Adolescent-Parent Dyad and Adolescent Eating Disorders: A Standardized Patient Simulation
Connie Gao, Carolyne Plansky, Nicole Ferguson, Jennifer Caputo-Seidler, Amy Weiss, Vinita Kiluk

TL;DR
This study introduces a simulation to help medical students practice communicating with adolescents and their parents about sensitive health issues.
Contribution
A new OSCE using a standardized patient dyad to train medical students in adolescent communication and differential diagnosis.
Findings
Students identified an average of 2.24 correct differentials during the OSCE.
Standardized patient feedback showed students met or exceeded expectations in most communication domains.
Students improved their skills in taking histories, performing exams, and maintaining confidentiality with adolescents.
Abstract
Introduction: Many medical students are uncomfortable with adolescent patients and the associated difficulties of navigating speaking with an adolescent alone while ensuring confidentiality. To address this, students are encouraged to effectively use the home, education and employment, eating, activities, drugs, sexuality, suicide/depression, and safety (HEEADSSS) assessment, which is a history-taking method designed to reveal information about a patient’s home life, social life, and self-image. We created this observed structured clinical examination (OSCE) for learners to practice their communication skills and improve their comfort in seeing adolescents. In this case, learners interviewed an adolescent female with an overbearing mother, which adds yet another level of difficulty. Medical students practised history and physical exam skills as well as developed a differential diagnosis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
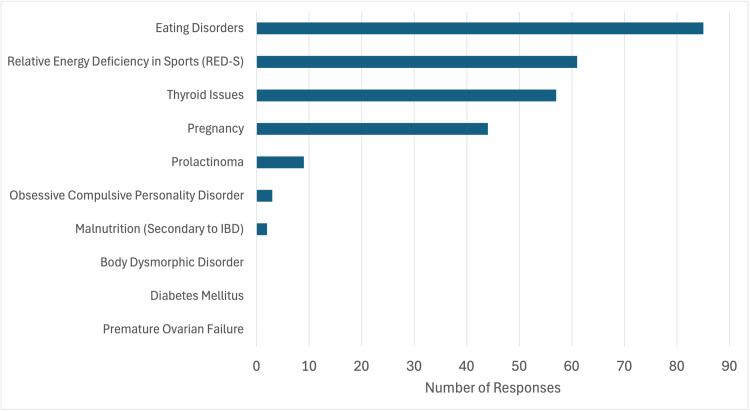 Figure 1
Figure 1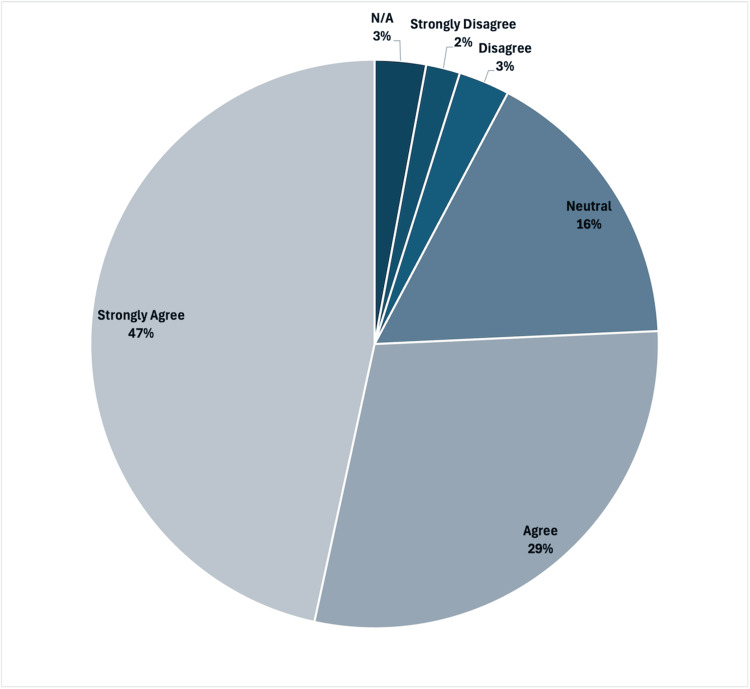 Figure 2
Figure 2| Differential | Acceptable Alternative | Not Accepted |
| Anorexia nervosa | Bulimia, Other not specified eating disorder | Avoidant/restrictive food intake disorder (ARFID) |
| Relative energy deficiency in sport (RED-S) | Athletic triad, female athlete triad, stress-induced amenorrhea, functional hypothalamic amenorrhea | Hormonal imbalance, hypogonadotropic hypogonadism, hypopituitarism, and adrenal insufficiency |
| Malnutrition secondary to Inflammatory Bowel Disease (IBD) | Malnutrition secondary to (other medical condition) | Malnutrition secondary to poor caloric intake (student must give medical cause), Iron-deficient anemia, Vague "nutritional deficiency" or "insufficient caloric intake" |
| Obsessive-compulsive personality disorder | Obsessive-compulsive disorder (OCD) | Depression, adjustment disorder |
| Pregnancy | - | - |
| Premature ovarian failure | - | Polycystic ovary syndrome (PCOS), primary amenorrhea, anovulatory cycles |
| Diabetes mellitus | - | - |
| Thyroidopathy | Hyperthyroidism, hypothyroidism | - |
| Body dysmorphic disorder | - | - |
| Hyperprolactinemia | Prolactinoma, pituitary adenoma | - |
| Score | Partnership | Empathy | Apology | Respect | Legitimization | Support |
| Above expectations | 50% | 47% | 39% | 49% | 51% | 52% |
| Meets expectations | 42% | 39% | 24% | 45% | 41% | 31% |
| Standardized Patient Feedback Prompt: “As a patient, these students made me feel” | ||
| Positive themes | Number of Students | Example Statement |
| Comfortability | 70 (59.3%) | "As a patient, the student made me feel very comforted and heard" |
| Listened to | 32 (27.1%) | "I felt partnered with the student to figure out what is going on. " |
