Serum S100A8 as a potential biomarker for diagnosis of antiphospholipid syndrome and risk stratification among aPL carriers
Liang Luo, Yuebing Wang, Wenhua Zhu, Xiangjun Liu, Lei Zhu, Ru Li, Chun Li

TL;DR
This study explores serum S100A8 as a potential biomarker for diagnosing antiphospholipid syndrome and assessing risk in carriers of antiphospholipid antibodies.
Contribution
The study introduces serum S100A8 as a novel biomarker for antiphospholipid syndrome diagnosis and risk stratification.
Findings
Serum S100A8 levels were significantly higher in aPL carriers and APS patients compared to healthy controls.
S100A8 showed good diagnostic accuracy for APS with an AUC of 0.854.
S100A8 positivity was independently associated with increased obstetric APS risk among aPL carriers.
Abstract
Current diagnosis of antiphospholipid syndrome (APS) relies on antiphospholipid antibodies (aPL) testing, but false-positive aPL results and asymptomatic aPL carriers pose significant clinical challenges. The importance of S100A8 in thrombosis has been demonstrated, yet its potential role in APS has received little attention. This study aimed to assess serum S100A8 for APS diagnosis and risk stratification among aPL carriers. Serum S100A8 levels were measured by ELISA in healthy controls (HCs), aPL carriers without manifestation and patients with APS. Receiver operating characteristic curves were used to evaluate the diagnostic performance of APS. Logistic regression was performed to identify independent variables associated with obstetric morbidity among female aPL carriers. The study enrolled 120 HCs, 57 aPL carriers and 114 patients with APS. Serum S100A8 levels were significantly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
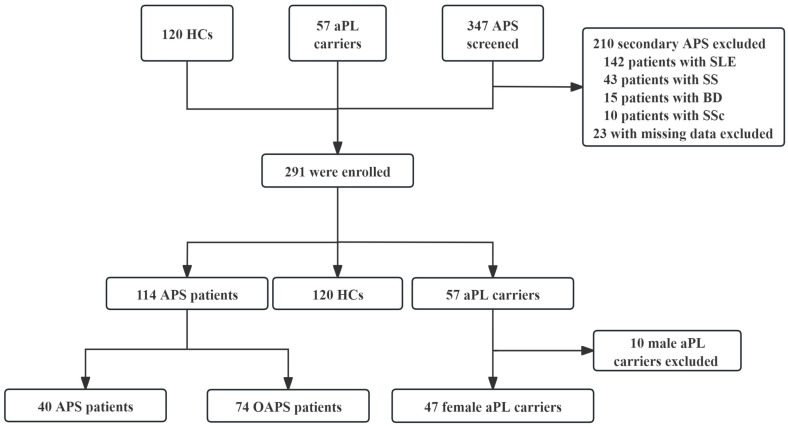 Figure 1
Figure 1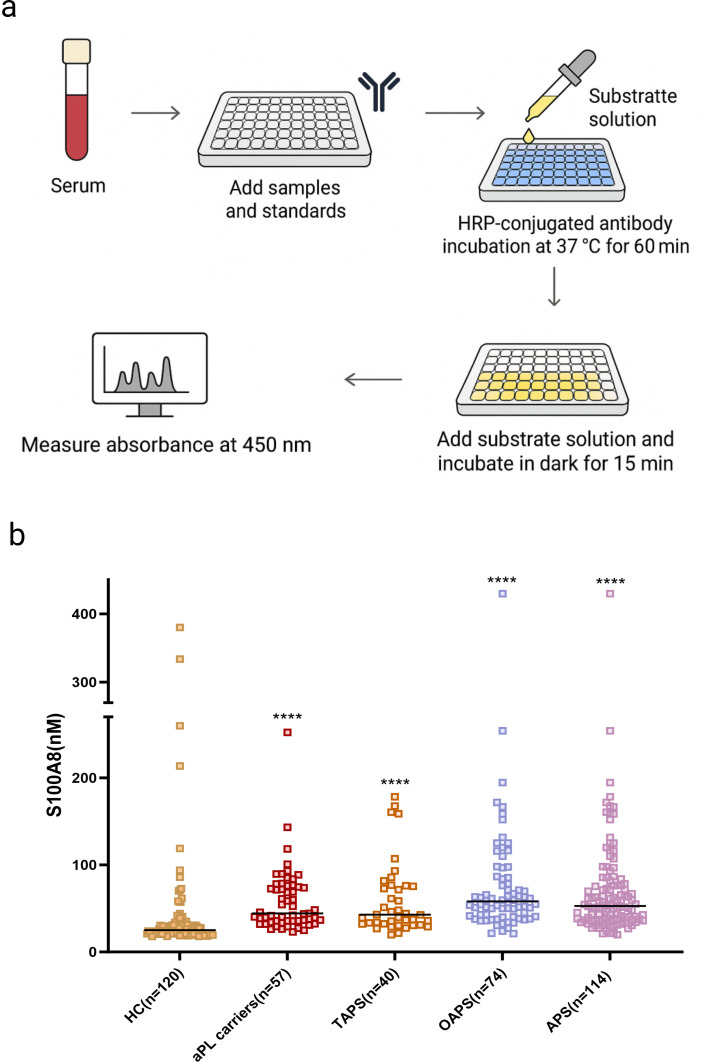 Figure 2
Figure 2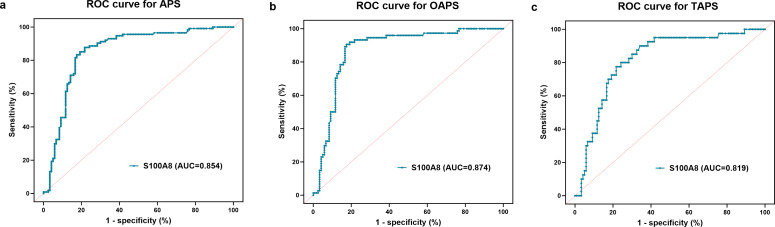 Figure 3
Figure 3| Variables | HCs | aPL carriers (n=57) | Patients with APS (n=114) | Patients with TAPS (n=40) | Patients with OAPS (n=74) | P value | P value | P value |
|---|---|---|---|---|---|---|---|---|
| Age, years (x̄±s) | 42.4±12.7 | 40.3±12.1 | 42.1±13.6 | 53.3±16.6 | 36.1±6.0 | 0.394 | 0.005 | 0.018 |
