI < 18.5 kg/m^2^; (2) normal weight, 18.5 ≤ BMI < 24.0 kg/m^2^; (3) overweight, 24.0 ≤ BMI < 28.0 kg/m^2^; and (4) obese, BMI ≥ 28.0 kg/m^2^ [19]. Pre-pregnancy weight was self-reported, whereas height and weight were measured at enrolment.
Total GWG was calculated by subtracting the pre-pregnancy weight from the weight recorded before delivery. GWG was classified according to the recommended ranges for Chinese women across BMI categories [20]: 11.0–16.0 kg for individuals classified as underweight; 8.0–14.0 kg for those within the normal weight range; 7.0–11.0 kg for those classified as overweight; and 5.0–9.0 kg for those classified as obese. GWG was further categorised as inadequate (below the recommended range), adequate (within the range), and excessive (above the range).
Statistical analysis
Continuous variables with normal distributions are summarised as mean ± standard deviation (SD), whereas non-normally distributed variables are presented as median (interquartile range [IQR]). Categorical variables are presented as frequencies (n) and percentages (%). Log-Poisson regression analysis was performed to examine the association between lipid levels and risk of SGA. Relative risks (RRs) and adjusted RRs (aRRs), along with 95% confidence intervals (CIs), were calculated. The RR of SGA was estimated across lipid-level tertiles, with the middle tertile (T2) as the reference group.
Models were adjusted for the following covariates: maternal ethnicity (Han Chinese or other), age, parity (primiparous or multiparous), pre-pregnancy BMI, regular physical activity in early pregnancy (yes/no), educational level (< 12 years, 12–15, ≥ 16 years according to the number of completed schooling), monthly average income (< 5000, 5000–9999 or ≥ 10,000 Chinese Yuan), gestational age at blood sampling, neonatal sex (male/female), and total weight gain. Data analyses were performed using IBM SPSS Statistics version 26.0 for Windows (IBM Corp., Armonk, NY, USA). Mediation analysis was conducted following the steps described by Baron and Kenny to evaluate whether iGWG mediated the association between lipid levels and SGA [21] (Fig. 1). To determine whether lipids significantly influenced SGA (path c) and iGWG (path a), a log-Poisson regression model was applied. The association between iGWG and SGA (path b) was then examined. Finally, the effect of lipids on SGA while accounting for iGWG as a categorical variable (yes, no) was analysed (path c′). The mediation effect was evaluated using the regression coefficients of pathways a and b (a × b). Analyses were performed using the mediation package in R software version 4.3.2 (R Foundation for Statistical Computing, Austria). A P-value of < 0.05 was considered statistically significant.Fig. 1. Mediation diagram illustrating the role of iGWG in the association between maternal lipid levels and SGA. Path a represents the association between lipid levels and iGWG (log-Poisson regression). Path b represents the association between iGWG and SGA (log-Poisson regression). Path c represents the association between lipid levels and SGA without adjusting for iGWG (log-Poisson regression). Path c': represents the association between lipid levels and SGA after adjusting for iGWG (log-Poisson regression). iGWG: inadequate gestational weight gain, SGA: small-for-gestational-age
Results
Baseline characteristics of the study population
