Preventive and therapeutic effects of ginsenosides on myocardial ischemia-reperfusion injury in animal models: a systematic review and meta-analysis
Hongyi Yue, Yunfei Jia, Ruohao Sun, Zhuoyang Song, Wenhua Li

TL;DR
This study reviews how ginsenosides from ginseng can protect the heart from injury caused by reduced blood flow and reperfusion in animal models.
Contribution
This is the first systematic review and meta-analysis evaluating ginsenosides' preventive and therapeutic effects on myocardial ischemia-reperfusion injury in animals.
Findings
Ginsenosides significantly reduce myocardial infarct size and improve hemodynamic performance in MIRI models.
Ginsenosides attenuate MIRI-induced inflammation, oxidative stress, and cardiomyocyte apoptosis.
Pre-ischemic administration of ginsenosides provides greater protection than post-reperfusion treatment.
Abstract
Myocardial ischemia-reperfusion injury (MIRI) markedly impairs cardiac functional recovery and represents a major determinant of adverse outcomes in patients with ischemic heart disease. Ginsenosides, the principal bioactive constituents of ginseng, exert significant cardioprotection against MIRI. This review systematically summarizes and analyzes in vivo (animal) studies to clarify the efficacy and underlying mechanisms of ginsenosides in MIRI. The PubMed, EMbase, Web of Science, Cochrane Library, CNKI, WanFang, and Cqvip databases were systematically searched from inception to 31 July 2024. In vivo studies evaluating ginsenosides pretreatment or post-treatment in models of MIRI were identified. Outcome measures comprised myocardial infarct size and indices of hemodynamic performance, myocardial injury, apoptosis, inflammation, and oxidative stress. A meta-analysis was conducted with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
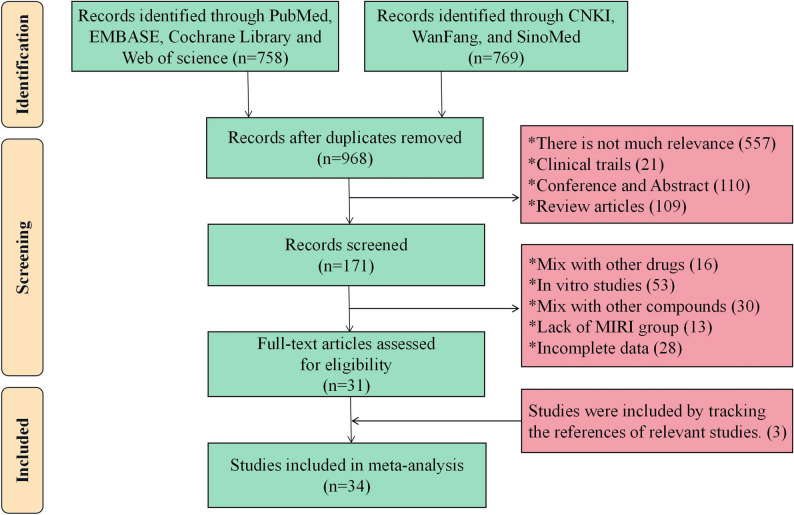 Figure 1
Figure 1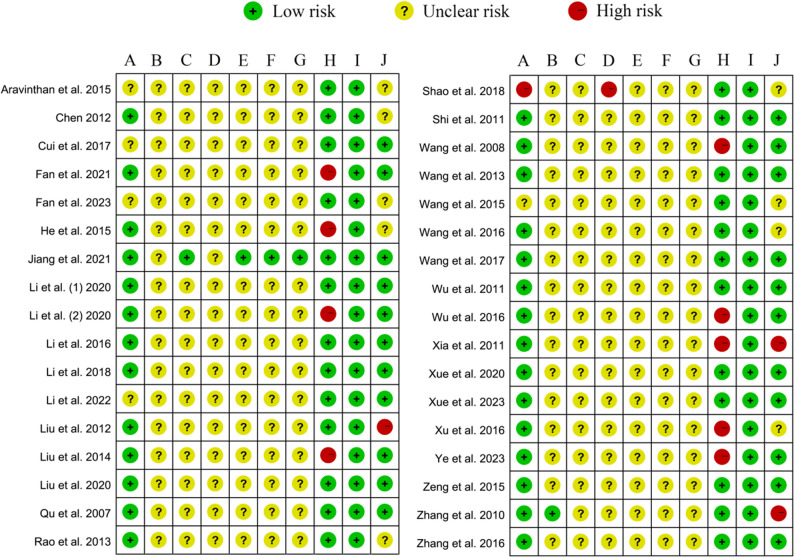 Figure 2
Figure 2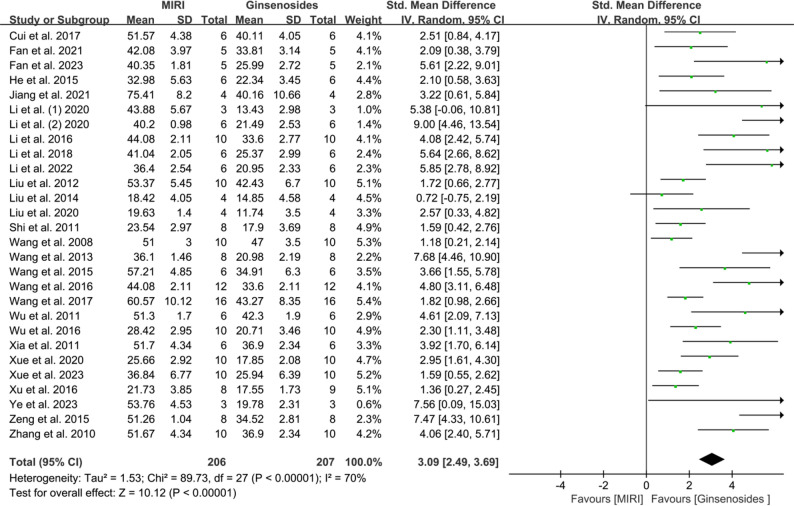 Figure 3
Figure 3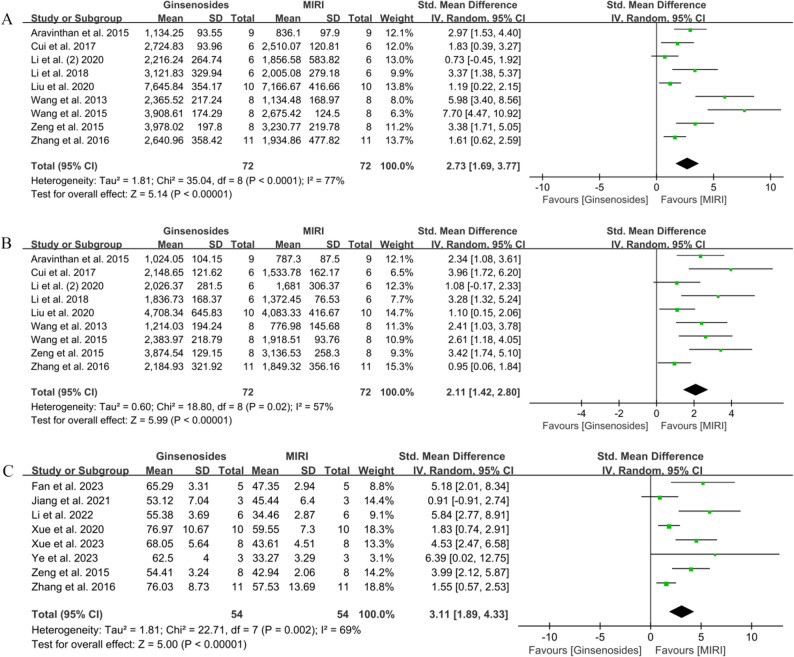 Figure 4
Figure 4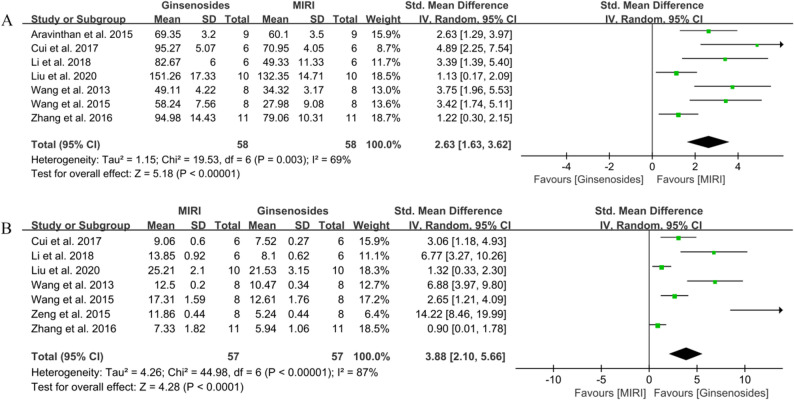 Figure 5
Figure 5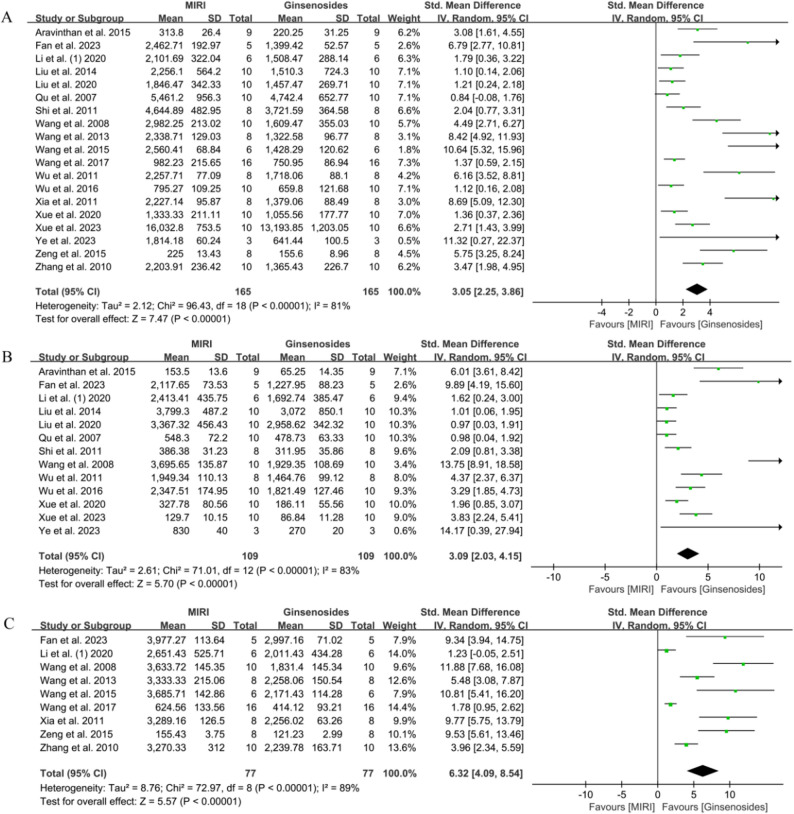 Figure 6
Figure 6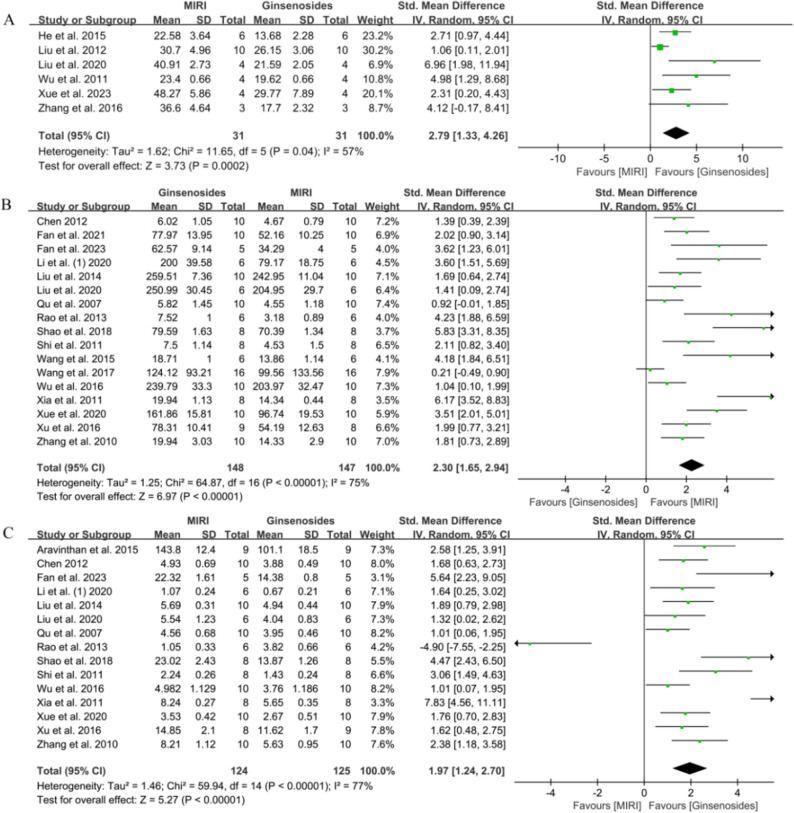 Figure 7
Figure 7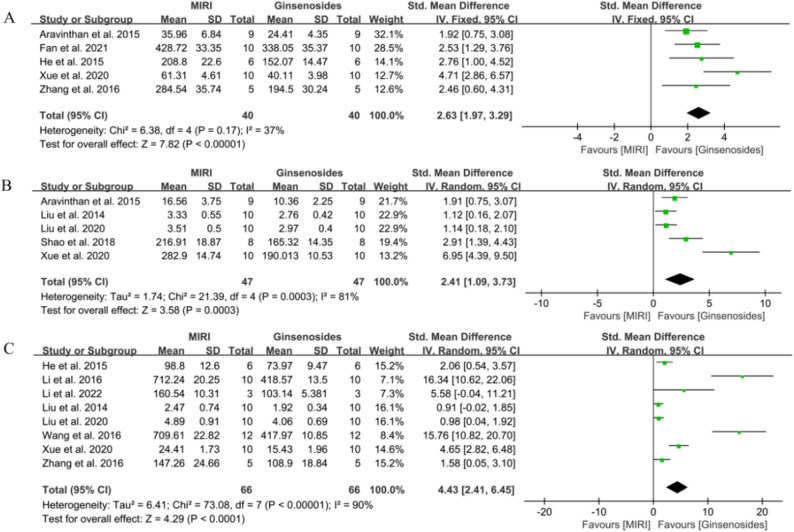 Figure 8
Figure 8- —The Postgraduate Research Innovation and Practice Project of Xizang Minzu University
- —A comparative study of the active ingredients of Rhodiola rosea in Tibetan medicine, salidroside and kaempferol, against myocardial injury caused by cytokine storm
- —Mechanism study of the role of Fritillariae Cirrhosae Bulbus component peimisine in inflammatory response
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGinseng Biological Effects and Applications · Traditional Chinese Medicine Analysis · Cardiac Ischemia and Reperfusion
Introduction
