Uptake of Newly Licensed Influenza Vaccine Formulations Among Patients Receiving Chronic Hemodialysis During the 2010/2011 to 2021/2022 Influenza Seasons
John M. Sahrmann, J. Bradley Layton, Katelin B. Nickel, John W. Davis, Vikas R. Dharnidharka, David J. Weber, Anne M. Butler

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
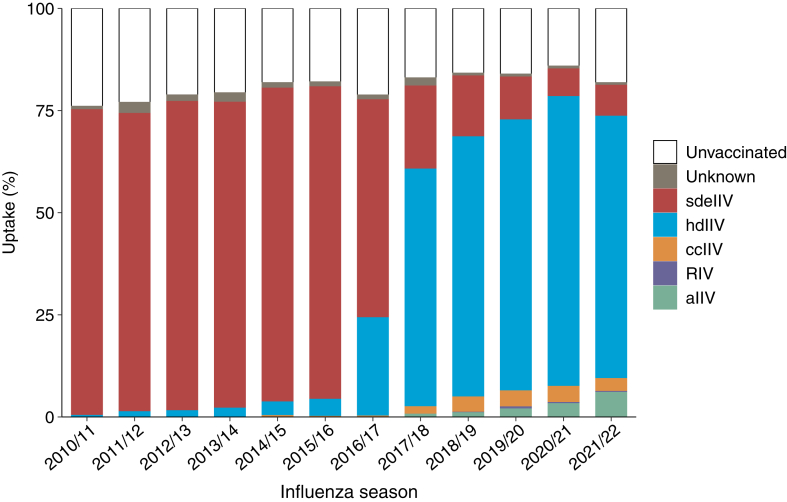 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfluenza Virus Research Studies · Intramuscular injections and effects · Virology and Viral Diseases
To the Editor:
Influenza causes substantial morbidity and mortality in patients with kidney failure. The Centers for Disease Control and Prevention (CDC) has long recommended that patients with kidney failure receive annual influenza vaccination1 but does not state a preferred vaccine formulation. Recently, the CDC preferentially recommended vaccination with enhanced formulations in persons aged ≥65 years including high-dose inactivated influenza vaccine (hdIIV), adjuvanted inactivated influenza vaccine (aIIV), or recombinant influenza vaccine (RIV) vaccine rather than standard-dose, egg-based, inactivated influenza vaccine (sdeIIV). sdeIIV elicits inferior immunogenicity responses in patients with kidney failure relative to the general population and may be inferior in effectiveness to more novel formulations.2, 3, 4 Several enhanced influenza vaccine formulations were introduced in the United States starting in 2009, including hdIIV, aIIV, RIV, and cell culture–based (ccIIV). Before 2013, sdeIIV accounted for most influenza vaccination among patients with kidney failure.5 Otherwise, little is known about utilization of these novel formulations in patients with kidney failure. We sought to evaluate utilization of influenza vaccine formulations from the 2010/2011 to 2021/2022 seasons in a national cohort of patients ≥65 years undergoing hemodialysis.
We used data (including Medicare claims) from the United States Renal Data System (USRDS),6 a government-funded data source including most individuals with kidney failure in the United States. For each influenza season (2010/2011 to 2021/2022; Table S1), we identified a cohort of adults alive on August 1, aged ≥65 years, with Medicare as primary payer, and receiving chronic, in-center hemodialysis for ≥3 months before vaccination. We identified the first influenza vaccination from August 1 to end of influenza season (or December 31, 2021, because of end of available data; Table S2). Patients were eligible for multiple seasons. We assessed demographic and clinical characteristics, comorbid conditions, frailty indicators, preventive health services, and other health care utilization (Table S3).