| Female, n (%) | 75 (62.5) | 47 (82.5) | 103 (90.4) | 29 (72.5) | 74 (100.0) | 0.138 | 0.241 | 0.001 |
| Smoking, n (%) | 0 (0) | 3 (5.3) | 8 (7.0) | 8 (20.0) | 0 (0) | 0.912 | 0.054 | 0.080 |
| Hypertension, n (%) | 0 (0) | 3 (5.3) | 23 (20.2) | 19 (47.5) | 4 (5.4) | 0.010 | <0.001 | 1.000 |
| Hyperlipidaemia, n (%) | 0 (0) | 4 (7.0) | 8 (7.0) | 7 (63.6) | 1 (1.4) | 1.000 | 0.201 | 0.166 |
| Diabetes, n (%) | 0 (0) | 4 (7.0) | 6 (5.3) | 6 (15.0) | 0 (0) | 0.908 | 0.203 | 0.034 |
| Coronary heart disease, n (%) | 0 (0) | 1 (1.8) | 7 (6.1) | 7 (17.5) | 0 (0) | 0.271 | 0.008 | 0.435 |
| Thrombosis, n (%) | 0 (0) | 0 (0) | 40 (35.1) | 40 (100.0) | 0 (0) | – | – | – |
| Obstetric morbidity, n (%) | 0 (0) | 0 (0) | 74 (64.9) | 0 (0) | 74 (100.0) | – | – | – |
| Leucopenia, n (%) | 0 (0) | 1 (1.9) | 6 (5.6) | 5 (13.2) | 1 (1.4) | 0.429 | 0.092 | 1.000 |
| Anaemia, n (%) | 0 (0) | 5 (9.5) | 18 (16.7) | 11 (28.9) | 7 (10.0) | 0.234 | 0.018 | 0.944 |
| Thrombocytopenia, n (%) | 0 (0) | 0 (0) | 18 (15.8) | 13 (32.5) | 5 (6.8) | – | – | – |
| ANA (+), n (%) | 0 (0) | 11 (19.3) | 45 (39.5) | 17 (42.5) | 28 (37.8) | 0.026 | 0.013 | 0.021 |
| Anti-β2 glycoprotein I antibodies (+), n (%) | 0 (0) | 42 (73.7) | 85 (74.6) | 24 (60.0) | 61 (82.4) | 0.902 | 0.155 | 0.226 |
| Anticardiolipin antibodies (+), n (%) | 0 (0) | 25 (43.9) | 39 (34.4) | 19 (47.5) | 20 (27.0) | 0.219 | 0.723 | 0.044 |
| Lupus anticoagulant (+), n (%) | 0 (0) | 27 (47.4) | 47 (41.2) | 21 (52.5) | 26 (35.1) | 0.445 | 0.619 | 0.157 |
| Elevated erythrocyte sedimentation rate, n (%) | 0 (0) | 4 (9.3) | 14 (21.9) | 9 (31.0) | 5 (14.3) | 0.088 | 0.019 | 0.742 |
| Elevated C reactive protein, n (%) | 0 (0) | 1 (3.1) | 12 (18.5) | 3 (10.3) | 9 (25.0) | 0.055 | 0.338 | 0.028 |
| Low complement 3, n (%) | 0 (0) | 13 (22.8) | 17 (18.1) | 10 (26.3) | 13 (17.6) | 0.481 | 0.696 | 0.456 |
| Low complement 4, n (%) | 0 (0) | 9 (18.4) | 19 (20.0) | 12 (31.6) | 7 (12.3) | 0.815 | 0.153 | 0.383 |
| Treatment, n (%) | ||||||||
| Anticoagulant | – | 16 (28.1) | 60 (52.6) | 20 (50.0) | 40 (54.2) | 0.004 | 0.047 | 0.005 |
| Low-dose aspirin | – | 30 (52.6) | 55 (48.2) | 6 (15.0) | 49 (66.2) | 0.705 | <0.001 | 0.163 |
| Hydroxychloroquine | – | 42 (73.7) | 71 (62.3) | 21 (52.5) | 50 (67.6) | 0.189 | 0.053 | 0.571 |