Ischemic heart disease (IHD) is one of the most common and serious cardiovascular diseases in clinical practice. According to relevant epidemiological surveys, approximately 4 million people die from IHD in China each year [1]. Restoring blood perfusion is an effective and important method for the treatment of IHD, but the reperfusion process often leads to secondary injuries such as myocardial edema, cell membrane rupture, mitochondrial swelling, and excessive sarcomere contraction, which in turn leads to myocardial ischemia-reperfusion injury (MIRI) [2, 3]. MIRI severely affects survival after revascularization in patients with IHD and greatly reduces the benefit of reperfusion therapy and the recovery of cardiac function [4]. To date, the pathogenesis of MIRI has remained incompletely understood, and no effective therapeutic strategy is available. Consequently, identifying effective approaches to preventing and treating MIRI has become a major focus of cardiovascular research.
As a world-famous traditional Chinese medicinal herb, Panax ginseng C. A. Mey. (ginseng) has long been recognized for its significant therapeutic value; recent studies have increasingly indicated that its efficacy mainly relies on its primary active constituents, ginsenosides [5, 6]. Ginsenosides are triterpenoid glycosides divided into four types: protopanaxadiol, protopanaxatriol, ocotillol, and oleanolic acid. The types differ in structure, properties and activity, but their pharmacological effects are similar: antioxidant and anti-inflammatory actions, immune modulation and autophagy induction [7]. A substantial body of evidence indicates that ginsenosides confer marked cardioprotection in vivo and in vitro by suppressing homocysteine-induced superoxide-anion generation and endothelial dysfunction and by protecting human vascular endothelial cells from oxidized-LDL-mediated injury [8, 9]. In addition, ginsenoside pretreatment reverses the increases in reactive oxygen species production and the decreases in superoxide dismutase activity in vascular smooth muscle cells that are induced by resistin and acetylated LDL, thereby preventing vascular injury [10]. These pharmacological mechanisms align with the recognized therapeutic mechanisms of MIRI, making it highly significant to evaluate the cardioprotective effect of ginsenosides in MIRI treatment.
Thus far, although numerous preclinical studies have confirmed ginsenosides as promising agents against MIRI, their efficacy remains neither systematically summarized nor critically evaluated. To fill this gap, we provide a comprehensive assessment of the protective effects of ginsenosides on MIRI and delineate the underlying mechanisms, offering a theoretical framework for the prevention, treatment and clinical translation of MIRI.
Methods
This article aims to reveal the effects of ginsenosides on MIRI in preclinical studies through systematic review and meta-analysis. In this study, we strictly adhered to the guidelines of the PRISMA statement [11]. Furthermore, to ensure transparency and traceability, this meta-analysis was registered with PROSPERO (registration number: CRD42024569208).