Table 1 summarises the demographic characteristics of the 2,721 participants. The mean pre-pregnancy BMI was 20.8 ± 2.7 kg/m^2^. Overall, 116 (4.26%), 921 (33.85%), and 1,684 (61.89%) participants had inadequate, adequate, and excessive GWG, respectively. Male and female newborns accounted for 54.1% and 45.9% of births, respectively. A total of 262 (9.6%) newborns were classified as SGA. Participants with iGWG were less likely to be primiparous and had a higher prevalence of gestational diabetes mellitus and SGA births.Table 1. Demographic characteristics of the study population stratified by total GWG according to Chinese guidelines^a^Maternal characteristicsOverall n = 2721Inadequate n = 116Adequate n = 921Excessive n = 1684P-valueAge (years)28.5 ± 3.529.6 ± 4.128.7 ± 3.428.4 ± 3.40.001Height (cm)160.3 ± 5.0160.0 ± 4.8159.9 ± 4.9160.5 ± 5.00.019Pre-pregnancy BMI (kg/m^2^)20.8 ± 2.720.9 ± 3.820.5 ± 2.621.0 ± 2.7 < 0.001 Underweight518 (19.0)46 (39.7)240 (26.1)232 (13.8) Normal weight1874 (68.9)47 (40.5)610 (66.2)1217 (72.3) Overweight and Obese329 (12.1)32 (19.8)71 (7.7)235 (14.0)Ethnicity (Han Chinese)2656 (97.6)115 (99.1)897 (97.4)1644 (97.6)0.543Educational level0.164 < 12 years356 (13.1)16 (13.8)109 (11.8)231 (13.7) 12–15 years742 (27.3)29 (25.0)232 (25.2)481 (28.6) ≥ 16 years1547 (56.9)70 (60.3)548 (59.5)929 (55.2) Unknown76 (2.8)1(0.9)32 (3.5)43 (2.6)Monthly income (CNY)0.313 < 50001005 (36.9)45 (38.8)317 (34.4)643 (38.2) 5000–99991125 (41.3)47 (40.5)391 (42.5)687 (40.8) ≥ 10,000543 (20.0)21 (18.1)199 (21.6)323 (19.2) Unknown48 (1.8)3 (2.6)14 (1.5)31 (1.8)Primiparous2241 (82.4)81 (69.8)736 (79.9)1424 (84.6) < 0.001Regular physical activity in early pregnancy (yes)650 (23.9)21 (18.1)223 (24.2)406 (24.1)0.325Drinking before pregnancy (yes)329 (12.1)13 (11.2)105 (11.4)211 (12.5)0.671Smoking before pregnancy (yes)85 (3.1)2 (1.7)21 (2.3)62 (3.7)0.098Hypertensive disorders of pregnancy (yes)141 (5.2)5 (4.3)22 (2.4)114 (6.8) < 0.001Gestational diabetes mellitus (yes)300 (11.0)27 (23.3)120 (13.0)153 (9.1) < 0.001Total weight gain (kg)15.9 ± 4.77.2 ± 2.712.2 ± 2.118.6 ± 3.5 < 0.001Gestational age at blood sampling (weeks)39.4 ± 1.339.1 ± 1.339.2 ± 1.339.5 ± 1.2 < 0.001Gestational age at delivery39.46 ± 1.2239.17 ± 1.1839.30 ± 1.2739.56 ± 1.18 < 0.001Preterm infant70 (2.6)5 (4.3)38 (4.1)27 (1.6) < 0.001TG (mmol/L)3.29 (1.71)3.13 (1.82)3.23 (1.68)3.33 (1.72)0.042TC (mmol/L)6.16 (1.55)6.21 (1.59)6.24 (1.53)6.10 (1.54)0.027HDL-C (mmol/L)1.78 (0.54)1.79 (0.52)1.78 (0.53)1.78 (0.55)0.770LDL-C (mmol/L)3.43 (1.36)3.48 (1.40)3.54 (1.40)3.37 (1.33)0.001Male newborn1472 (54.1)67 (57.8)517 (56.1)888 (52.7)0.180Birth weight (g)3344.7 ± 417.03104.3 ± 349.83237.3 ± 377.03420 ± 423.1 < 0.001SGA262 (9.6)26 (22.4)116 (12.6)120 (7.1) < 0.001CNY, Chinese Yuan, 1 CNY ≈ 0,14 US$BMI Body mass index, TG Triglycerides, TC Total cholesterol, HDL-C High-density lipoprotein cholesterol, LDL-C Low-density lipoprotein cholesterol, SGA Small-for-gestational-age^a^Non-normally distributed data are expressed as median (IQR), whereas normally distributed data are presented as mean ± SD. Categorical variables are reported as n (%)P-values were calculated using the chi-square test, Kruskal–Wallis test and one-way ANOVA for categorical, non-normally distributed and normally distributed variables, respectively
Associations between lipid profile and birth outcomes