| Immunosuppressant | – | 22 (38.6) | 32 (28.1) | 22 (55.0) | 10 (13.5) | 0.222 | 0.164 | 0.002 |
| Variables | Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| B | OR | 95% CI | P value | B | OR | 95% CI | P value | |
| Age, years | −0.042 | 0.959 | 0.917 to 1.002 | 0.064 | −0.031 | 0.970 | 0.921 to 1.020 | 0.236 |
| S100A8 (+), n (%) | 1.073 | 2.925 | 1.044 to 8.197 | 0.048 | 1.204 | 3.335 | 1.010 to 11.012 | 0.048 |
| ANA (+), n (%) | 0.944 | 2.570 | 1.082 to 6.105 | 0.032 | 1.694 | 5.439 | 1.834 to 16.131 | 0.002 |
| aβ2GPI (+), n (%) | 0.475 | 1.609 | 0.662 to 3.909 | 0.294 | 0.216 | 1.241 | 0.425 to 3.624 | 0.693 |
| Anticardiolipin antibodies (+), n (%) | −0.693 | 0.500 | 0.231 to 1.083 | 0.079 | −0.821 | 0.440 | 0.175 to 1.107 | 0.081 |
| LA (+), n (%) | −0.549 | 0.577 | 0.274 to 1.217 | 0.149 | −0.735 | 0.479 | 0.184 to 1.248 | 0.132 |
| Anticoagulant, n (%) | 0.920 | 2.510 | 1.168 to 5.393 | 0.018 | 0.843 | 2.324 | 0.861 to 6.275 | 0.096 |
| LDA, n (%) | 0.545 | 1.725 | 0.816 to 3.646 | 0.153 | 0.500 | 1.649 | 0.582 to 4.667 | 0.346 |
| HCQ, n (%) | −0.336 | 0.714 | 0.316 to 1.616 | 0.419 | −0.642 | 0.526 | 0.190 to 1.459 | 0.217 |
| Immunosuppressant, n (%) | −0.895 | 0.409 | 0.162 to 1.029 | 0.058 | −0.287 | 0.750 | 0.250 to 2.256 | 0.609 |
- —Shandong Provincial Natural Science Foundation
- —Peking University People’s Hospital Research And Development Fund
- —The People’s Hospital of Yubei District of Chongqing Clinical Research Project
- —Chongqing Yubei District Science and Health Joint Medical Research Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · S100 Proteins and Annexins · Blood Coagulation and Thrombosis Mechanisms
Introduction
Antiphospholipid syndrome (APS) is a systemic autoimmune disorder defined by the occurrence of thrombotic events and/or obstetric morbidity in the presence of persistent antiphospholipid antibodies (aPL), including lupus anticoagulant (LA), anticardiolipin antibodies (aCL) and anti-β2 glycoprotein I antibodies (aβ2GPI).1 Epidemiological data indicate that APS affects 1–2 individuals per 100 000 annually, with a prevalence of up to 50 per 100 000 and a rising trend.2 3 APS primarily affects young individuals, and severe thrombotic events can be life-threatening, with