Search strategy
A systematic literature search was conducted across seven databases: PubMed, Embase, Web of Science, Cochrane Library, CNKI, WanFang and Cqvip. We aimed to identify all potentially relevant studies to ensure the meta-analysis was based on the most comprehensive and up-to-date scientific evidence. The search period extended from the inception of the database to July 31, 2024. The search formula was constructed as follows: [(Ginseng) OR (Ginsenosides) OR (Ginseng Saponin) OR (Panaxosides) OR (Sanchinosides)] AND [(Myocardial Ischemia) OR (Ischemic Heart Disease) OR (Myocardial Reperfusion) OR (Myocardial Ischemia-Reperfusion Injury) OR (Injuries, Myocardial Reperfusion) OR (Myocardial Reperfusion Injuries) OR (Reperfusion Injuries, Myocardial) OR (Reperfusion Injury, Myocardial) OR (Injury, Myocardial Reperfusion)]. To minimize the risk of missing relevant studies, we also tracked the citations of selected articles.
Inclusion and exclusion guidelines
According to the PICOS principle, literature was included in this meta-analysis if the following conditions were met: (1) population: animals; (2) intervention: administration of ginsenosides drugs (either before or after MIRI); (3) comparison: the control group was given saline or no treatment for the experimental animals; (4) outcome: myocardial infarction size, apoptosis rate, hemodynamic indices [maximum rate of left ventricular pressure rise (+ dp/dtmax), maximum rate of left ventricular pressure decrease (-dp/dtmax), left ventricular ejection fraction (LVEF), left ventricular systolic pressure (LVSP), left ventricular end-diastolic pressure (LVEDP)], myocardial injury markers [lactate dehydrogenase (LDH), creatine kinase (CK), creatine kinase MB (CK-MB)], oxidative stress markers [superoxide dismutase (SOD), malondialdehyde (MDA)], and inflammation markers [tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and interleukin-1β (IL-1β)]; (5) study design: animal studies of MIRI were constructed using ligation of the left anterior descending (LAD) branch of the coronary artery or other methods (langendorff perfusion system; ligation of the right atrial vein).
The literature will be excluded if the following conditions are met: (1) during administration, ginsenosides are administered along with other drugs; (2) low relevance to the core themes of this study; (3) reviews, abstracts, conferences, clinical trials, and in vitro experiments; (4) the study suffers from missing data; (5) the MIRI modeling was unsuccessful.
Data extraction
After applying the predefined inclusion and exclusion criteria, we screened the articles and then independently extracted the data. This information includes: (1) the name of the first author and the year in which the article was published; (2) species, sex, weekly age, and weight of the animals used in the study; (3) types of narcotic drugs; (4) methods of constructing disease models and the duration of ischemia-reperfusion; (5) duration of the intervention group and method of intervention; (6) classes of ginsenosides monomers; (7) outcome indicators and the mechanism of action of the treatment. When the intervention arm included different ginsenoside doses, we combined the subgroup data into a single treatment group using the methodology recommended by the Cochrane Handbook [12]. This approach ensures that the combined data accurately reflects the treatment effects of the different conditions. In addition, when articles presented data graphically, we digitized them with GetData Graph Digitizer 2.22 for statistical analysis [13].
Risk of bias and quality assessment
Included articles were independently assessed based on the SYRCLE statement’s recommended risk assessment scale for experiments on animals [14]. The assessment process covered the following aspects: (A) the level of detail at which the sequence was generated; (B) whether animal characteristics were accurately described at baseline; (C) whether the allocation sequence is adequately concealed; (D) whether the animal’s rearing process is randomized; (E) blinding of researchers; (F) randomness in outcome measurement; (G) blinding researchers during outcome assessment; (H) treatment of Incomplete Results; (I) whether there is a risk of selective reporting of results; (J) whether other potential biases exist. All entries were categorized as having a high, low, or unclear risk of bias, and the summary was visualized in RevMan 5.4. The reliability of outcomes was then assessed using GRADE [15]. Correction and verification of the raw data were conducted by the corresponding author, WH. In cases of disagreement during the evaluation process, the final decision was also made by WH.
Statistical analysis
The forest plot was generated using RevMan 5.4 (The Cochrane Collaboration, London, England), and the statistical significance level was set at P < 0.05. In forest plots, parameter variables were consistently represented as mean ± standard deviation. For studies that reported data as medians and quartiles, the means and standard deviations were estimated using the methods outlined by Wan et al. and Hozo et al. [16, 17]. For the effect indicators in the forest plots, the standardized mean difference (SMD) was consistently used due to variations in age and sex among the included studies, as well as the involvement of multiple species [18]. In order to assess whether there was publication bias in the included studies and whether the results were stable, we utilized Stata/MP 14.0 (StataCorp, College Station, TX, USA) software and employed a variety of methods for testing. Specifically, this involved Egger’s test, funnel plot, and sensitivity analysis [19, 20]. When publication bias was detected in the results, we employed the trim-and-fill method to account for potentially missing studies and recalculated the effect size. Additionally, to assess heterogeneity among the included studies, we performed the I² test. If P < 0.10 or I² > 50%, this indicated significant heterogeneity between studies, in which case we selected the random-effects model for analysis. If P > 0.10 or I² < 50%, heterogeneity was not significant, and we chose the fixed-effects model for analysis [21]. In addition, subgroup analyses, meta-regression analyses, and sensitivity analyses were conducted to investigate potential causes of heterogeneity. The subgroup and meta-regression analyses focused on five outcomes: myocardial infarct size, LDH, CK-MB, SOD, and MDA, as these outcomes were covered in a sufficient number of studies. Sensitivity analysis involved removing each study individually and observing the impact of this action on I² values.
Results
Selection of included studies
The process of literature retrieval is shown in Fig. 1. After implementing the established search strategy, we screened a total of 1,527 articles in seven databases, including 758 articles in English and 769 articles in Chinese. During the initial screening process, 559 duplicate studies were identified and removed using NoteExpress software, leaving 968 candidates. For further screening, the abstracts and titles of the remaining articles were briefly read by two researchers, HY and YJ. Among these, 557 articles with low relevance to the core topic, 110 conference abstracts, 21 clinical studies, and 109 reviews were excluded. A detailed reading of the remaining 171 articles led to the further exclusion of 140 papers. Among these, 46 were mixed with other drugs or compounds, 53 were in vitro studies, 13 lacked model groups, and 28 had incomplete data. We then tracked down three eligible studies from the citations of Zheng et al. [22] Ultimately, 34 papers were included in this meta-analysis [23–56].
Fig. 1. Flowchart of study selection based on PRISMA
Characteristics of the included studies
This study pooled 34 studies covering 505 animals, with 253 animals in the intervention group and 252 animals in the model group. Of all the studies, SD rats were the most common, appearing in 24 studies [25–28, 30–33, 35–37, 40–49, 54–56]. This was followed by Wistar rats, which were used in 6 studies [24, 38, 39, 50, 51, 53]. Additionally, one study utilized Duncan-Hartley guinea pigs [23], and two studies involved C57 BL/6 J mice [29, 34]. The MIRI model is commonly constructed using coronary artery ligation. The duration of ischemia was 0.5 h in most studies, 0.75 h in two studies [42, 53], and 1 h in one study [23]. Regarding the time to reperfusion, a reperfusion time of 2 h was more common, while other studies varied from 1 to 24 h. Ether and pentobarbital were the primary anesthetics utilized during model construction. Nevertheless, it is noteworthy that seven studies did not specify the use of anesthetics [29, 31, 33, 36, 45, 51, 53]. The main modes of administration of ginsenosides include intragastric administration, intravenous injections, and intraperitoneal injections. Regarding the use of drug monomers, 17 studies used ginsenoside Rb [24, 25, 29, 31, 32, 35–38, 41, 42, 45, 47–50, 55], 8 studies used ginsenoside Rg [28, 30, 33, 34, 39, 44, 52, 56], 4 studies used ginsenoside Rh [26, 27, 40, 46], and 5 studies used other types of ginsenoside monomers [23, 43, 51, 53, 54]. Other basic characteristics are shown in Table 1.