Table 2 presents the RR and aRR, along with 95% CIs, for SGA across tertiles of maternal lipid levels during the third trimester. Compared with the middle tertile (T2), the highest tertile (T3) of HDL-C was associated with an increased risk of SGA (aRR, 1.54; 95% CI, 1.15–2.07). The lowest tertile of TG (T1) showed a marginal, but non-significant association with SGA risk (aRR, 1.27; 95% CI, 0.95–1.70) compared with T2. These findings were consistent after excluding preterm births (2.6% of the total).Table 2. Associations between lipid levels during the third trimester and SGA riskLipid profileNSGAn** (%)Crude model (95% CI)Adjusted model (95% CI)^1^P-valueTG (mmol/L) < 2.79906108 (11.92)1.30 (0.97, 1.73)1.27 (0.95, 1.70)0.556 2.79–3.9090283 (9.20)Ref. (1.00)Ref. (1.00)- ≥ 3.9191371 (7.78)0.85 (0.62, 1.16)0.91 (0.66, 1.26)0.109TC (mmol/L** < 5.6790785 (9.37)0.92 (0.68, 1.23)1.05 (0.78, 1.42)0.758 5.67–6.6590192 (10.21)Ref. (1.00)Ref. (1.00)- ≥ 6.6691385 (9.31)0.91 (0.68, 1.22)0.88 (0.65, 1.19)0.391HDL-C (mmol/L) < 1.6291269 (7.57)0.90 (0.65, 1.24)0.95 (0.68, 1.33)0.772 1.62–1.9690276 (8.43)Ref. (1.00)Ref. (1.00)- ≥ 1.97907117 (12.90)1.53 (1.15, 2.04)1.54 (1.15, 2.07)0.004LDL-C (mmol/L) < 3.0590989 (9.79)1.02 (0.76, 1.38)1.12 (0.82, 1.51)0.478 3.05–3.8889886 (9.58)Ref. (1.00)Ref. (1.00)- ≥ 3.8991487 (9.52)0.99 (0.74, 1.34)0.90 (0.66, 1.22)0.478CI Confidence interval, SGA Small-for-gestational-age, TG Triglycerides, TC Total cholesterol, HDL-C High-density lipoprotein cholesterol, LDL-C Low-density lipoprotein cholesterolRef., reference^1^Adjusted for maternal education, ethnicity, age, monthly average income, regular physical activity in early pregnancy, pre-pregnancy BMI, parity, gestational age at blood sampling, total weight gain, and neonatal sex‘n (%)’ values represent the number and percentage of SGA births within each category
Low TG and high HDL-C combination in relation to SGA risk
Given the individual associations of TG and HDL-C with the risk of SGA, potential interactions between TG and HDL-C were examined. A significant interaction was identified between low TG and high HDL-C levels (P for interaction = 0.019; Supplementary Table S1). To further examine this combined effect, women were categorised into four groups based on their TG and HDL-C tertiles: (1) middle tertile (T2) for both TG and HDL-C (reference group); (2) low TG (T1) and high HDL-C (T3); (3) high TG (T3) and low HDL-C (T1); and (4) all other combinations. Mothers with low TG and high HDL-C levels had a significantly higher risk of delivering an SGA infant compared with the reference group (aRR, 1.77; 95% CI, 1.10–2.87; Table 3).Table 3. Associations between combined TG and HDL-C levels during the third trimester and SGA riskCombined TG and HDL-CNSGAn** (%)****Crude model (95% CI)**Adjusted model (95% CI)^1^P-value**Middle TG (2.79–3.90) and middle HDL-C (1.62–1.96)30224 (7.95)Ref. (1.00)Ref. (1.00)-Low TG (< 2.79) and high HDL-C (≥ 1.97)42863 (14.72)1.85 (1.16, 2.96)1.77 (1.10, 2.87)0.020High TG (≥ 3.91) and low HDL-C (< 1.62)43029 (6.74)0.85 (0.49, 1.46)0.94 (0.54, 1.64)0.839All other combinations for TG and HDL-C1561146 (9.35)1.18 (0.76, 1.81)1.19 (0.76, 1.85)0.447CI Confidence interval, SGA Small-for-gestational-age, TG Triglycerides, HDL-C High-density lipoprotein cholesterolRef., reference^1^Adjusted for maternal education, ethnicity, age, monthly average income, regular physical activity in early pregnancy, pre-pregnancy BMI, parity, gestational age at blood sampling, total weight gain, and neonatal sex‘n (%)’ values represent the number and percentage of SGA births within each category
This association was further confirmed in sensitivity analyses restricted to women with normal pre-pregnancy BMI, which demonstrated an even stronger association (aRR, 2.28; 95% CI, 1.16–4.47; Supplementary Table S2).