mortality reaching 50% in cases of catastrophic APS.4 Although current classification criteria rely heavily on aPL detection, laboratory assays are sometimes limited by false positives and variable clinical correlation.5 Importantly, clinical manifestations remain central to diagnosis, yet the management of persistently aPL carriers without definite APS features is still difficult due to the absence of reliable biomarkers for risk stratification.
S100A8 is a calcium-binding protein highly expressed in neutrophil cytoplasm, where it forms a heterodimer with S100A9 known as calprotectin. S100A8/A9 is stored in the cytosolic fraction and is released predominantly during the formation of neutrophil extracellular traps (NETs).6 Recent studies have highlighted the role of neutrophils and NETs, which are prothrombotic and proinflammatory networks of DNA and proteins, in the pathophysiology of APS.7 8 Elevated levels of circulating NET remnants have been observed in patients with APS,9 and aPL can trigger NET release by activating neutrophils.10 Once released, calprotectin promotes inflammation and thrombosis by engaging pattern recognition receptors, such as Toll-like receptor 4 (TLR4) and the receptor for advanced glycation end-products (RAGE), contributing to endothelial activation and leucocyte recruitment.11 12 Elevated S100A8 levels have also been reported in thrombosis.13 However, its clinical relevance in APS, particularly in obstetric APS (OAPS), remains poorly defined. This study aimed to investigate serum S100A8 levels among healthy controls (HCs), aPL carriers without clinical manifestations and patients with APS. Additionally, we assessed the diagnostic performance of S100A8 in identifying APS and its clinical subtypes, including thrombotic APS (TAPS) and OAPS, and explored its potential association with morbidity in aPL carriers.
Materials and methods
Study design and participants
This was a cross-sectional study conducted at Peking University People’s Hospital between June 2016 and August 2024. A total of 524 individuals were initially screened. After the exclusion of ineligible participants, 291 participants were enrolled, including HCs, aPL carriers and primary APS. The flowchart of the study is shown in figure 1.
