Mpox Outbreak in the East Africa Region: Current Status, Containment Measures, Challenges, and Future Direction
Reuben Sindayiheba, Noel Gahamanyi, Jerome Ndayisenga, Edouard Ntagwabira, Emmanuel Nsengiyumva, Emmanuel Kabalisa, Gashegu Misbah, Isabelle Mukagatare, Leon Mutesa, Claude Mambo Muvunyi

TL;DR
The Mpox outbreak in East Africa, led by the DRC, highlights transmission challenges and the need for regional cooperation to strengthen outbreak preparedness and resource access.
Contribution
This study provides a comprehensive review of Mpox outbreak status, containment measures, and challenges in East Africa, emphasizing the need for a coordinated regional strategy.
Findings
The DRC had the highest Mpox cases and deaths in the EAC region as of July 2025.
Over 73% of MVA-BN vaccine doses were administered in the DRC.
Healthcare infrastructure limitations and misinformation hindered outbreak control.
Abstract
In 2024, the World Health Organization declared Mpox outbreak a Public Health Emergency of International Concern. The epicenter of this outbreak was the Democratic Republic of Congo (DRC), which is a member of the East African Community (EAC). The majority of EAC countries reported Mpox cases and associated deaths. Mpox outbreak negatively affected EAC member states but triggered the strengthening of diagnostic and surveillance capacity. This review assessed the status, containment measures, challenges, and future directions of Mpox in the EAC. As of July 27, 2025, the DRC was the top country in the world with Mpox with 28,165 cases and 69 deaths, followed by Uganda, Burundi, Kenya, Rwanda, Tanzania, and South Sudan with 7648 cases and 48 deaths, 4231 cases and one death, 281 cases and five deaths, 124 cases, 111 cases, and 17 cases, respectively. Rwanda, Tanzania, and South Sudan have…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
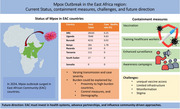 Figure 1
Figure 1| S/N | Country | Total cases | Total deaths | CFR (%) | Most affected age group |
|---|---|---|---|---|---|
| 1. | DRC | 28,165 | 69 | 0.25 | Multiple age groups |
| 2. | Uganda | 7648 | 48 | 0.63 | 20–29 years |
| 3. | Burundi | 4231 | 1 | 0.02 | Children ≤15 (39.5%) |
| 4. | Kenya | 281 | 5 | 1.78 | Multiple age groups |
| 5. | Rwanda | 124 | 0 | 0 | Multiple age groups |
| 6. | Tanzania | 111 | 0 | 0 | Multiple age groups |
| 7. | South Sudan | 17 | 0 | 0 | Multiple age groups |
| 8. | Somalia | 0 | 0 | 0 | Multiple age groups |
| Country | Key containment measures | Mpox vaccine started | Challenges |
|---|---|---|---|
| Rwanda | Surveillance, contact tracing, public health campaigns, vaccination rollout, and establishment of a testing hub | Yes | Vaccine shortages |
| Burundi | Training healthcare workers, psychosocial support, IPC, and WASH interventions | No | High transmission rate |
| Uganda | Early detection, contact tracing, treatment units, public awareness campaigns | Yes | High CFR |
| Kenya | Public awareness campaigns, WASH initiatives, and resource mobilization | No | Transmission along trade routes |
| Tanzania | Port health services, community surveillance, public health education | No | Potential undetected cases |
| DRC | Vaccination campaigns, contact tracing, IPC strengthening, and enhanced surveillance | Yes | Widespread cases |
| South Sudan | Contact tracing, training of laboratory staff, strengthened surveillance at entry points, IPC, and WASH reinforcement | No | Limited laboratory capacity, fragile health system |
| Somalia | Health‐worker training, public awareness campaigns, border vigilance, and surveillance | No | Weak surveillance infrastructure, risk of undetected introduction |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · Viral Infections and Outbreaks Research · Data-Driven Disease Surveillance
Introduction
1
Mpox, formerly known as monkeypox, is a zoonotic disease caused by the monkeypox virus (MPXV), which emerged as a global health threat due to the high transmission and challenges to the health systems [1, 2]. Mpox is a double‐stranded DNA virus that belongs to the Poxviridae family of the genus Orthopoxvirus and has two different clades, Clade I historically associated with the Congo Basin and Clade II associated with West Africa outbreaks [3]. Mpox virus was initially identified in captive monkeys in Denmark in 1959, and the first human case was identified in 1970 from a male in the Democratic Republic of the Congo (DRC) [4]. By 1980, 59 cases were reported in DRC [5], and in the following decades, Mpox sporadic outbreaks heavily affected Central and West Africa, especially in DRC, Nigeria, Cameroon, and the Central African Republic [6]. In 2017–2018, Nigeria recorded the largest number of cases, over 276 confirmed cases, with human‐to‐human transmission [7]. In 2022, Mpox outbreak marked a significant shift in the disease's epidemiology. It showed the change from sporadic cases, primarily linked to animal contact, to widespread human‐to‐human transmission [8, 9].
On August 13, 2024, the Africa Centre for Disease Control and Prevention declared Mpox as a Public Health Emergency of Continental Security (PHECS) [10, 11]. The following day, the World Health Organization (WHO) declared Mpox a Public Health Emergency of International Concern (PHEIC) in response to the high number of cases in DRC and the ongoing regional spread [12, 13, 14]. This declaration highlighted the urgent need for increased surveillance, vaccination efforts, and international collaboration to contain the outbreak [15].