Table 1. Basic characteristics of the included studiesStudy andYearSpecies and genderWeek old and WeightAnestheticModeling methodTreatment groupMI/RI TimeDrug (Monomer)PretreatmentOutcomesMechanism ofactionTime of administrationMode of administration Aravinthan et al. 2015Duncan-Hartley guinea pigs, MaleND, 300–350 gPentobarbitalLigation of the right atrial vein14 daysTake orally1 h/2 hGinseng total saponinNob, c, e, g, h, k, n, oInflammation↓, Oxidative stress↓ Chen 2012Wistar rats, MaleND, 220–260 gEthyletherLigation of LAD7 daysIntragastric administration0.5 h/3 hGinsenoside Rb1Noj, kAntioxidant enzyme activity↑, Oxidative stress↓, eNOS level↑ Cui et al. 2017SD rats, MaleND, 230–270 gUrethaneLigation of LAD30 min before MIRIIntravenous injection0.5 h/1.5 hGinsenoside Rb1Yesa, b, c, e, fRhoA signaling pathway↓, Energy metabolism disorder↓, Apoptosis↓ Fan et al. 2021SD rats, MaleND, 160–200 gPentobarbitalLigation of LAD10 daysIntravenous injection0.5 h/4 hGinsenoside Rh2Noa, j, oNLRP3 protein↓, Inflammation↓, Oxidative stress↓ Fan et al. 2023SD rats, Male1–8 weeks, NDPentobarbitalLigation of LAD10 days before MIRIIntravenous injection0.5 h/24 hGinsenoside Rh2Yesa, d, g, h, i, j, kNrf2↑/HO-1↑/NLRP3↓, Inflammation↓, Oxidative stress↓ He et al. 2015SD rats, Female or MaleND, 250–280 gUrethaneLigation of LAD15 days before MIRIIntragastric administration0.5 h/2 hGinsenoside Rg1Yesa, l, m, oNF-κB signaling pathway↓, Inflammation↓ Jiang et al. 2021C57BL/6 mice, Male6–8 or 8–12 weeks, NDNDLigation of LAD10 min before MIRIND0.5 h/15min, 24 h, 14d, 28dGinsenoside Rb1Yesa, dNADH dehydrogenase activity↓Li et al. (1) 2020SD rats, NDNDChloral hydrateLigation of LADAt the time of ligationIntramyocardial injection0.5 h/2 hGinsenoside Rg3Noa, g, h, i, j, kInflammation↓, Oxidative stress↓, Fibrosis↓Li et al. (2) 2020SD rats, MaleND, 200–300 gNDLangendorff perfusion system30 min before MIRIND0.5 h/0.5 h,1 hGinsenoside Rb1Yesa, b, cAutophagy↓, Myocardial contractility↑ Li et al. 2016SD rats, MaleND, 200–250 gPentobarbitalLigation of LAD5 min before reperfusionIntravenous injection0.5 h/2 hGinsenoside Rb1Noa, mp38α MAPK phosphorylation↓, Apoptosis↓ Li et al. 2018SD rats, MaleND, 240–260 gNDLigation of LAD150 min before MIRIFemoral venous catheter infusion0.5 h/1.5 hGinsenoside Rg1Yesa, b, c, e, fRhoA ↓/ ROCK↓, Activity of mitochondria respiratory Complexes↑, ATP5D↑ Li et al. 2022C57BL/6 mice, Male12 weeks, 22–25 gPentobarbitalLigation of LAD5 min before reperfusionvia caudal tail injection0.5 h/4 hGinsenoside Rg2Noa, d, mTAK1 phosphorylation↑, Necroptosis↓ Liu et al. 2012SD rats, MaleND, 250–300 gPentobarbitalLigation of LAD10 min before MIRIND0.5 h/2 hGinsenoside Rb1Yesa, lPI3K↑/Akt↑, Apoptosis↓ Liu et al. 2014SD rats, MaleND, 200–220 gNDLigation of LAD3 daysTake orally0.5 h/2 hGinsenoside Rb3Noa, g, h, j, k, m, nInflammation↓, Oxidative stress↓, Apoptosis↓ Liu et al. 2020SD rats, Male7–8 weeks, 220–240 gIsofluraneLigation of LAD3 daysTake orally0.5 h/2 hGinsenosides Rb2 and Rb3Noa, b, c, e, f, g, h, j, k, l, m, nInflammation↓, Oxidative stress↓, Apoptosis↓ Qu et al. 2007Wistar rats, Female or MaleND, 240–260 gEthyletherLigation of LAD7 daysIntragastric administration0.5 h/24 hGinsenoside RbNog, h, j, kAntioxidant enzyme activity↑, Oxidative stress↓, Platelet aggregation activity↓Rao et al. 2013Wistar rats, MaleND, 200–230 gEthyletherLigation of LAD7 daysIntragastric administration0.5 h/24 hGinsenoside Rg2Noj, kOxidative stress↓, eNOS level↑ Shao et al. 2018SD rats, MaleND, 180–250 gPentobarbitalLigation of LAD30 min before ischemiaIntraperitoneal injection0.5 h/24 hGinsenoside Rh2Yesj, k, nInflammation↓, Oxidative stress↓, Peripheral blood EPCs↑ Shi et al. 2011SD rats, NDND, 230–260 gChloraloseLigation of LAD3 daysTake orally0.5 h/24 hGinsenoside Rb3Noa, g, h, j, kOxidative stress↓, Microcirculatory disturbance↓ Wang et al. 2008SD rats, MaleND, 260–320 gPentobarbitalLigation of LAD10 min before ischemiaIntravenous injection0.75 h/2 hGinsenoside Rb1Yesa, g, h, iPI3K↑ /P-Akt↑ Wang et al. 2013SD rats, MaleND, 270–320 gPentobarbitalLigation of LAD30 min before MIRIIntraperitoneal injection0.5 h/3 hGinsenoside RdYesa, b, c, e, f, g, iROS↓, Apoptosis↓ Wang et al. 2015SD rats, MaleND, 260–280 gPentobarbitalLigation of LAD30 min before MIRIIntravenous injection0.5 h/3 hGinsenoside Rg3Yesa, b, c, e, f, g, i, jBcl-2↑/Bax↓, P-Akt↓/P-eNOS↓, Apoptosis↓ Wang et al. 2016SD rats, MaleND, 180–240 gNDLigation of LAD5 min before reperfusionIntravenous injection0.5 h/2 hGinsenoside Rb1Noa, mp38α phosphorylation↓, Apoptosis↓, Inflammation↓ Wang et al. 2017SD rats, MaleND, 180–200 gChloral hydrateLigation of LAD7 days before MIRIIntraperitoneal injection0.5 h/2 hGinsenoside Rh3Yesa, g, i, jBcl-2↑/Bax↓, Oxidative stress↓ Wu et al. 2011SD rats, MaleND, 250–300 gPentobarbitalLigation of LAD20 min before MIRIIntravenous injection0.5 h/2 hGinsenoside Rb1Yesa, g, h, lCardiomyocyte apoptosis↓, Cardiac dysfunction↓ Wu et al. 2016SD rats, Female or MaleND, 200–250 gPentobarbitalLigation of LAD2 daysIntragastric administration0.5 h/2 hGinsenoside Rb3Noa, g, h, j, kanti-lipid peroxide activities↑, Oxidative stress↓, Inflammation↓ Xia et al. 2011SD rats, MaleND, 220–280 gPentobarbitalLigation of LAD10 min before MIRIIntravenous injection0.5 h/2 hGinsenoside Rb1Yesa, g, i, j, kExpression of eNOS↑, Oxidative stress↓ Xue et al. 2020Wistar rats, FemaleND, 250–280 gPentobarbitalLigation of LAD3 days before MIRIIntragastric administration0.5 h/6 hGinsenoside Rb2Yesa, d, g, h, j, k, m, n, oSIRT1↑, Oxidative stress↓, Inflammation↓ Xue et al. 2023Wistar rats, MaleND, 210–230 gNDLigation of LAD7 days before MIRIIntragastric administration0.5 h/6 hGinsenoside RcYesa, d, g, h, lMitochondrial oxidative stress and apoptosis↓, SIRT1↑ Xu et al. 2016Rats, MaleND, 200–230 gEthyletherLigation of LAD5 daysIntraperitoneal injectionNDGinsenoside Rg2Noa, j, kAntioxidant activity↑, Free radical oxidative damage↓ Ye et al. 2023Wistar–Kyoto rats, Female8 weeks, NDNDLigation of LAD5 daysIntragastric administration0.75 h/NDGinsenoside ReNoa, d, g, hmiR-144-3p↑/SLC7A11↑ Zeng et al. 2015SD rats, MaleND, 270–320 gPentobarbitalLigation of LAD30 min before reperfusionIntraperitoneal injection0.5 h/2 hGinsenoside RdYesa, b, c, d, f, g, iNrf2↑/HO-1↑, Cardiac dysfunction↓ Zhang et al. 2010SD rats, MaleND, 220–280 gPentobarbitalLigation of LAD10 min before ischemiaIntravenous injection0.5 h/2 hGinsenoside Rb1Yesa, g, i, j, kOxidative stress↓, Free radical oxidative damage↓ Zhang et al. 2016SD rats, MaleND, 270–290 gChloraloseLigation of LAD7 daysIntragastric administration0.5 h/24 hGinsenoside Rg3Nob, c, d, e, f, l, m, oApoptosis↓, Inflammation↓ND No description, MIRI Myocardial ischemia/reperfusion injury, h Hour, LAD Left anterior descending branch, SD Sprague-Dawley, eNOS Endothelial nitric oxide synthase, Nrf2 NFE2-related factor 2, HO-1 Heme oxygenase-1, NLRP3 NOD-like receptor protein 3, NADH Nicotinamide adenine dinucleotide, TAK1 TGF-beta activated kinase 1, ROS Reactive oxygen species, SIRT1 Silent information regulator 1, ↓ reduction vs baseline, ↑ increase vs baseline^a^myocardial infarction size, ^b^maximum rate of left ventricular pressure rise, ^c^maximum rate of left ventricular pressure decrease, ^d^left ventricular ejection fraction, ^e^left ventricular systolic pressure, ^f^left ventricular end-diastolic pressure, ^g^lactate dehydrogenase, ^h^creatine kinase MB, ^i^creatine kinase, ^j^superoxide dismutase, ^k^malondialdehyde, ^l^apoptotic rate, ^m^tumor necrosis factor-alpha, ^n^interleukin-6, ^o^interleukin-1β
Quality assessment of included studies
We assessed the quality of the included studies using SYRCLE, a risk of bias assessment tool for animal experiments, and the relevant results were displayed in Fig. 2. Sequence generation and animal feeding were randomized in most of the studies. Only one study was rated as high risk because the sequence generation was grouped according to body weight, and some animals were on a high-fat diet during feeding. Furthermore, only one study explicitly reported randomization of animal baseline characteristics, animal grouping, investigator blinding, outcome measure blinding, and outcome assessment. The remaining studies were rated as an unclear risk because these aspects were not adequately described. None of the studies selectively reported results. Nine studies were rated as high risk in terms of animal loss because they experienced animal loss [26, 28, 31, 36, 42, 48, 49, 52, 53]. Regarding other risks of bias, four studies were also rated as high risk because of possible errors in the unit of analysis [35, 47, 49, 55].