Flowchart of the study. aPL carriers, antiphospholipid antibody positive without clinical manifestations; APS, antiphospholipid syndrome; BD, Behçet's disease; HCs, healthy controls; OAPS, obstetric APS; SS, Sjögren syndrome; SSc, systemic sclerosis; TAPS, thrombotic APS.
All patients with APS fulfilled the 2006 Sydney and 2023 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria of APS.1 14 Patients with APS were further classified into TAPS and OAPS based on their clinical manifestations. aPL carriers were defined as those who persistently tested positive for aPL (including LA, aCL or aβ2GPI) at least two times 12 weeks apart but without any clinical manifestations. HCs were age- and sex-matched volunteers with no history of autoimmune disease, thrombosis, pregnancy complications or aPL positivity. Individuals with secondary APS due to SLE or other autoimmune disorders, or with missing clinical or laboratory data, were excluded.
Data collection
Demographics, cardiovascular risk factors, clinical manifestations and laboratory data were collected from the hospital’s electronic medical records at the time of enrolment. Demographics included age and sex. Cardiovascular risk factors comprised smoking, hypertension, hyperlipidaemia, diabetes and coronary heart disease. Clinical manifestations included thrombotic events and obstetric morbidity. Laboratory indicators included haematological abnormalities (leucopenia, anaemia and thrombocytopenia), aPL (aβ2GPI, aCL and LA), inflammatory markers (C reactive protein and erythrocyte sedimentation rate) and complement components. Treatment included low-dose aspirin (LDA), anticoagulants, hydroxychloroquine (HCQ) and immunosuppressants.
Serum S100A8 testing
Serum S100A8 levels were measured using a commercial human ELISA kit (CHEJETER, China; Catalogue No. CJT12029; 96T format) following the manufacturer’s instructions. The ELISA kit specifically detects free S100A8 monomers. This assay exhibits negligible cross-reactivity with the S100A8/A9 heterodimer (calprotectin) due to conformational masking of target epitopes in the heterocomplex. Samples and standards were added to pre-equilibrated wells, followed by horseradish peroxidase-conjugated antibody incubation at 37 °C for 60 min. After washing, substrate solutions were added and incubated in the dark for 15 min. The reaction was stopped, and absorbance was measured at 450 nm (figure 2a). All samples were tested in duplicate, and mean values were used for analysis.
*Measurement of serum S100A8 in 291 research subjects. (a) Schematic illustration of the S100A8 ELISA. (b) Differences in S100A8 levels among HCs, aPL carriers and patients with APS. ***p<0.001 compared with HCs. aPL carriers, antiphospholipid antibody positive without clinical manifestations; APS, antiphospholipid syndrome; HCs, healthy controls; OAPS, obstetric APS; TAPS, thrombotic APS.
Statistical analysis
Continuous variables were tested for normality using the single-sample Kolmogorov-Smirnov test. Normally distributed data are presented as mean±SD and compared using the Student’s t-test. Non-normally distributed data are expressed as median with IQR and compared using the Mann-Whitney U test or Kruskal-Wallis test, as appropriate. Categorical variables are presented as frequencies and percentages and were compared using the χ^2^ test or Fisher’s exact test. The Bonferroni correction was applied for multiple comparisons where appropriate. As the proportion of missing data was <5% and the missingness was random, we did not apply data imputation.
Receiver operating characteristic (ROC) curves were performed to evaluate the diagnostic performance of serum S100A8 in identifying APS and its clinical subtypes. The area under the curve (AUC), optimal cut-off, sensitivity and specificity were calculated. Binary logistic regression analysis was performed to identify independent variables associated with obstetric morbidity among aPL carriers. Variables with p<0.05 in univariate analysis were entered into multivariate models (adjusted for aβ2GPI and LA). All statistical analyses were performed using SPSS V.26.0 (SPSS, Chicago, Illinois, USA) and GraphPad Prism V.10.1.2.