| Cared for | 21 (17.8%) | "As patients, “J” made us feel important. He was incredibly warm and engaging." |
| Feeling partnered/included in conversation | 17 (14.4%) | "I felt truly respected, supported, and partnered at the highest level." |
| Negative themes | Number of students | Example Statement |
| Lack of rapport | 5 (4.2%) | "The student made us feel uncomfortable since he didn't establish rapport before asking awkward questions." |
| Overwhelmed | 3 (2.5%) | "As a patient, the student made me feel like he overwhelmed us with a lot of information." |
| Judged | 3 (2.5%) | "As a patient, this student made me feel overall supported but a little judged." |
| Standardize Patient Feedback Prompt: “Please state what the students could improve on for next time.” | |
| Response from SP | Number of students receiving feedback |
| Building rapport with patient before asking sensitive questions | 10 (8.5%) |
| Navigating timing and how to ask the mother to leave | 10 (8.5%) |
| Decreasing medical jargon use | 5 (4.2%) |
| Confidence/knowing next steps | 4 (4.2%) |
| Standardize Patient Feedback Prompt: “Please state what the students did well.” | |
| Response from SP | Number of students recieving feedback |
| Making the patient feel comfortable | 20 (16.9%) |
| Clear communication/clear explanations | 20 (16.9%) |
| Feeling heard/listened to | 15 (12.7%) |
| Asked the mom to leave well | 10 (8.5%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · Innovations in Medical Education · Empathy and Medical Education
Introduction
Medical students may find encounters with adolescent patients to be difficult for a variety of reasons. Balancing speaking privately with a teenager while maintaining confidentiality can be challenging, and questions regarding risk-taking behaviors, such as substance use or sexual activity, may be embarrassing for learners to ask. However, due to high rates of morbidity and mortality from risk-taking behaviors and unintentional injuries in adolescents, a comprehensive psychosocial interview is essential. Adolescents who report receiving patient-centered care are more likely to have participated in private conversations with a clinician as well as discussions regarding health behaviors. These same adolescents are less likely to report an unmet need for care or having a serious, untreated health problem [1].
The observed structured clinical examination (OSCE) presented here was created to primarily increase learners’ exposure to challenging adolescent patients and their parents, and to improve comfort level in having difficult conversations with this patient population. Recent studies have shown that medical students are reporting feeling underprepared for their pediatrics clerkships, therefore making OSCEs, such as the one presented in this paper, are more relevant than ever [2]. As pediatric clerkships have decreased in length over the past decade, there is no guarantee that students will develop the skills necessary to approach an overbearing parent and their ambivalent teenager [3]. Adolescent SPs have been shown to improve students’ skills of working with adolescent patients and to help students bridge their own past experiences of adolescence with their new role in a physician-patient interaction. Each additional practice with adolescent patients helps students fine-tune their professionalism in this complicated setting [4]. The OSCE format was chosen to decrease didactic time and increase student experiential learning.