We identified 400,238 eligible patients who contributed 1,190,564 unique seasons (mean age, 74.6 years; 50.7% male; 60.9% White race; 32.0% Black race; 37.4% Medicaid dual-eligibility). The distribution of influenza vaccine formulations was as follows: sdeIIV (46.3%), hdIIV (31.0%), ccIIV (1.5%), aIIV (1.1%), RIV (0.2%), unknown (1.1%), and unvaccinated (18.8%) (Table 1). Initially, sdeIIV use was predominant; however, use markedly declined from 2010/2011 (74.8%) to 2021/22 (7.6%) (Fig 1). Simultaneously, hdIIV use increased considerably from 2010/2011 (0.6%) to 2021/2022 (64.2%). Particularly notable shifts from sdeIIV to hdIIV occurred in the 2016/2017 and 2017/2018 seasons. By the 2021/2022 season, patients receiving dialysis predominantly received hdIIV, whereas 9.2% received either aIIV or ccIIV. Formulation-specific uptake increased to as high as 6.0% for aIIV in 2021/2022, 3.9% for ccIIV in 2018/2019, and 0.7% for RIV in 2019/20. The proportion of unvaccinated patients decreased from 2010/2011 (24.0%) to 2020/2021 (14.1%), followed by a small increase in 2021/2022 (18.2%). Among all vaccine recipients, ccIIV, aIIV, and RIV recipients were the most likely to reside in the Northeast, and recipients of aIIV and RIV were most likely to attend a nonprofit dialysis clinic and not be dual-eligible for Medicaid (Tables 1 and S4). Unvaccinated individuals generally had lower prevalence of comorbid conditions and preventive health services versus vaccinated patients. Table S5 presents demographic characteristics by season and formulation type.Table 1. Select Demographic and Clinical Characteristics of Patients with Kidney Failure Receiving Chronic Hemodialysis During the 2010/2011 to 2021/2022 Influenza Seasons in the United States, by Influenza Vaccine Formulation.a^,^bCharacteristicsdeIIV (n = 551,811; 46.3%)hdIIV (n = 368,544; 31.0%)ccIIV (n = 18,211; 1.5%)aIIV (n = 12,761; 1.1%)RIV (n = 2,339; 0.2%)Unknown (n = 12,996; 1.1%)Unvaccinated (n = 223,902; 18.8%)Demographic characteristics Age, mean (SD)75 (7.0)75 (7.0)75 (7.2)75 (7.1)75 (7.1)75 (7.1)74 (7.0) Male278,095 (50.4)191,892 (52.1)9,387 (51.5)7,024 (55.0)1,285 (54.9)6,566 (50.5)108,832 (48.6) Race White338,731 (61.4)233,124 (63.3)10,635 (58.4)8,532 (66.9)1,579 (67.5)8,098 (62.3)124,707 (55.7) Black173,413 (31.4)108,200 (29.4)5,670 (31.1)2,906 (22.8)625 (26.7)3,762 (29.0)86,034 (38.4) Other39,667 (7.2)27,220 (7.4)1,906 (10.5)1,323 (10.4)135 (5.8)1,136 (8.7)13,161 (5.9) Residence in metropolitan statistical area485,776 (88.0)323,259 (87.7)16,837 (92.5)11,804 (92.5)2,046 (87.5)11,494 (88.4)199,090 (88.9) Region Northeast94,275 (17.1)60,763 (16.5)5,490 (30.1)3,044 (23.9)730 (31.2)3,468 (26.7)44,003 (19.6) South243,746 (44.2)162,305 (44.0)6,826 (37.5)4,821 (37.8)960 (41.0)4,513 (34.7)96,341 (43.0) West104,414 (18.9)71,315 (19.4)3,377 (18.5)2,902 (22.7)277 (11.8)2,891 (22.2)39,050 (17.4) Midwest109,376 (19.8)74,161 (20.1)2,518 (13.8)1,994 (15.6)372 (15.9)2,124 (16.3)44,508 (19.9) Dual-eligible for Medicaid206,367 (37.4)129,196 (35.1)7,344 (40.3)3,945 (30.9)722 (30.9)5,094 (39.2)92,117 (41.1)Clinical characteristics Years with dialysis treatment <127,374 (5.0)16,674 (4.5)821 (4.5)781 (6.1)133 (5.7)682 (5.2)12,634 (5.6) 1-2184,622 (33.5)115,819 (31.4)5,710 (31.4)4,886 (38.3)813 (34.8)4,272 (32.9)76,178 (34.0) 3-4135,029 (24.5)86,350 (23.4)4,331 (23.8)2,947 (23.1)550 (23.5)3,139 (24.1)52,608 (23.5) 5-9152,341 (27.6)103,379 (28.0)5,170 (28.4)2,868 (22.5)610 (26.1)3,673 (28.3)59,542 (26.6) ≥1052,445 (9.5)46,322 (12.6)2,179 (12.0)1,279 (10.0)233 (10.0)1,230 (9.5)22,940 (10.2)Dialysis facility characteristics Hospital based34,929 (6.3)12,713 (3.5)942 (5.2)1,088 (8.5)185 (7.9)2,930 (22.6)17,765 (7.9) Nonprofit78,557 (14.2)39,549 (10.7)2,774 (15.2)3,137 (24.6)486 (20.8)4,064 (31.3)36,519 (16.3) No of stations 0-19220,923 (40.0)154,334 (41.9)7,245 (39.8)5,038 (39.5)1,075 (46.0)5,072 (39.0)87,696 (39.2) 20-29236,117 (42.8)157,667 (42.8)7,282 (40.0)5,716 (44.8)865 (37.0)5,686 (43.8)95,163 (42.5) ≥3094,771 (17.2)56,543 (15.3)3,684 (20.2)2,007 (15.7)399 (17.1)2,238 (17.2)41,043 (18.3)Health care utilization No. of days hospitalized in last month 0484,617 (87.8)327,283 (88.8)15,858 (87.1)11,403 (89.4)1,997 (85.4)10,761 (82.8)181,384 (81.0) 1-638,315 (6.9)23,220 (6.3)1,240 (6.8)835 (6.5)179 (7.7)1,122 (8.6)20,836 (9.3) ≥728,879 (5.2)18,041 (4.9)1,113 (6.1)523 (4.1)163 (7.0)1,113 (8.6)21,682 (9.7) Skilled nursing facility in last month31,237 (5.7)18,537 (5.0)1,171 (6.4)491 (3.9)146 (6.2)1,173 (9.0)21,723 (9.7)Comorbid conditions Pneumonia105,443 (19.1)47,295 (12.8)27,07 (14.9)1,543 (12.1)342 (14.6)2,946 (22.7)31,424 (14.0) Ischemic heart disease402,421 (72.9)263,384 (71.5)13,511 (74.2)9,245 (72.4)1,725 (73.8)9,863 (75.9)107,241 (47.9) Dementia107,126 (19.4)67,245 (18.2)3,893 (21.4)2,129 (16.7)454 (19.4)3,163 (24.3)37,712 (16.8) Diabetes with chronic complications369,677 (67.0)273,437 (74.2)13,896 (76.3)9,625 (75.4)1,822 (77.9)9,132 (70.3)102,128 (45.6) Diabetes without chronic complications61,692 (11.2)18,607 (5.0)820 (4.5)450 (3.5)92 (3.9)1,268 (9.8)13,069 (5.8) Heart failure396,772 (71.9)267,586 (72.6)13,463 (73.9)9,194 (72.0)1,709 (73.1)9,764 (75.1)108,506 (48.5) Hypertension (uncomplicated or complicated)545,500 (98.9)365,540 (99.2)18,069 (99.2)12,680 (99.4)2,329 (99.6)12,896 (99.2)141,497 (63.2) Liver disease108,553 (19.7)67,444 (18.3)3,715 (20.4)2,258 (17.7)417 (17.8)2,631 (20.2)32,723 (14.6)Frailty markers Stroke or brain injury206,879 (37.5)155,476 (42.2)8,178 (44.9)5,138 (40.3)1,064 (45.5)5,616 (43.2)66,873 (29.9)Preventive health services Cancer screening17,437 (3.2)14,780 (4.0)711 (3.9)591 (4.6)111 (4.8)403 (3.1)4,145 (1.9) Hemoglobin A_1c_ test300,945 (54.5)191,014 (51.8)10,370 (56.9)6,850 (53.7)1,221 (52.2)6,550 (50.4)74,009 (33.0) Diabetic eye examination179,736 (32.6)114,364 (31.0)5,978 (32.8)4,448 (34.9)815 (34.8)4,287 (33.0)42,593 (19.0)Abbreviations: aIIV, adjuvanted inactivated influenza vaccine; ccIIV, cell culture-based inactivated influenza vaccine; hdIIV, high-dose inactivated influenza vaccine; RIV, recombinant influenza vaccine; SD, standard deviation; sdeIIV, standard dose, egg-based inactivated influenza vaccine.aResults are expressed as n (%) unless otherwise indicated.bTable S3 presents the definitions and timing of assessment for all patient characteristics.Figure 1. Uptake of influenza vaccine formulations among patients with kidney failure receiving chronic hemodialysis, during the 2010/2011 to 2021/2022 influenza seasons in the United States.