Potential influence of iGWG on the relationship between lipid profiles and SGA risk
GWG has been reported to influence both lipid levels and the risk of SGA. As shown in Table 4, the associations of high HDL-C levels and combined low TG–high HDL-C with SGA remained significant after adjustment for iGWG (path c'). No significant indirect effects through iGWG were observed (a × b). Although iGWG was significantly associated with SGA (path b), it was not associated with maternal lipid levels (path a). The robustness of these findings was supported by sensitivity analyses, excluding women with gestational diabetes mellitus and hypertensive pregnancy disorders (Supplementary Table S3). These results indicate that maternal lipid levels markedly influence foetal growth and SGA risk independent of iGWG.Table 4. Mediation of iGWG in the association between maternal lipid levels and SGA riskPath cPath c'Path aPath bMediating effectLipidsCoefficient (95% CI)****Coefficient (95% CI)****Coefficient (95% CI)****Coefficient (95% CI)****a × bP**-value**TG < 2.790.209 (− 0.184, 0.610)0.212 (− 0.180, 0.613)0.008 (− 0.137, 0.153)**0.690 (0.240, 1.103)***0.00550.914TG ≥ 3.91 − 0.110 (− 0.566, 0.338) − 0.126 (− 0.581, 0.323)0.010 (− 0.138, 0.158)**0.690 (0.240, 1.103)0.00680.895HDL-C < 1.620.219 (− 0.262, 0.707)0.249 (− 0.233, 0.736) − 0.009 (− 0.154, 0.136)0.666 (0.215, 1.079)−0.00580.905HDL-C ≥ 1.970.794 (0.379, 1.233)*****0.797 (0.381, 1.236)***0.003 (− 0.143, 0.148)**0.666 (0.215, 1.079)***0.00170.972TG (< 2.79) and HDL-C (≥ 1.97)**1.216 (0.468, 2.115)*****1.195 (0.446, 2.094)***0.036 (− 0.196, 0.271)**0.648 (0.197, 1.061)*0.02330.766The table presents the coefficients and 95% CIs for each stage of the mediation analysis, estimated using the mediation package with log-Poisson models adjusted for maternal ethnicity, education, age, monthly average income, parity, regular physical activity in early pregnancy, pre-pregnancy BMI, gestational age at blood sampling and neonatal sex. Path c represents the association between lipid levels and SGA, whereas path c' represents this association after adjusting for iGWG (yes, no). Path a represents the association between lipid levels and iGWG, and path b represents the association between iGWG and SGA. The significance of a × b was assessed using the Sobel test. * P < 0.05CI Confidence interval, TG Triglycerides, HDL-C High-density lipoprotein cholesterol
Discussion
This study examined maternal lipid profiles during the third trimester of pregnancy and their association with the risk of delivering SGA newborns. High HDL-C levels were positively associated with an increased SGA risk. Furthermore, an elevated risk of SGA was particularly observed among mothers with low TG and high HDL-C levels. The findings of this study revealed that the combination of low TG and high HDL-C levels during the third trimester was a significant risk factor for SGA infants, suggesting a potential interaction between these lipid components in influencing foetal growth. These associations were independent of iGWG.
Maternal lipid levels may influence the placental vascular endothelium, thereby disrupting placental function and potentially leading to underperfusion and abnormal birth weight. Nevertheless, the precise mechanisms through which maternal lipid profiles affect neonatal outcomes remain unclear. During pregnancy, trophoblasts take up glycerol and free fatty acids released from HDL-C and LDL-C via placental enzyme-catalysed hydrolysis. These absorbed components are subsequently re-esterified to support foetal development [22]. Under normal physiological conditions, HDL-C possesses anti-inflammatory and antioxidant properties that help protect against cardiovascular diseases [23] and play a crucial role in removing cholesterol and other lipids from peripheral tissues [24]. Although this study demonstrated the association between high HDL-C levels and an increased SGA risk, this finding may be explained by alterations in HDL-C function under pathological conditions. Such changes can impair vascular endothelial cell function [25], potentially affecting placental function and foetal growth. Elevated HDL-C concentrations have been associated with unfavourable pregnancy outcomes, including spontaneous preterm delivery [26]. Elevated HDL-C concentrations during pregnancy may reflect placental dysfunction resulting from altered lipid metabolism or peroxidation. This dysfunction may contribute to SGA by reducing the transfer of essential nutrients or by interfering with placental blood flow, thereby disrupting the normal transfer of HDL-C to the foetus. Consistently, SGA infants have been reported to exhibit lower cord blood HDL-C concentrations compared with infants born appropriate for gestational age [27]. Accordingly, elevated maternal HDL-C levels may result from placental dysfunction, which decreases the amount of maternal HDL-C transported to the foetus [28].