Understanding how to properly utilize the home, education and employment, eating, activities, drugs, sexuality, suicide/depression, and safety (HEEADSSS) assessment is an important skill for a physician to have, as is recommended by the American Academy of Pediatrics [5]. HEEADSSS is designed as a thorough yet succinct history, taking method that elucidates information about a patient’s home life, social life, and self-image [6]. Students were taught to use HEEADSSS as a tool to structure their interview given the discomfort many students have with adolescent patient interviews. It is designed to gradually increase the invasiveness of each question asked to avoid overwhelming the adolescent patient. This helps the physician develop rapport with both the patient and the patient’s parent over the course of the interview [6]. Learners have also been taught about the need to speak with adolescent patients privately, the need for and importance of confidentiality, and the limits of confidentiality.
Furthermore, this OSCE focuses on developing diagnostic reasoning skills and obtaining a thorough history. It is particularly important that medical trainees gain experience in guiding conversations regarding adolescent mental health and eating behaviors. Physicians in primary care are in the position to detect eating disorders early and prevent worsening complications of the disease [7]. There has been a dramatic increase in the incidence of eating disorders following the coronavirus disease 2019 pandemic, primarily in female adolescents with diagnoses of anorexia nervosa. With such a staggering rise in hospital admissions for self-harm and eating disorders, early detection by physicians is more important than ever [8,9]. This case highlights several red flags, as well as more subtle signs, that can guide clinicians to consider further work-up for an eating disorder. At the same time, the patient presentation is purposefully ambiguous enough that students are required to develop a broad differential for amenorrhea in adolescents. Not only is it important for students to correctly identify the root of a patient’s problem, but it is equally important for learners to keep an open mind and avoid confirmation bias when conducting the rest of their history and exam. In this OSCE, students were asked to provide three potential differential diagnoses for the patient’s presentation, rather than focusing on one correct differential diagnosis. This serves as a measurable goal and encourages students to consider less readily obvious causes of amenorrhea and expand their diagnostic skills.
Materials and methods
Educational context
This OSCE was first implemented in 2012. The simulation was created to ensure standardization and to guarantee that all students were exposed to a difficult adolescent patient scenario. We chose to use the OSCE format as an experiential form of learning for the students, which allows educators to assess students’ higher-level skills in communication with adolescent patients and management of this difficult clinical scenario. This format also allows the student to demonstrate the application and analysis levels of Bloom’s Taxonomy while entering into the beginning stages of evaluation for the students who were able to successfully discuss a management plan with this patient and mother.
Setting and participants
The simulation is generally run four times per year, with about one-fourth of the third-year medical school class participating each time. All third-year medical students at a large academic institution participated. Each time we run this OSCE, we use four rooms concurrently in our medical education simulation center, which are designed to imitate a clinic setting. Prior to the OSCE, students were educated on the HEEADSSS framework and were encouraged to follow its structure (Appendix A). Each adolescent SP has a large water bottle or Styrofoam cup in the room. No other props are needed.
SPs selected for the adolescent patient in this case are typically in their early 20s but dressed to appear like high school students. SPs are asked to wear athletic clothing with baggy clothes overlaying (sweatshirt). We ask the SP mothers to dress well and appear like a middle-aged mother from an upper-middle-class family. Standardized patients and preceptors are emailed the standardized patient script (Appendix B) and the key teaching points (Appendix C) the week prior to the OSCE in order to review the material. All of our SPs receive general training on communication skills and providing feedback prior to working at our simulation center. On the day of the OSCE, the SPs receive training on this specific case. For example, the SPs playing the mother are asked to push back against the students’ request for them to leave the examination room unless rapport is achieved or if their questions from the learner are answered in an understandable manner.
Case procedure
At the start of the OSCE, students are given a door note (Appendix D) stating the chief complaint of amenorrhea and a set of vital signs. The door note includes instructions for the student to take on the role of the primary care doctor seeing the patient. The student is assigned to take a history related to the patient’s chief complaint. The student is asked to provide their top three differential diagnoses before leaving the room, along with an initial treatment plan. Students are given 25 minutes to conduct their patient interview and receive a five-minute warning prior to the end of the interview.