Results
Demographic and laboratory characteristics
A total of 120 HCs, 57 aPL carriers and 114 patients with APS, including 40 with TAPS and 74 with OAPS, were enrolled in this study. The baseline characteristics of HCs, aPL carriers and patients with APS are summarised in table 1. Compared with aPL carriers, TAPS patients were older (53.3±16.6 vs 40.3±12.1 years, p=0.005), while OAPS patients tended to be younger (36.1±6.0 vs 40.3±12.1 years, p=0.018). Hypertension was more common in patients with APS than in aPL carriers (20.2% vs 5.3%, p=0.010), especially those with TAPS (47.5% vs 5.3%, p<0.001). A higher rate of coronary heart disease (17.5% vs 1.8%, p=0.008), anticoagulant use (50.0% vs 28.1%, p=0.047) and a lower rate of LDA use (15.0% vs 52.6%, p<0.001) were observed in patients with TAPS compared with aPL carriers. In addition, aPL carriers had higher positivity rates of aCL compared with patients with OAPS (43.9% vs 27.0%, p=0.044). aPL carriers had a lower rate of ANA positivity than patients with APS (19.3% vs 39.5%, p=0.026). After Bonferroni correction (p<0.002), the high prevalence of hypertension and use of LDA in patients with TAPS remained significant.
Details of manifestations of OAPS phenotypes in patients were shown in online supplemental table 1. Compared with HCs, serum S100A8 levels were elevated in both isolated early pregnancy loss (59.7 (46.3–86.8) ng/mL, p<0.001) and isolated late pregnancy complication patients (61.7 (49.9–98.1) ng/mL, p<0.001). Moreover, S100A8 levels were significantly higher in late complication patients compared with aPL carriers (48.1 (35.1–77.4) ng/mL, p=0.020). There was no significant difference in serum S100A8 levels between patients with isolated early pregnancy loss and isolated late complications (online supplemental figure 1).
S100A8 levels among the study population
Serum S100A8 levels were significantly elevated in aPL carriers and patients with APS compared with HCs. The median S100A8 concentration in HCs was 25 (IQR 21.6–31.1) ng/mL, which was markedly lower than that in aPL carriers (44.3 (35.6–75.4) ng/mL, p<0.001) and patients with APS (52.8 (37.2–79.2) ng/mL, p<0.001) (figure 2b). The median S100A8 concentration in patients with TAPS and OAPS was 42.8 (32.3–76.0) ng/mL and 58 (40.5–85.7) ng/mL, respectively, which was significantly higher than HCs (figure 2b).
Diagnostic performance of S100A8
The AUC for identifying overall patients with APS was 0.854 (95% CI 0.803 to 0.907), with a sensitivity of 87.7% and a specificity of 78.3% at the optimal cut-off value of 32.19 ng/mL (p<0.001). In subgroup analyses, S100A8 also demonstrated high diagnostic accuracy for both TAPS and OAPS. The AUC was 0.819 (95% CI 0.747 to 0.891) for TAPS, with 80% sensitivity and 75.8% specificity at a cut-off of 31.10 ng/mL (p<0.001). For OAPS, the AUC was 0.874 (95% CI 0.821 to 0.926), with 90.5% sensitivity and 82.5% specificity at a cut-off of 34.02 ng/mL (p<0.001) (figure 3 and online supplemental table 2).
ROC curves of S100A8 for identifying APS and different clinical subtypes. (a) ROC curve for overall APS patients; (b) ROC curve for TAPS; (c) ROC curve for OAPS. The AUC values are shown in each panel. APS, antiphospholipid syndrome; AUC, area under the curve; OAPS, obstetric APS; ROC, receiver operating characteristic; TAPS, thrombotic APS.