Consistent with these findings, a previous study reported that high HDL-C levels during the third trimester were markedly associated with an increased SGA risk among women with appropriate GWG [29]. Additionally, elevated HDL-C levels at 36 weeks of gestation have been associated with an increased risk of developing SGA. Furthermore, reduced newborn size has been linked to alterations in maternal HDL-C levels over the course of pregnancy [30]. Mothers who gave birth to SGA infants exhibited higher HDL-C levels compared with those who delivered normal birth weight infants [28]. However, evidence regarding the relationship between HDL-C levels and birth weight remains inconsistent, with some studies reporting inverse associations, particularly among women classified as overweight or obese [31, 32].
Based on the findings of the present study, TG levels approached statistical significance in relation to SGA, suggesting a potential role of TG in influencing birth weight. Low maternal TG levels during pregnancy were found to be more likely to result in SGA infants, whereas elevated maternal TG levels were associated with a higher risk of large-for-gestational-age (LGA) infants [33]. Furthermore, the prevalence of SGA has demonstrated negative correlation with HDL-C concentrations in underweight women before pregnancy and with TG levels across all BMI groups [5]. In addition, a meta-analysis reported that higher maternal TG levels during pregnancy were associated with a lower risk of SGA [34].
Maternal TG levels are well recognised for their substantial role in foetal development, despite TG being unable to cross the placenta directly. TG is broken down by endothelial-placental lipase, generating free fatty acids that are absorbed by placental trophoblasts. This process, in turn, influences placental development and angiogenesis [35, 36]. However, dysregulation of placental lipid transport may result in an insufficient nutrient and energy supply to the foetus, thereby contributing to SGA outcomes. Fatty acids may act as growth factors and compete with hormones for albumin binding, thereby increasing free hormone levels in the circulation and potentially affecting intrauterine foetal growth [37]. Importantly, free fatty acids can contribute to insulin resistance, which may have detrimental effects on birth outcomes [38]. As insulin resistance increases the activation of amino acid transport systems, it promotes protein synthesis and decreases lipolysis, potentially impairing glucose tolerance [38]. Maternal nutrition plays a pivotal role in foetal development, as it directly affects the supply of essential nutrients and energy. Maternal diet has been reported to influence the regulation of lipid levels [39, 40]. Furthermore, an animal study has suggested that maternal malnutrition during pregnancy can restrict foetal growth [41]. Infants born with SGA may experience inadequate foetal growth owing to inadequate maternal weight gain, which may also lead to inadequate adipose tissue energy storage and insufficient TC and TG delivery to the foetus during late pregnancy [42]. Various mechanisms contribute to SGA outcomes, including placental dysfunction, obstetric complications, and foetal genetic abnormalities. In addition, smoking during pregnancy has been consistently associated with low birth weight [43, 44]. In contrast, some studies have found no significant effect of TG on neonatal birth weight [32] or HDL-C levels [45]. These discrepancies may be attributable to variations in sample size, population characteristics, gestational age at blood sampling, or other factors.
Based on the assessment of the combined effects of TG and HDL-C levels, the co-occurrence of low TG and high HDL-C levels markedly increased the risk of SGA. Nevertheless, this finding highlights the potential relevance of maternal lipid levels in predicting foetal growth, including among women with normal pre-pregnancy BMI. These results also underscore the importance of considering lipid combinations, rather than evaluating individual lipids in isolation, in prenatal risk assessment. Notably, low TG and high HDL-C levels during the third trimester emerged as significant predictors of SGA infants.
As previously noted, the objective of the mediation analysis was to clarify the mechanisms underlying the association between lipid profiles and SGA. iGWG is an important concern during pregnancy owing to its association with several adverse maternal and foetal outcomes. The analysis indicated that the observed associations between high HDL-C, the low TG–high HDL-C combination, and SGA could not be explained by iGWG. This finding suggests that the relationship between lipid levels and SGA is not related to iGWG. These results highlight the potential value of integrating lipid profile monitoring into prenatal care, which may help inform more tailored strategies for managing pregnancy and enhancing foetal well-being.
Thus, monitoring lipid profiles during pregnancy or obtaining lipid measurements before pregnancy may help improve maternal lipid status at an early stage. Given that women undergoing preconception may be more willing to modify their lifestyles, pre-pregnancy lipid level assessment may offer an opportunity to reduce subsequent risks and enable timely intervention [46]. Monitoring lipid levels during pregnancy also provides an opportunity to adapt to lifestyle changes that may improve pregnancy outcomes and support the well-being of mothers and their foetuses. Although therapeutic options for modifying lipid profiles during pregnancy remain limited, these results highlight the need for further research on early identification and intervention, particularly among high-risk women with abnormal lipid profiles. Such efforts may enhance monitoring and personalised care, thereby improving pregnancy outcomes.