Fig. 2. Risk of bias map of included studies based on the SYRCLE tool. A: Generation of random sequences; B: Characteristics of the baseline; C: Assign hidden situations; D: Randomness of animal feeding; E: Blinding of the experimenter; F: Randomness of outcome assessments; G: Blinding of outcome assessments; H: Integrity of result data; I: Selective reporting of results; J: Other biases
Quality evaluation of outcome indicators
This study provided a comprehensive assessment of all outcome indicators based on the GRADE rating methodology. The results showed (Table 2) that the proportion of outcome indicators of high quality was 33.33% (5/15), that of low quality was 53.33% (8/15), and that of moderate and very low quality were each 6.67% (1/15). The risk of bias and publication bias were the main reasons for downgrading the quality of evidence. In addition, due to exaggerated data for some of the outcome indicators, we had to adjust the quality of these results downward accordingly.
Table 2A GRADE summary of the protective effect of ginsenosides on MIRIOutcomesRelative effect (95% CI)LimitationsInconsistencyIndirectnessImprecisionPublication biasQualityInfarct sizeSMD, 3.09 (2.49, 3.69)−+++−⨁⨁◯◯, Low+dp/dtmaxSMD, 2.73 (1.69, 3.77)+++++⨁⨁⨁⨁, High-dp/dtmaxSMD, 2.11 (1.42, 2.80)+++++⨁⨁⨁⨁, HighLVEFSMD, 3.11 (1.89, 4.33)+++++⨁⨁⨁⨁, HighLVSPSMD, 2.63 (1.63, 3.62)+++++⨁⨁⨁⨁, HighLVEDPSMD, 3.88 (2.10, 5.66)+++++⨁⨁⨁⨁, HighLDHSMD, 3.05 (2.25, 3.86)−+++−⨁⨁◯◯, LowCK-MBSMD, 3.09 (2.03, 4.15)−+++−⨁⨁◯◯, LowCKSMD, 6.32 (4.09, 8.54)−+++−⨁⨁◯◯, LowSODSMD, 2.30 (1.65, 2.94)−+++−⨁⨁◯◯, LowMDASMD, 1.97 (1.24, 2.70)−−+++⨁⨁◯◯, LowApoptotic rateSMD, 2.79 (1.33, 4.26)++−++⨁⨁⨁◯, ModerateTNF-αSMD, 4.43 (2.41, 6.45)−+++−⨁⨁◯◯, LowIL-6SMD, 2.41 (1.09, 3.73)−+−+−⨁◯◯◯, Critically lowIL-1βSMD, 2.63 (1.97, 3.29)−+−++⨁⨁◯◯, LowLVEF Left ventricular ejection fraction, LVSP Left ventricular systolic pressure, LVEDP Left ventricular end-diastolic pressure, LDH Lactate dehydrogenase, CK-MB Creatine kinase MB, CK Creatine kinase, SOD Superoxide dismutase, MDA Malondialdehyde, *TNF-*α Tumor necrosis factor-alpha, IL-6 Interleukin-6, *IL-*1β Interleukin-1β, SMD Standardized mean difference, WMD Weighted mean difference, ⨁⨁⨁⨁ high certainty, ⨁⨁⨁◯ moderate certainty, ⨁⨁◯◯ low certainty, ⨁◯◯◯ very low certainty^−^downgrade, ^+^not downgrade, ^+^dp/dtmax, Maximum rate of left ventricular pressure rise; ^-^dp/dtmax, Maximum rate of left ventricular pressure decrease
Meta-analysis results
Effect of ginsenosides on myocardial infarction size
Measurement of myocardial infarction size (IS) was reported in 28 included studies [25–37, 41–55], involving 206 animals in the control group and 207 animals in the administration group. Because of significant heterogeneity in the determination of myocardial infarct size, the results were pooled and analyzed using a random-effects model (I^2^ = 70.00%, P < 0.00001). The results are shown in Fig. 3, where the use of ginsenosides significantly reduced the size of myocardial infarction (SMD = 3.09, 95% CI = 2.49–3.69, P < 0.00001). In addition, considering the significant heterogeneity in this analysis, we conducted a sensitivity analysis to investigate the reasons for this (Supplementary Fig. 1). After excluding each study individually, the total effect sizes and I^2^ values remained unchanged, indicating the robustness of our results.
Fig. 3. Forest plot of the effect of ginsenosides on the size of myocardial infarction
Effects of ginsenosides on post-MI cardiac function
In order to verify the beneficial effects of ginsenosides on cardiac function, we examined five cardiac function indexes: +dp/dtmax, -dp/dtmax, LVEF, LVSP, and LVEDP. The results of the heterogeneity test showed + dp/dtmax I^2^ = 77.00%, -dp/dtmax I^2^ = 57.00%, LVEF I^2^ = 69.00%, LVSP I^2^ = 69.00%, LVEDP I^2^ = 87.00%. Consequently, all outcome indicators were analyzed using a random-effects model in a pooled manner. In addition, sensitivity analyses of the five outcome indicators showed that our results were reliable and stable (Supplementary Fig. 2).
First, there are nine articles that reported the therapeutic effects of ginsenosides on + dp/dtmax and -dp/dtmax [23, 25, 31, 33, 37, 43, 44, 54, 56]. These articles included a total of 72 animals in the control group and 72 animals in the administration group, as depicted in Fig. 4A and B. The use of ginsenosides significantly reversed the decrease in control + dp/dtmax (SMD = 2.73, 95% CI = 1.69–3.77, P < 0.00001). Simultaneously, the decrease in -dp/dtmax was also reversed (SMD = 2.11, 95% CI = 1.42–2.80, P < 0.00001). Secondly, eight studies reported the effect of ginsenosides on LVEF [27, 29, 34, 50, 51, 53, 54, 56], with 54 animals in the control group and 54 animals in the administered group. The results are shown in Fig. 4C, where LVEF was significantly higher in the administered group compared to the control group (SMD = 3.11, 95% CI = 1.89–4.33, P < 0.00001). The effect on LVSP was then determined in seven studies involving 58 animals in the dosing group and 58 animals in the control group [23, 25, 33, 37, 43, 44, 56]. As shown in Fig. 5A, ginsenosides were able to cause a significant increase in LVSP (SMD = 2.63, 95% CI = 1.63–3.62, P < 0.00001). Finally, seven studies (57 animals each in control and administered groups) reported the effect of ginsenosides on LVEDP [25, 33, 37, 43, 44, 54, 56]. Treatment with ginsenosides significantly reduced LVEDP (SMD = 3.88, 95% CI = 2.10–5.66, P < 0.0001). Specific results are shown in Fig. 5B.
Fig. 4. Forest diagram of the effect of ginsenosides on cardiac function. A + dp/dtmax, B **-**dp/dtmax, C LVEF
Fig. 5. Forest diagram of the effect of ginsenosides on cardiac function. A LVSP, B LVEDP
Effect of ginsenosides on myocardial damage
Considering that the results of the heterogeneity test showed significant heterogeneity (LDH: I^2^ = 81.00%, CK-MB: I^2^ = 83.00%, CK: I^2^ = 89.00%), three markers of myocardial injury were evaluated using a random-effects model to explore the potential benefits of ginsenosides on myocardial injury. The results of the sensitivity analysis showed that the findings were robust for all three markers (Supplementary Fig. 3).