Learner assessment
After the OSCE, faculty preceptors and SPs are then asked to fill out written feedback forms (Appendix E) [10]. Students are asked to write-up the case with inclusion of patient history, assessment consisting of three differential diagnoses, and management plan. Students are asked to allow themselves 10 minutes for a write-up, timing themselves, and then must electronically submit the write-up within one week of the OSCE. These write-ups are reviewed by faculty or fourth-year medical students with formative feedback provided electronically. At the end of the year, students rated the case based on how they felt it helped advance their abilities to communicate with patients.
Data sources and measures
Analysis included all third-year medical students’ write-ups and SP data from the 2023-2024 academic year. The sample size was determined by the number of third-year medical students in the cohort during the 2023-2024 academic year; all eligible students were included.
Faculty defined a priori the set of acceptable differential diagnoses and alternatives (Table 1). Student write-ups were screened, and the presence of acceptable differentials was recorded for analysis. A maximum of one eating disorder and one thyroid disorder diagnosis was accepted. Differential diagnoses of malnutrition or insufficient caloric intake were considered invalid if the student failed to provide an identified cause. Other differential diagnoses were excluded due to a lack of consistency with the patient’s history and exam. These include child neglect, depression, ovarian cancer, avoidant restrictive food intake disorder, primary anovulation, hypomania, anemia, human immunodeficiency virus (HIV), adrenal insufficiency, and polycystic ovarian syndrome. Quantitative analysis was descriptive. To gauge students’ understanding of the OSCE, the average number and standard deviation of acceptable differentials were obtained. Students’ end-of-year evaluation responses for the OSCE were reported.
SP feedback responses were summarized and used to gauge overall student feedback. SPs rated each student on six domains: partnership, empathy, apology, respect, legitimization, and time management. We summarized the class performance, reporting the proportion of medical students who met or exceeded the SP’s expectation. SP short-answer responses were categorized into common themes (broadly positive or negative, then further into students’ ability to create comfort or a judgmental environment). The frequency of themes was quantified.
Results
Since this OSCE was first implemented in 2012, about 1,560 third-year medical students have completed this OSCE at our institution. During the 2023-2024 academic year, 118 third-year medical students participated in the case and submitted write-ups available for our review. All third-year medical students' write-ups were included in our analysis. In examining the differential diagnosis of 118 write-ups, one (0.8%) write-up included 0 valid differential diagnoses, 16 (13.6%) write-ups included only one valid differential diagnosis, 55 (46.6%) write-ups included two valid differential diagnoses, and 46 (39.0%) write-ups included three valid differential diagnoses.
Students are instructed to include three differential diagnoses within their case write-ups, and 110 (93.2%) of 118 submissions met this goal. However, of the 340 differentials given, only 264 (77.6%) met the study's a priori criteria for a valid differential. On average, students identified 2.24 correct differentials with a standard deviation of 0.71 differentials. As shown in Table 1, we excluded differential diagnoses that were redundant, nonspecific, or inappropriate for this patient scenario.
In examining the 264 valid differential diagnoses (shown graphically in Figure 1): 85 (72.0%) students identified eating disorders, 61 (51.6%) students identified relative energy deficiency in sports, 57 (48.3%) students identified thyroid disease, 44 (37.3%) students identified pregnancy, 9 (7.6%) students identified prolactinoma, 3 (2.5%) student identified obsessive compulsive personality disorder, 2 (1.7%) students identified malnutrition secondary to inflammatory bowel disease, 0 (0.0%) students identified body dysmorphic disorder, and 0 (0.0%) student identified premature ovarian failure.
Number of students that identified particular diagnoses. Compares acceptable differentials and the number of times students proposed the differential after their interaction with the SPs.
The remainder of our educational objectives cannot be objectively measured but instead are discerned from feedback forms from the SP’s and students. On feedback forms, SPs rated students on their abilities to project partnership, empathy, apology, respect, legitimization, and support during the OSCE (Appendix E) [10]. Students met or were above expectations 92% (N=108) of the time in partnership, 86% (N=101) of the time for empathy, 84% (N=99) of the time for apology, 93% (N=109) of the time for respect, 92% (N=108) of the time for legitimization, and 83% (N=97)of the time for support (Table 2).
The SPs then gave feedback detailing how students made them feel, how they could improve next time, and what the students did well (Appendix E). Themes in the SPs' feedback were identified and shown below (Table 3).