Subgroup analysis
Baseline demographic and laboratory characteristics of female aPL carriers were shown in online supplemental table 3. After adjusting for aβ2GPI, LA positivity, LDA, HCQ and immunosuppressants, multivariate logistic regression analysis showed S100A8 positivity (OR 3.335, 95% CI 1.010 to 11.012, p=0.048) and ANA positivity (OR=5.439, 95% CI 1.834 to 16.131, p=0.002) were independently associated with an increased risk of OAPS among aPL carriers (table 2). No significant associations were observed between aPL carriers and patients with TAPS.
Discussion
This study showed that serum S100A8 levels were significantly elevated in aPL carriers and patients with APS. Moreover, S100A8 exhibited good diagnostic performance for identifying APS and its subtypes. Multivariate logistic regression analysis revealed that S100A8 positivity was independently associated with an increased risk of obstetric morbidity among female aPL carriers.
The elevated serum S100A8 levels observed in patients with APS may reflect enhanced neutrophil activation and NETs formation, processes implicated in both thrombotic and obstetric manifestations. In TAPS, NETs have been shown to promote endothelial injury and thrombosis through the activation of platelets and the coagulation cascade.15 16 However, the most pronounced increase in S100A8 levels was observed in patients with OAPS, suggesting an important role in pregnancy-related complications. aPL can trigger the release of NETs at the maternal–foetal interface, leading to increased reactive oxygen species production and trophoblast apoptosis, ultimately contributing to placental injury in OAPS.17 As a major cytosolic component of NETs, S100A8 may engage innate immune receptors such as TLR4 and RAGE on decidual and endothelial cells, promoting inflammation, endothelial dysfunction and trophoblast injury.18 These mechanisms may underlie the association between S100A8 and obstetric morbidity, highlighting its potential as a biomarker of placental immune dysregulation in OAPS.
The clinical spectrum of OAPS is heterogeneous, encompassing both recurrent early losses and late pregnancy complications such as severe pre-eclampsia and foetal growth restriction. Notably, the latter is considered more specific to APS pathology.14 19 Interestingly, our study found that serum S100A8 levels were similarly elevated in patients with isolated recurrent early losses and those with isolated late pregnancy complications. Both subgroups had significantly higher S100A8 levels compared with HCs. This phenotypic independence suggests that the elevated S100A8 may reflect a common, upstream proinflammatory endothelial environment driven by aPL, serving as a shared risk for various obstetric manifestations.
Although the role of S100A8/A9 has been explored in other autoimmune diseases,2022 its involvement in APS, especially in OAPS, remains inadequately characterised. Elevated calprotectin levels have been observed in primary APS patients and in asymptomatic aPL carriers, indicating a potential contribution to disease processes such as endothelial activation and thrombus formation.23 While the S100A8/A9 heterodimer (calprotectin) is established as a downstream thrombotic effector that directly activates platelets via epithelial growth factor receptor-dependent pathways to promote coagulation,24 free S100A8 functions as an upstream inflammatory alarmin. S100A8 initiates vascular inflammation by activating the endothelial TLR4/mitogen-activated protein kinase axis and amplifying the NOD-, LRR- and pyrin domain-containing protein 3 (NLRP3)/Caspase-1/interleukin-1β pathway,25 26 which are potential processes in APS-related endothelial injury and placental dysfunction.27 28 Prior evidence suggests that elevated circulating free S100A8 serves as an early diagnostic biomarker in thromboembolic diseases.29 Our findings revealed significantly elevated serum S100A8 levels in both patients with APS and aPL carriers compared with HCs, suggesting early immune or vascular activation prior to clinical onset.
Our results showed that S100A8 has good diagnostic potential for APS and its subtypes. The current diagnosis of APS requires both clinical manifestations and persistent positivity for aPL.14 However, this approach has notable limitations. Some patients initially test negative for standard aPLs despite clinical features suggestive of APS. In our previous study, the inclusion of non-criteria aPLs significantly enhanced diagnostic accuracy in seronegative APS.30 Moreover, aPL levels may fluctuate over time, and their correlation with clinical events is not always consistent.31 Therefore, independent of traditional aPL profiles, S100A8 may provide complementary diagnostic value in APS, particularly in cases with ambiguous clinical presentations or borderline serological findings.