A pooled analysis of 19 animal studies (165 animals each in control and administered groups) showed that ginsenosides significantly down-regulated LDH secretion compared to controls (SMD = 3.05, 95% CI = 2.25–3.86, P < 0.00001, Fig. 6A) [23, 27, 30, 36–38, 41–44, 46–51, 53–55]. Not only that, ginsenosides also reduced serum levels of CK-MB [23, 27, 30, 36–38, 41, 42, 47, 48, 50, 51, 53] (n = 318, SMD = 3.09, 95% CI = 2.03–4.15, P < 0.00001, Fig. 6B) as well as CK [27, 30, 42–44, 46, 49, 54, 55] (n = 154, SMD = 6.32, 95% CI = 4.09–8.54, P < 0.00001, Fig. 6C).
Fig. 6. Forest plot of the effect of ginsenosides on markers associated with myocardial injury. A LDH, B CK-MB, C CK
Effects of ginsenosides on apoptosis and oxidative stress
The effect of ginsenosides on cardiomyocyte apoptosis was reported in six studies (31 animals each in control and administered groups) [28, 35, 37, 47, 51, 56]. The results of the pooled analysis are shown in Fig. 7A, where ginsenosides effectively resisted apoptosis in cardiomyocytes (SMD = 2.79, 95% CI = 1.33–4.26, P = 0.0002 < 0.001, heterogeneity: I^2^ = 57.00%). Sensitivity analysis showed this result to be stable (Supplementary Fig. 4).
Fig. 7. Forest plot of the effect of ginsenosides on indicators related to apoptosis and oxidative stress. A Cardiomyocyte apoptosis rate, B SOD, C MDA
To assess the effect of ginsenosides on oxidative stress, we analyzed the expression of SOD and MDA. Seventeen of these studies measured SOD [24, 26, 27, 30, 36–41, 44, 46, 48–50, 52, 55], and it was evident that there was a significant increase in the level of SOD in the treatment group (SMD = 2.30, 95% CI = 1.65–2.94, P < 0.00001, heterogeneity: I^2^ = 75.00%, Fig. 7B). Regarding the measurement of MDA, a pooled analysis of 15 studies [23, 24, 27, 30, 36–41, 48–50, 52, 55] showed that ginsenoside administration reduced MDA expression (SMD = 1.97, 95% CI = 1.24–2.70, P < 0.00001, heterogeneity: I^2^ = 77.00%, Fig. 7C).
Effect of ginsenosides on myocardial inflammation
Ginsenosides had good anti-inflammatory properties and effectively protected the myocardium from inflammatory responses. In this pooled analysis, we mainly observed the expression levels of three inflammatory factors: IL-1β, IL-6, and TNF-α. Due to the significant heterogeneity of IL-6 and TNF-α, analyses were performed using a random-effects model (IL-6: I^2^ = 81.00%, TNF-α: I^2^ = 90.00%). The heterogeneity of IL-1β metrics was not significant, so analyses were conducted using a fixed-effects model (IL-1β: I^2^ = 37.00%). Sensitivity analyses showed that all outcome indicators were stable (Supplementary Fig. 5).
In a pooled analysis of five studies [23, 26, 28, 50, 56] (40 animals per group), we observed a statistically significant reduction in IL-1β in the ginsenosides-treated versus control group (SMD = 2.63, 95% CI = 1.97–3.29, P < 0.00001, Fig. 8A). Additionally, the use of ginsenosides significantly reduced IL-6 [23, 36, 37, 40, 50] (SMD = 2.41, 95% CI = 1.09–3.73, P = 0.0003 < 0.01, Fig. 8B) and TNF-α [28, 32, 34, 36, 37, 45, 50, 56] (SMD = 4.43, 95% CI = 2.41–6.45, P < 0.0001, Fig. 8C).
Fig. 8. Forest plot of the effect of ginsenosides on myocardial inflammation-related indicators. A IL-1β, B IL-6, C TNF-α
Results of subgroup analysis
First, subgroup analyses were performed on predefined five outcome indicators according to the type of ginsenosides (Table 3A). Subgroup analyses of IS showed that ginsenoside Rb (SMD = 2.85, 95% CI = 2.11–3.58, P < 0.01), ginsenoside Rg (SMD = 3.43, 95% CI = 1.85–5.01, P < 0.01), ginsenoside Rh (SMD = 2.47, 95% CI = 0.97–3.96, P < 0.01), and Other (SMD = 5.73, 95% CI = 1.51–9.94, P < 0.01) subgroups still significantly reduced myocardial infarct size, and the heterogeneity remained significant (Ginsenoside Rb: I^2^ = 68.00%; Ginsenoside Rg: I^2^ = 68.00%; Ginsenoside Rh: I^2^ = 56.00%; Other: I^2^ = 88.00%). Subgroup analyses of LDH showed that only the ginsenoside Rb (SMD = 2.43, 95% CI = 1.50–3.36, P < 0.01, I^2^ = 81.00%) and Other (SMD = 4.70, 95% CI = 2.69–6.72, P < 0.01, I^2^ = 72.00%) subgroups were able to observe benefits, and the heterogeneity remained significant for both. Subgroup analysis of the three outcome indicators, CK-MB, SOD, and MDA, showed that the protective effect of ginsenosides persisted. However, in a subgroup analysis of MDA outcome metrics, we found that the protective effect of the ginsenoside Rg subgroup on MDA was no longer present (SMD = -0.27, 95% CI = -3.24–2.69, P = 0.857, I^2^ = 91.00%). Subgroup difference tests indicated that different ginsenosides did not produce significant differences in the outcome measures of IS (P = 0.48, I^2^ = 0.00%), LDH (P = 0.21, I^2^ = 34.50%), and SOD (P = 0.16, I^2^ = 45.4%).
Table 3. Subgroup analyses based on (A) ginsenoside class, (B) pretreatment, and (C) speciesSubgroupsOutcomes (A)Ginsenosides RbGinsenosides RgGinsenosides RhOtherSubgroupsDifferencesSMD95% CI P I^2^SMD95% CI P I^2^SMD95% CI P I^2^SMD95% CI P I^2^IS2.85[2.11, 3.58]< 0.0168%3.43[1.85, 5.01]< 0.0168%2.47[0.97, 3.96]< 0.0156%5.73[1.51, 9.94]< 0.0188%P = 0.48,I^2^ = 0.0%LDH2.43[1.50, 3.36]< 0.0181%5.83[−2.81, 14.47]0.18690%3.71[−1.55, 8.97]0.16785%4.70[2.69, 6.72]< 0.0172%P = 0.21,I^2^ = 34.5%CK-MB2.46[1.34, 3.58]< 0.0184%1.62[0.24, 3.00]0.022-9.89[4.19, 15.60]< 0.01-5.06[2.61, 7.51]< 0.0151%P = 0.007,I^2^ = 75.4%SOD1.87[1.21, 2.53]< 0.0164%3.20[1.97, 4.43]< 0.0139%2.64[0.55, 4.73]0.01389%----P = 0.16,I^2^ = 45.4%MDA1.92[1.24, 2.59]< 0.0164%−0.27[−3.24, 2.69]0.85791%4.78[3.03, 6.52]< 0.010%2.58[1.25, 3.91]< 0.01-P = 0.007,I^2^ = 75.0% Subgroups
Outcomes (B)
Pretreatment
No pretreatment
Subgroups
Differences
SMD
95% CI
P
I ^2^
SMD
95% CI
P
I ^2^ IS3.37[2.56, 4.17]< 0.0173%2.72[1.78, 3.66]< 0.0167%P = 0.3,I^2^ = 5.0%LDH4.69[3.26, 6.12]< 0.0185%1.49[0.93, 2.04]< 0.0140%P < 0.0001,I^2^ = 94.0%CK-MB5.65[2.94, 8.35]< 0.0187%2.04[1.09, 3.00]< 0.0174%P = 0.01,I^2^ = 83.5%SOD3.40[1.68, 5.11]< 0.0188%1.71[1.24, 2.18]< 0.0133%P = 0.06,I^2^ = 71.2%MDA3.89[2.12, 5.65]< 0.0178%1.38[0.64, 2.11]< 0.0172%P = 0.01,I^2^ = 85.0% Subgroups
Outcomes (C)
Rats
Mice
Duncan-Hartley guinea pigs
Subgroups
Differences
SMD
95% CI P and I^2^ SMD
95% CI P and I^2^ SMD (95% CI) P and I^2^IS3.01[2.40, 3.62]P < 0.01,I^2^ = 70.0%4.41[1.85, 6.97]P = 0.20,I^2^ = 39.0%--P = 0.30,I^2^ = 7.60%LDH3.07[2.23, 3.91]P < 0.01,I^2^ = 82.0%---3.08 [1.61, 4.55]P < 0.01P = 0.99,I^2^ = 0.0%CK-MB2.79[1.76, 3.83]P < 0.01,I^2^ = 82.0%---6.01 [3.61, 8.42]P < 0.01P = 0.02,I^2^ = 82.8%MDA1.92[1.15, 2.70]P < 0.01,I^2^ = 78.0%---2.58 [1.25, 3.91]P < 0.01P = 0.40,I^2^ = 0.0%IS Infarct size, LDH Lactate dehydrogenase, CK-MB Creatine kinase MB, SOD Superoxide dismutase, MDA Malondialdehyde
Secondly, to thoroughly investigate the preventive and therapeutic effects of ginsenosides on MIRI, we conducted subgroup analyses based on whether ginsenosides were administered as pretreatment or not (Table 3B). Pretreatment subgroup analyses showed that ginsenosides were beneficial for all five outcome measures: IS (SMD = 3.37, 95% CI = 2.56–4.17, P < 0.01, I^2^ = 73.00%), LDH (SMD = 4.69, 95% CI = 3.26–6.12, P < 0.01, I^2^ = 85.00%), CK-MB (SMD = 5.65, 95% CI = 2.94–8.35, P < 0.01, I^2^ = 87.00%), SOD (SMD = 3.40, 95% CI = 1.68–5.11, P < 0.01, I^2^ = 88.00%), and MDA (SMD = 3.89, 95% CI = 2.12–5.65, P < 0.01, I^2^ = 78.00%), and the heterogeneity was significant for all of them. Not only that, the protective effect of ginsenosides persisted in the subgroup without pretreatment. It should be noted that the heterogeneity of the protective effect of ginsenosides on LDH and SOD was not significant in this subgroup (LDH: I^2^ = 40.00%, SOD: I^2^ = 33.00%). Overall, differences among subgroups were observed regarding the interventions [LDH: (P < 0.05, I^2^ = 94.00%); CK-MB (P = 0.01, I^2^ = 83.50%); SOD (P = 0.06, I^2^ = 71.20%); MDA: (P = 0.01, I^2^ = 85.50%)].