We documented dramatic increases in uptake of newly licensed influenza vaccines among patients with kidney failure between the 2010/2011 and 2021/2022 influenza seasons, possibly reflecting changes in the formularies of large commercial dialysis providers because of increasing data of improved effectiveness of these vaccines in all persons ≥65 years. Our findings in the dialysis population generally reflect patterns in the general population. In our study, the proportion of patients ≥65 years with kidney failure in the United States who received influenza vaccination increased from 76.0% to 85.9% from 2010/2011 (24.0%) to 2020/2021, which is similar but higher than estimates in the general population (2011-2013: 59.1%; 2021-2023: 67.5%).7 Similar to our findings in the dialysis population, the Medicare-insured general population experienced dramatic increases over time in use of newly licensed vaccines.4^,^8 Notably, our results indicate that the dialysis population has higher uptake of hdIIV but lower uptake of other newly licensed vaccines than the Medicare population. For example, a study of 12.7 million Medicare-insured influenza vaccine recipients during the 2019/2020 influenza season reported the following distribution: 69.0% hdIIV, 24.7% aIIV, 15.0% sdeIIV, 7.9% ccIIV, and 6.3% RIV.8
Our study had several limitations. First, patients vaccinated in 2022 were misclassified as unvaccinated in the 2021/2022 season because of end of data (although <1% of vaccinations occurred after December 31 in each prior season). Additionally, some vaccinations may have been missed because vaccinations were identified using Current Procedural Terminology (CPT), Healthcare Common Procedure Coding System (HCPCS), International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), and International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) codes for insurance reimbursement purposes but not national drug codes billed by retail pharmacies; we expect this to be rare because patients with kidney failure receive in-center dialysis typically thrice weekly and receive reimbursement for influenza vaccines via Medicare Part B. Lastly, some important predictors of vaccine receipt (eg, health-seeking behaviors, personal beliefs) may not be observable in billing claims.
Our observation of increasing utilization of newly licensed influenza vaccine formulations in the dialysis population highlights the need for an updated evaluation of the comparative effectiveness and safety of influenza vaccines in this high-risk population.9^,^10
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Grohskopf L.A.Ferdinands J.M.Blanton L.H.Broder K.R.Loehr J.Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices—United States, 2024–25 influenza season MMWR Recomm Rep 73202412510.15585/mmwr.rr 7305 a 1PMC 1150100939197095 · doi ↗ · pubmed ↗
- 2Vogtländer N.P.J.Brown A.Valentijn R.M.Rimmelzwaan G.F.Osterhaus A.D.M.E.Impaired response rates, but satisfying protection rates to influenza vaccination in dialysis patients Vaccine 222004219922011514977710.1016/j.vaccine.2003.11.046 · doi ↗ · pubmed ↗
- 3Mc Grath L.J.Kshirsagar A.V.Cole S.R.Influenza vaccine effectiveness in patients on hemodialysis: an analysis of a natural experiment Arch Intern Med 17220125485542249346210.1001/archinternmed.2011.2238 PMC 4082376 · doi ↗ · pubmed ↗
- 4Izurieta H.S.Chillarige Y.Kelman J.Relative effectiveness of influenza vaccines among the United States elderly, 2018-2019 J Infect Dis 22220202782873210000910.1093/infdis/jiaa 080 · doi ↗ · pubmed ↗
- 5Mc Grath L.J.Layton J.B.Krueger W.S.Kshirsagar A.V.Butler A.M.High-dose influenza vaccine use among patients receiving hemodialysis in the United States, 2010–2013 Vaccine 362018608760943019548610.1016/j.vaccine.2018.08.079PMC 6176722 · doi ↗ · pubmed ↗
- 6Johansen K.L.Gilbertson D.T.Li S.US Renal Data System 2023 Annual Data Report: epidemiology of kidney disease in the United States Am J Kidney Dis 83Suppl 12024 A 8A 133851926210.1053/j.ajkd.2024.01.001 · doi ↗ · pubmed ↗
- 7Tao H.Chen J.Zhang X.Wang T.Jiang N.Jia Y.Sociodemographic disparities in influenza vaccination among older adults in United States Front Public Health 132025147467710.3389/fpubh.2025.1474677 PMC 1184304539991691 · doi ↗ · pubmed ↗
- 8Izurieta H.S.Lu M.Kelman J.Comparative effectiveness of influenza vaccines among US Medicare beneficiaries ages 65 years and older during the 2019–2020 season Clin Infect Dis 732021 e 4251 e 42593321180910.1093/cid/ciaa 1727 · doi ↗ · pubmed ↗