SPs noted that students made them feel comfortable, listened to, cared for, and partnered with. In the feedback, the most prominent themes critiquing the students involved a lack of rapport before asking sensitive questions, feeling overwhelmed, or feeling judged by the students. When asked for suggested improvements for students (Table 4), SPs noted building rapport, navigating timing when asking the mother to leave, decreasing medical jargon, and building confidence.
When asking for feedback on what the student did well (Table 5), SPs stated the students frequently made them feel comfortable, had clear communication, made them feel heard, and would ask the mom to leave well.
Additionally, preceptors reviewed what eating disorder red flags the students picked up in their interviews. SPs and preceptors discussed the students’ ability to successfully ask the mother to leave the room and discuss confidentiality, with a focus on the students’ ability to develop a rapport with the adolescent and earn the mother’s trust. Often, students who were not able to build a relationship with the SPs were not successful in getting the mother to leave the room. Preceptors also assessed the student’s plan for patient follow-up and evaluated the student’s use of the HEEADSSS assessment.
Several faculty members have acted as preceptors for this OSCE at our institution over the last few years. Typical faculty preceptors used for this case specialized in pediatrics, adolescent medicine, internal medicine-paediatrics, or family medicine. Faculty comments about the case are generally positive. Our faculty have enjoyed precepting this case, citing the realistic nature of the scenario and the opportunity for student education and growth. Concerns cited by faculty include the short amount of time given to the students and the fact that many students become fixated on getting mom out of the room, thereby wasting valuable interview time.
A cadre of younger women SPs (for the adolescent patient) and older women SPs (for the mom) have participated in this OSCE over the past few years. Many SPs comment that it is one of their favourite cases to play.
At the end of the year, students were given a course feedback form that gauged their feedback regarding the doctoring class. Particularly, 100 students responded to the prompt “the adolescent suicide case and eating disorder cases improved my comfort level and ability to communicate with adolescent patients and their parents." Of the 100 students responding (shown in Figure 2), 47 strongly agreed, 29 agreed, 16 were neutral, 3 disagreed, 2 strongly disagreed, and 3 stated not applicable.
Student response to "The adolescent suicide case and eating disorders cases improved my comfort level and ability to communicate with adolescent patients and their parents."
Discussion
We have found that this OSCE has provided an opportunity to increase exposure to adolescent patients, specifically a difficult adolescent scenario with an overbearing parent. There are many ways in which this case allows students to hone their communication skills. The learner must navigate seeking information from a reticent adolescent when her overbearing mom keeps answering questions. Many students struggle with the issue of asking their mom to leave the room to speak to the adolescent patient privately. Some students become fixated on getting mom out of the room to the detriment of their overall performance. They forget about the broader goals of rapport building and information gathering as they instead spend time arguing with mom. Some students are blatantly rude to the mother, while others discount her. Other students ignore the adolescent patient or aren’t able to build rapport with her since the mom is so overbearing.
The amount of time given for the interview is also a challenge for students. Many students would benefit from more time to talk to the adolescent and build rapport. However, due to the desire to keep the case realistic as would occur in a time-crunched clinic and also time limitations within our simulation center, we have decided to keep the time limited to 25 minutes [11, 12]. The students were given the HEEADSSS assessment to help mitigate the time constraints and provide structure for forming rapport with both the parent and adolescent. The HEEADSSS report provided students with an organized approach to efficiently gather social information, minimizing stress and maximizing the information they collected.
Despite the challenge, most students appreciated the opportunity to participate in this OSCE, with 76% (N=76) of the students agreeing or strongly agreeing that the OSCE helped them gain skills when communicating with adolescent patients and their family members on their end-of-year feedback forms. However, the students' responses to both an adolescent suicide OSCE and the eating disorder OSCE discussed in this paper were gauged in a single prompt in the feedback form; therefore, it is difficult to elucidate how the students felt about this OSCE in particular. The overall responses to the OSCE were still favorable, indicating the students valued their experiences, with nearly half of the class stating they strongly agreed with the prompt.
Additionally, one of the key goals of the case was to ensure students could generate a comprehensive diagnostic differential. Early in clinical practice, students fail to expand their differential, especially when patients with particularly salient symptoms like amenorrhea present [13,14]. On average, students identified more than one acceptable differential (2.24 acceptable differentials on average). This indicates that despite the challenging nature of the interpersonal relationships of the OSCE, students were able to synthesize the information to reliably consider alternative differential diagnoses such as anorexia nervosa, relative energy deficiency in sports, thyroidopathy, etc.