Finally, we conducted subgroup analyses based on species (Table 3C). The results showed that in rats, ginsenosides had statistically significant effects favoring the intervention on IS (SMD = 3.01, 95% CI = 2.40–3.62, P < 0.01, I^2^ = 70.00%), LDH (SMD = 3.07, 95% CI = 2.23–3.91, P < 0.01, I^2^ = 82.00%), CK-MB (SMD = 2.79, 95% CI = 1.76–3.83, P < 0.01, I^2^ = 82.00%), and MDA (SMD = 1.92, 95% CI = 1.15–2.70, P < 0.01, I^2^ = 78.00%), although all exhibited considerable heterogeneity. In mice, no significant therapeutic effect of ginsenosides on alleviating IS was observed, with low heterogeneity (SMD = 4.41, 95% CI = 1.85–6.97, P > 0.05, I^2^ = 39.00%). However, due to insufficient data, the effects of ginsenosides on LDH, CK-MB, and MDA in mice and Duncan-Hartley guinea pigs remain unclear.
Meta-regression analysis
To fully investigate sources of heterogeneity, a meta-regression analysis was conducted for difficult-to-cluster confounding factors, including anesthetic type, time of administration, mode of administration, duration of ischemia, and duration of reperfusion. The results are shown in Table 4. We found that these confounding factors were not sources of heterogeneity for the outcome measures IS, LDH, SOD, and MDA. However, time of administration (P = 0.009 < 0.05) and duration of ischemia (P = 0.006 < 0.05) were identified as sources of heterogeneity for the CK-MB outcome measure.
Table 4. Meta-regression analysis was performed with anesthetic type, time of administration, mode of administration, duration of ischemia, and duration of reperfusion as covariatesOutcomesHeterogeneity FactorCoefficientStd. ErrtP Value95% CIISAnesthetic type−0.21097640.1713932−1.230.231[−0.5664241, 0.1444713]Time of administration0.11953270.09185081.300.207[−0.0709542, 0.3100195]Mode of administration−0.10700750.2231552−0.480.636[−0.569803, 0.355788]Duration of ischemia−0.72158260.8845747−0.820.423[−2.556078, 1.112913]Duration of reperfusion−0.25788010.2436062−1.060.301[−0.7630884, 0.2473281]LDHAnesthetic type−0.76803020.3758261−2.040.062[−1.579953, 0.0438927]Time of administration−0.03035370.1772381−0.170.867[−0.4132534, 0.3525461]Mode of administration0.84557310.54840271.540.147[−0.3391789, 2.030325]Duration of ischemia−0.54469951.383987−0.390.700[−3.534621, 2.445223]Duration of reperfusion1.2172080.65653021.850.087[−0.2011388, 2.635556]CK-MBAnesthetic type0.06926590.31936020.220.834[−0.6859009, 0.8244328]Time of administration−0.9249080.2594603−3.560.009[−1.538434,−0.3113818]Mode of administration−0.63621630.5458382−1.170.282[−1.926918, 0.6544858]Duration of ischemia4.9323971.284563.840.006[1.894895, 7.969899]Duration of reperfusion0.49962080.7929620.630.549[−1.375436, 2.374678]SODAnesthetic type−0.39872540.3005316−1.330.211[−1.060191, 0.2627401]Time of administration0.08030980.16728120.480.641[−0.2878735, 0.4484932]Mode of administration0.25704020.37591140.680.508[−0.5703352, 1.084416]Duration of ischemia−0.9923192.538071−0.390.703[−6.578575, 4.593937]Duration of reperfusion0.22719040.40585350.560.587[−0.6660872, 1.120468]MDAAnesthetic type−0.80618380.3921053−2.060.070[−1.693188, 0.0808199]Time of administration0.05923370.31435350.190.855[−0.6518834, 0.7703507]Mode of administration1.0383190.53696171.930.085[−0.176373, 2.25301]Duration of ischemia−1.48921.652382−0.900.391[−5.227148, 2.248749]Duration of reperfusion0.50465420.50988850.990.348[−0.6487937, 1.658102]IS Infarct size, LDH Lactate dehydrogenase, CK-MB Creatine kinase MB, SOD Superoxide dismutase, MDA Malondialdehyde
Detection of publication bias
By utilizing a funnel plot and Egger’s test, we identified significant publication bias in thirteen outcome metrics: IS (Egger’s: t = 7.06, P < 0.05), +dp/dtmax (Egger’s: t = 6.26, P < 0.05), -dp/dtmax (Egger’s: t = 6.34, P < 0.05), LVEF (Egger’s: t = 3.09, P < 0.05), LVSP (Egger’s: t = 8.76, P < 0.05), LVEDP (Egger’s: t = 15.44, P < 0.05), LDH (Egger’s: t = 9.27, P < 0.05), CK-MB (Egger’s: t = 6.32, P < 0.05), CK (Egger’s: t = 7.49, P < 0.05), SOD (Egger’s: t = 11.26, P < 0.05), apoptotic rate (Egger’s: t = 6.72, P < 0.05), TNF-α (Egger’s: t = 4.88, P < 0.05), and IL-6 (Egger’s: t = 26.12, P < 0.05). There was no significant publication bias detected for the remaining two indicator outcome metrics, as detailed in Supplementary File 1.
We employed the trim-and-fill method to analyze 13 outcome measures with publication bias. These measures included: IS (Heterogeneity: Q = 131.887, P < 0.01, SMD = 12.12, 95% CI = 6.43–22.84), +dp/dtmax (Heterogeneity: Q = 35.042, P < 0.01, SMD = 15.35, 95% CI = 5.41–43.52), -dp/dtmax (Heterogeneity: Q = 25.895, P = 0.004 < 0.01, SMD = 6.18, 95% CI = 3.09–12.35), LVEF (Heterogeneity: Q = 31.230, P = 0.001 < 0.01, SMD = 11.36, 95% CI = 3.50–36.86), LVSP (Heterogeneity: Q = 31.230, P = 0.001 < 0.01, SMD = 11.36, 95% CI = 3.50–36.86), LVEDP (Heterogeneity: Q = 67.817, P < 0.01, SMD = 12.69, 95% CI = 1.96–82.41), LDH (Heterogeneity: Q = 170.743, P < 0.01, SMD = 6.48, 95% CI = 2.63–15.95), CK-MB (Heterogeneity: Q = 73.086, P < 0.01, SMD = 20.75, 95% CI = 7.15–60.22), CK (Heterogeneity: Q = 88.185, P < 0.01, SMD = 89.39, 95% CI = 11.77–678.70), SOD (Heterogeneity: Q = 96.745, P < 0.01, SMD = 5.45, 95% CI = 2.79–10.63), apoptotic rate (Heterogeneity: Q = 19.714, P < 0.01, SMD = 6.47, 95% CI = 1.52–27.51), TNF-α (Heterogeneity: Q = 73.084, P < 0.01, SMD = 84.00, 95% CI = 11.10–635.77), and IL-6 (Heterogeneity: Q = 21.386, P < 0.01, SMD = 11.12, 95% CI = 2.97–41.55). Even after accounting for potentially missing studies, the results remained statistically significant, indicating that the significance of our findings is not attributable to publication bias. Detailed trim-and-fill results are provided in Supplementary File 1.