Strengths and limitations
This study has several important implications. It was conducted using standardised data and biological samples collected from a large prospective observational cohort study. Data on lifestyle factors and maternal characteristics during pregnancy were collected and analysed, allowing adjustment for several important confounding factors. In addition, fasting blood samples were obtained in the morning to minimise the influence of non-fasting conditions on lipid levels.
Despite these strengths, some limitations should be considered. Pre-pregnancy weight was self-reported, which may introduce reporting bias. However, this is a common practice and is generally considered acceptable, as weight was measured at enrolment in early pregnancy, when body weight did not change significantly [47]. Additionally, a considerable proportion of participants were Han Chinese, which may limit the generalisability of the findings to other communities or ethnic populations. Given the observational nature of this study, the results may also have been influenced by unmeasured confounding factors, despite adjustment for several known covariates. In particular, unmeasured factors such as dietary intake and maternal metabolic status may have influenced the observed associations. Although genetic risk factors are an important consideration, they were not included in this analysis. Nonetheless, investigating these factors will be the central focus of the next phase of this research. Given the limited sample size with longitudinal lipid data, this study focused on maternal lipid profiles measured during the third trimester. However, analyses of the available data indicated that both baseline lipids and their subsequent changes during gestation strongly predicted third-trimester lipid concentrations. Although repeated measurements would offer a more comprehensive understanding of lipid dynamics in relation to SGA, this study underscores the significant association between third trimester maternal lipid status and SGA.
This study did not perform sensitivity analyses using alternative birth-weight references or growth charts, such as those from the WHO or INTERGROWTH-21ST. However, similar associations employing various reference charts have been reported in earlier literature. For example, a Japanese study [33] identified SGA and LGA infants using Japanese neonatal charts based on gestational ages at birth. The INTERGROWTH-21ST standards for birth weight were used in rural Gambia to define SGA [42]. According to both studies, SGA risk and infant weight at birth correlated with lipid levels throughout pregnancy, supporting the robustness of the findings of the present study. The classification of SGA in this study was based on Chinese reference standards, which are widely used in studies conducted in China and provide relevant context for the study population. However, birth-weight standards vary across regions owing to differences in socioeconomic status, nutritional habits, healthcare access, and environmental conditions. Consequently, the findings of this study may not fully capture the diversity of birth weight distributions across all regions of China.
This study demonstrated that lipid levels were a notable risk factor for SGA among women with normal pre-pregnancy BMI. However, it is important to note that the analyses of the associations between HDL-C and TG levels in the underweight and overweight/obese pre-pregnancy BMI groups were not feasible owing to small sample sizes. In addition, the mediation analysis employed Baron and Kenny’s approach, which remains a widely accepted and clear framework. Although more recent methods, such as the VanderWeele approach, are available, the Baron and Kenny method remains relevant and has been used in a recent study [48]. Further research is needed to clarify the mechanisms through which lipid profiles influence foetal growth outcomes.
Conclusions
This study demonstrated that an increased SGA risk was associated with high HDL-C levels and that this risk was further elevated when high HDL-C co-occurred with low TG levels. Importantly, the association between maternal lipid profiles and SGA appeared to be independent of iGWG.
Clinically, in addition to managing GWG, it is also important to monitor the lipid profiles during pregnancy, particularly in cases of unexpectedly low TG and high HDL-C levels, to mitigate the risk of SGA.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang W, Li N, Wang X, Zhang X, Tu M, Lin L, et al. Remnant cholesterol is associated with gestational diabetes mellitus: a cohort study. J Clin Endocrinol Metab. 2023;dgad 262.10.1210/clinem/dgad 26237167108 · doi ↗ · pubmed ↗
- 2Obesity LP-M, Voerman E, Santos S, Inskip H, Amiano P, Barros H, et al. Association of gestational weight gain with adverse maternal and infant outcomes. JAMA. 2019;321:1702.10.1001/jama.2019.3820 PMC 650688631063572 · doi ↗ · pubmed ↗
- 3Wang Y, Chen Z, Zhang F. Association between maternal lipid levels during pregnancy and delivery of small for gestational age: A systematic review and meta-analysis. Front Pediatr. 2022;10:934505. 10.3389/fped.2022.934505 PMC 958233436275062 · doi ↗ · pubmed ↗
- 4Society CN. Weight Monitoring Evaluation During Pregnancy Period of Chinese Women. 2021; https://www.cnsoc.org/other Notice/392100200.html. Accessed Sept 2024.