SP feedback was used to gauge the students’ abilities to create rapport and manage the adolescent-parent dyad. Overall, the SPs stated that students were able to respond to the case with empathy, respect, and support while creating partnerships with them. Most frequently, SPs positively commented on students’ abilities to make them feel comfortable and on students' abilities to give clear explanations. However, SPs noted that students could still work on timing and building rapport before asking sensitive questions. Overall, the feedback indicated that students were able to gain practice with managing the adolescent-parent dyad and helped identify key areas where students could continue to grow.
A limitation of this OSCE is that students received feedback from the SPs through an online service, but given difficulties with granting permissions, many students did not check their feedback. As a key objective of the case is preparing students as clinicians, receiving SP feedback should be prioritized as it can help students adjust their interpersonal navigation practices in preparation for future patients. To address this, SPs could leave feedback in the same rubric that the preceptors fill out; therefore, the preceptors' and SPs’ feedback are stored in one place and are easily accessible for the students. Students could also be given designated debrief or feedback time with the SP and preceptors [15]. Additionally, as the OSCE was integrated into an existing longitudinal medical student course and needed to be conducted in a timely manner, the students were not required to conduct pre and post-comparisons on performance, nor was a control group implemented. To strengthen the study's results, both of these interventions could be implemented to obtain a more quantitative evaluation.
This OSCE was successful in helping medical students gain practice when working with complex adolescent health dynamics. Students gained insight into navigating parent-child dyads and creating valid differential diagnoses despite challenging circumstances. Given the positive feedback from students, SPs, and faculty and ease of setup, the case could be used in a variety of environments to help medical students at other programs, interns, and even residents.
Conclusions
Overall, the OSCE met the objectives set out initially and was seen favorably by SPs, students, and faculty members. The OSCE gave students practice in improving the comfort levels of adolescents and navigating family dynamics as they interact with healthcare professionals. The OSCE can be used to improve students’ abilities to navigate adolescent health cases and family dynamics while being low-cost and effective.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1relationship between adolescent-report of patient-centered care and of the quality of primary care Acad Pediatr Toomey SL Elliott MN Schwebel DC 7707761620162680268410.1016/j.acap.2016.01.006PMC 4958046 · doi ↗ · pubmed ↗
- 2Needs assessment for enhancing pediatric clerkship readiness BMC Med Educ Weinstein A Mac Pherson P Schmidt S 1882320233697808510.1186/s 12909-023-04167-7PMC 10044806 · doi ↗ · pubmed ↗
- 3A novel pediatric clinical skills curriculum to prepare medical students for pediatrics clerkship Med Sci Educ Podraza LC Starnes LS Starnes JR Patel A Apple RK 3433503520254014407910.1007/s 40670-024-02191-w PMC 11933490 · doi ↗ · pubmed ↗
- 4'Demystifying' the encounter with adolescent patients: a qualitative study on medical students' experiences and perspectives during training with adolescent simulated patients Med Educ Online Takeuchi YL Bonvin R Ambresin AE 19794452620213455367410.1080/10872981.2021.1979445 PMC 8462882 · doi ↗ · pubmed ↗
- 5Quality improvement: a template-based approach to HEADSS assessments for hospitalized adolescents Hosp Pediatr Wiley E Kulkarni D Dong H Hwang LY 5885961320233728285310.1542/hpeds.2022-006955 · doi ↗ · pubmed ↗
- 6HEEADSSS 3.0: the psychosocial interview for adolescents updated for a new century fueled by media. Contemporary Pediatrics 5 2025 2014 https://www.contemporarypediatrics.com/view/heeadsss-30-psychosocial-interview-adolescents-updated-new-century-fueled-media
- 7Identification and management of eating disorders in children and adolescents Pediatrics Hornberger LL Lane MA 147202110.1542/peds.2020-04027933386343 · doi ↗ · pubmed ↗
- 8Incidence and outcomes of eating disorders during the COVID-19 pandemic Br J Psychiatry Taquet M Geddes JR Luciano S Harrison PJ 13220202110.1192/bjp.2021.105PMC 761269835048812 · doi ↗ · pubmed ↗