Discussion
Summary of evidence
This paper has synthesized and analyzed 34 studies that included a total of 505 animals. Compared with the control group, ginsenosides significantly reduced infarct size, inhibited the elevation of LVEDP, and attenuated the decreases in LVSP, +dp/dtmax, and –dp/dtmax. These findings collectively demonstrate that ginsenosides exert robust cardioprotection. In addition, ginsenosides inhibited the increases in serum levels of LDH, CK-MB, CK, MDA, TNF-α, IL-6, and IL-1β, as well as cardiomyocyte apoptosis after MIRI. Despite significant publication bias in most outcome measures, sensitivity analyses and trim-and-fill analyses indicated that our findings were robust and that the conclusions were reliable. The presence of publication bias is attributable to substantial underreporting of negative outcomes, because nearly all included studies reported positive results, which exaggerated the protective effects of ginsenosides. Additionally, almost half of the included studies had sample sizes of fewer than eight animals per group. Subgroup analyses indicated that ginsenosides demonstrated consistent therapeutic effects across animal species, ginsenoside subtypes, and routes of administration. Based on our analysis of existing literature, the promising therapeutic potential demonstrated by ginsenosides in treating MIRI cannot be overlooked.
Mechanistic exploration
MIRI, a frequent complication of reperfusion therapy for IHD, remains an unresolved priority in cardiology. It is driven by multiple molecular mechanisms, including inflammation, oxidative stress, calcium overload, impaired energy metabolism, apoptosis, autophagy, and mitochondrial dysfunction [57, 58]. Our findings indicate that ginsenosides inhibit free radical production and inflammatory responses, reduce the size of myocardial infarction, and improve blood flow, thereby mitigating myocardial injury following reperfusion. These results are consistent with those reported by Zhu et al. [59]. In fact, the anti-MIRI benefits of ginsenosides were previously suggested. In vitro studies by Dong et al. demonstrated that ginsenosides maintained the dynamic balance of mitochondria by regulating mitofusin 2 and glutamate dehydrogenase, thereby effectively preventing hypoxia/reoxygenation-induced damage to cardiomyocytes [60]. At an earlier time, Sun and colleagues found that pretreatment with ginsenosides increased the viability of rat cardiomyocytes, reduced LDH release, caspase-3 activity, and apoptosis, and that this protective effect was closely related to the AKT/MAPK signaling pathway [61]. All aforementioned evidence indicates that ginsenosides are potential anti-MIRI agents, and our results confirm this.
With advances in medical research, the anti-MIRI effects of ginsenosides have garnered increasing attention. The MIRI process entails dysfunction of cation pumps, calcium overload, and excessive reactive oxygen species, which impair energy metabolism and up-regulate autophagy [62, 63]. Research has shown that ginsenosides inhibit the opening of the mitochondrial permeability transition pore, restore mitochondrial membrane potential, and upregulate phosphorylated protein kinase B and phosphorylated glycogen synthase kinase-3β, thereby correcting energy metabolism disorders in cardiomyocytes [64]. Ginsenosides also regulate the expression of proteins in the tricarboxylic acid cycle, including the L-lactate dehydrogenase B chain, the pyruvate dehydrogenase complex, and the aldose reductase, thereby enhancing energy metabolism in ischemic rat hearts [65]. In addition, ginsenosides activate an autophagy-mediated survival response that prevents cardiomyocyte apoptosis. Beclin 1 and Bcl-2, key regulators of autophagy, initiate autophagy during starvation; however, ginsenosides weaken their interaction in H9c2 cells under starvation, thereby reducing autophagy and preventing apoptosis [66]. Besides these two pathways, ginsenosides enhance adenosine triphosphatase activity in cardiomyocytes and regulate cytoplasmic–endoplasmic-reticulum ion homeostasis, thereby attenuating myocardial damage induced by calcium overload [67]. In summary, primary pharmacologically active constituents of ginseng, ginsenosides exhibit significant therapeutic potential.
Strengths and prospects
Ginseng has been extensively studied as a potential treatment for MIRI because of its multi-component, multi-pathway, and multi-target mode of action [68]. Studies have demonstrated that ginsenosides, the principal bioactive constituents of ginseng, directly interact with diverse immune cells and thereby confer therapeutic effects against MIRI. Furthermore, ginsenosides exhibit high bioactivity, are rapidly absorbed and utilized, and cause minimal adverse effects [69, 70]. The anti-MIRI properties of ginsenosides were clearly evident from our subgroup analysis. However, certain subgroups were represented by only a single study, which limits their informative value. More importantly, we found that administering ginsenosides before ischemia-reperfusion was more protective than administering them after. Additionally, when comparing different ginsenoside components, ginsenoside Rg exhibited superior efficacy in reducing LDH levels, whereas ginsenoside Rh provided better cost-effectiveness in lowering CK-MB levels. The core findings of this study support previous research indicating that ginsenosides exhibit promising therapeutic potential for MIRI [37, 71]. This consistency across studies and periods underscores the maturity of the field. Our contribution lies in enlarging the sample size with additional studies, thereby improving the precision of effect estimates. Additionally, we applied the GRADE framework to grade confidence in our conclusions and to transparently acknowledge the suboptimal quality of evidence for some outcomes.
Translational implications
In the modern drug development process, systematic reviews and meta-analyses of animal studies represent a crucial step toward translating preclinical data into clinical applications. The literature included herein is highly consistent with clinical MIRI cases, both in terms of disease model construction and the simulation of pathophysiological processes. Nevertheless, animal models inherently differ from human pathophysiology; therefore, verifying the efficacy of ginsenosides solely in animal models is insufficient. Phase I clinical trials are warranted to assess their safety profiles and validate our findings. Moreover, the current understanding of the mechanisms underlying ginsenoside action focuses primarily on anti-inflammatory, anti-apoptotic, and antioxidative stress effects, whereas calcium overload, energy metabolism disorders, ferroptosis, and autophagy remain understudied. We therefore recommend that future research prioritize these underinvestigated pathways as potential therapeutic targets.
Limitations
This study is based on extensive preclinical evidence that illustrates the significant effects of ginsenosides against MIRI, and confirms their efficacy. Nevertheless, several limitations of the present work should be recognized. First, most included studies exhibited low or unclear methodological quality, with inadequate reporting of blinding and risk of bias; consequently, some indicators received low-quality ratings that may weaken the persuasiveness of our conclusions. Second, substantial heterogeneity affected most outcome indicators; despite our efforts to identify its sources, limited literature precluded comprehensive analysis for some outcomes. Third, most corresponding authors are affiliated with Chinese institutions, and this geographical concentration may increase heterogeneity. Finally, the use of SMD and pooling across different doses may obscure dose–response relationships; thus, caution is warranted when interpreting these results. Additionally, MIRI patients often present with comorbidities such as hypertension and diabetes; however, this factor was rarely accounted for in the included studies. Therefore, future research should develop models that incorporate these pathological characteristics to evaluate whether ginsenoside-based combination therapy enhances cardioprotective efficacy.
Conclusion
This study systematically evaluated the preventive and therapeutic effects of ginsenosides against MIRI. Preliminary findings indicate that ginsenosides reduce myocardial infarct size and improve cardiac function. Moreover, ginsenosides exhibit potent anti-inflammatory, anti-apoptotic, and antioxidant properties. Despite its limitations, the outlook for ginsenosides as therapeutic agents against MIRI remains promising. Thus, ginsenosides may offer novel preventive and therapeutic strategies for patients with MIRI, warranting further investigation and development.
Supplementary Information
Supplementary Material 1. Supplementary Figure 1: Sensitivity analysis of myocardial infarction size.
Supplementary Material 2. Supplementary Figure 2: Sensitivity analysis of the effect of ginsenosides on cardiac function. (A) +dp/dtmax, (B) -dp/dtmax, (C) LVEF, (D) LVSP, (E) LVEDP.
Supplementary Material 3. Supplementary Figure 3: Sensitivity analysis of the effect of ginsenosides on myocardial injury. (A) LDH, (B) CK-MB, (C) CK.
Supplementary Material 4. Supplementary Figure 4: Sensitivity analysis of ginsenosides on the effects of apoptosis and oxidative stress. (A) Apoptosis rate, (B) SOD, (C) MDA.
Supplementary Material 5. Supplementary Figure 5: Sensitivity analysis of the effect of ginsenosides on myocardial inflammation. (A) IL-1β, (B) IL-6, (C) TNF-α.
Supplementary Material 6. Supplementary File 1: Results of funnel plots, Egger’s test, and trim-and-fill analyses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu Z, Cecarini V, Cuccioloni M, Bonfili L, Gong C, Angeletti M, Eleuteri AM. Ginsenosides Rg 1 and Rg 2 activate autophagy and attenuate oxidative stress in neuroblastoma cells overexpressing Aβ(1–42). Antioxid (Basel). 2024;13(3):310. 10.3390/antiox 13030310 PMC 1096760438539843 · doi ↗ · pubmed ↗