This study indicated S100A8 positivity was independently associated with increased OAPS risk among aPL carriers. Given its presumed involvement in neutrophil activation and NETs formation,6 S100A8 may contribute to placental immune dysregulation and inflammation, potentially impairing pregnancy outcomes. These findings suggest that S100A8 may serve not only as a biomarker reflecting heightened neutrophil-driven inflammation but also as a potential effector molecule linking innate immune activation to thrombogenic processes in OAPS.32 Its upregulation could exacerbate endothelial dysfunction33 and promote procoagulant activity, thereby facilitating placental thrombosis and foetal loss. Further mechanistic studies are warranted to elucidate whether targeting the S100A8–NETs axis could mitigate inflammatory and thrombotic cascades in OAPS.
Our study has several limitations. First, the relatively small sample size, especially in subgroup analyses, may reduce the statistical power of the findings. Second, all participants were recruited from a single centre, which may limit the generalisability of the results. Third, the study lacked mechanistic investigations to clarify the role of S100A8 in APS-related immune or inflammatory pathways. Fourth, the retrospective design limited the availability of complete IgG/IgM isotype data for aPLs, precluding a comprehensive cohort-wide analysis of isotype–phenotype associations. Further multicentre studies incorporating basic experimental research are needed to validate and expand upon these findings.
Conclusion
Serum S100A8 levels were significantly elevated in patients with APS and aPL carriers. S100A8 demonstrated good diagnostic performance and was independently associated with obstetric morbidity. These findings suggest its potential as a complementary biomarker for APS diagnosis and obstetric risk assessment among aPL carriers.
Supplementary material
10.1136/lupus-2025-001873online supplemental file 1
10.1136/lupus-2025-001873online supplemental file 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Miyakis S Lockshin MD Atsumi T et al International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS)J Thromb Haemost 2006429530610.1111/j.1538-7836.2006.01753.x 16420554 · doi ↗ · pubmed ↗
- 2Dabit JY Valenzuela-Almada MO Vallejo-Ramos S et al Epidemiology of Antiphospholipid Syndrome in the General Population Curr Rheumatol Rep 2022238510.1007/s 11926-021-01038-234985614 PMC 8727975 · doi ↗ · pubmed ↗
- 3Ioannou Y Beukelman T Murray M et al Incidence of Antiphospholipid Syndrome: Is Estimation Currently Possible?Eur J Rheumatol 202310394410.5152/eurjrheum.2023.2201236880810 PMC 10152079 · doi ↗ · pubmed ↗
- 4Schreiber K Sciascia S de Groot PG et al Antiphospholipid syndrome Nat Rev Dis Primers 201841710310.1038/nrdp.2017.10329321641 · doi ↗ · pubmed ↗
- 5Qiao J Bailly J Opie J Key Issues at the Forefront of Diagnosis and Testing for Antiphospholipid Syndrome Clin Appl Thromb Hemost 2024301076029624130675110.1177/1076029624130675139692090 PMC 11653459 · doi ↗ · pubmed ↗
- 6Sprenkeler EGG Zandstra J van Kleef ND et al S 100A 8/A 9 Is a Marker for the Release of Neutrophil Extracellular Traps and Induces Neutrophil Activation Cells 20221123610.3390/cells 1102023635053354 PMC 8773660 · doi ↗ · pubmed ↗
- 7Ambati A Zuo Y Knight JS An update on inflammation in antiphospholipid syndrome Curr Opin Rheumatol 202335899710.1097/BOR.000000000000092636580355 PMC 9877197 · doi ↗ · pubmed ↗
- 8Tambralli A Gockman K Knight JS NE Ts in APS: Current Knowledge and Future Perspectives Curr Rheumatol Rep 2020226710.1007/s 11926-020-00936-132845378 · doi ↗ · pubmed ↗