The epicenter of the 2024 Mpox outbreak was the DRC, which is a member of the East African Community (EAC), accounting for 96% of new cases and deaths [16]. The EAC is currently a global Mpox hotspot as partner states were directly affected by Mpox outbreak [17]. The EAC is composed of eight countries, namely, (i) the Republic of Burundi, (ii) the DRC, (iii) the Republic of Kenya, (iv) the Republic of Rwanda, (v) the Federal Republic of Somalia, (vi) the Republic of South Sudan, (vii) the Republic of Uganda, and (viii) the United Republic of Tanzania [18]. Mpox outbreak in the DRC began in April 2024 and rapidly spread to neighboring countries (Burundi, Uganda, Kenya, and Rwanda), which had not previously experienced Mpox. In addition, a travel‐associated clade Ib case was reported in Sweden in August 2024 [11]. Several countries beyond the EAC region have confirmed Mpox cases linked to EAC countries [19]. In Southern Africa, Zambia and Zimbabwe reported travel‐related cases [20]. In Europe, a travel‐associated Clade Ib case was reported in Sweden in August 2024 [11]. Moreover, Germany reported seven cases (three linked to EAC), whereas the United Kingdom and Northern Ireland both confirmed six cases, all linked to EAC. In Asia, China recorded seven cases with one linked to DRC, and Thailand confirmed one case linked to EAC. In North America, the USA confirmed four cases and Canada one case associated with EAC countries [19]. These cases around the world show the importance of coordinated global surveillance and response efforts.
Most countries in the EAC have been reporting Mpox cases, with the DRC, Burundi, and Uganda reporting the highest numbers. In response, the EAC implemented strategies to control Mpox, focusing on monitoring cross‐border movements and addressing health challenges arising from integrated public health frameworks [17, 21]. However, systemic gaps in healthcare infrastructure, different levels of disease surveillance capacity, and sociopolitical instability in some EAC member states complicated the region's response [11, 22, 23]. Furthermore, the stigma associated with Mpox, misinformation, and limited vaccine accessibility presented further barriers to effective containment [24]. Addressing these challenges requires a comprehensive approach that includes enhancing healthcare infrastructure, improving public awareness to prevent stigma and misinformation, and ensuring equitable access to vaccines across all member states. Therefore, this review aimed to provide a comprehensive analysis of Mpox outbreak in the EAC region, which has been ongoing since 2024, by focusing on epidemiological trends, containment measures, and challenges. By reflecting on the successes and challenges experienced, this review seeks to provide actionable insights for strengthening future outbreak preparedness and adopting regional resilience to emerging infectious diseases.
Status and Containment Measures of Mpox in the EAC Member States
2
Mpox continues to affect most EAC countries, with considerable variations in transmission patterns, case severity, and the populations at risk (Table 1). As of July 2025, DRC remains the most affected country, contributing the largest proportion of regional Mpox cases (28,165 cases and 69 deaths), with widespread transmission across nearly all provinces [25, 26]. Uganda and Burundi also experienced sustained community transmission, whereas Kenya had a disproportionately high case fatality rate (CFR) when compared to reported cases. Rwanda, Tanzania, and South Sudan documented relatively low numbers of confirmed cases, with no Mpox‐related deaths. Somalia remains the only EAC country that has not reported any Mpox case, possibly due to limited laboratory testing/surveillance system or limited introduction of the virus from neighboring countries. Differences of Mpox burden in EAC countries could be explained by multiple factors, including proximity to high‐burden countries, the level of implementation of testing and control measures, and the demographic characteristics of exposed populations.
Status of Mpox in the DRC
2.1
Since April 2024, the DRC has experienced a significant Mpox outbreak, characterized by continual human‐to‐human transmission and the circulation of multiple viral subclades in the community [27]. The outbreak started with Mpox Clade Ib in South Kivu province which was rapidly transmitted to North Kivu and nearly all regions of the country, affecting 22 of 26 provinces [28, 29]. Mpox outbreak was complicated by co‐circulation of both subclades Ia and Ib, along with multiple introductions in densely populated areas [30]. Moreover, genetic alteration of Clade Ib increased transmissibility, mostly linked to sexual transmission networks and significant spread within the community [31].
The most affected provinces are Equateur, North Kivu, Sankuru, South Kivu, South‐Ubangi, and Tshopo [29]. The main risk factors included sexual networks involving men who have sex with men (MSM) and sex workers [32, 33, 34]. However, nonsexual exposures, such as hunting, fishing, agriculture, wildlife trade, poverty, and contact with an infected individual, have been previously cited [35, 36].
Containment measures, including vaccination campaigns, contact tracing, enhanced surveillance, case isolation, and infection prevention and control (IPC) strategies, were adopted [37]. Indeed, the Modified Vaccinia Ankara‐Bavarian Nordic (MVA‐BN) vaccine has been deployed, and a vaccination model proved that immunizing 80% of <15 children in the DRC could reduce illness, viral circulation, and mortality [38]. Overall vaccine acceptance in the DRC was 61.0%, with higher willingness reported among healthcare workers and individuals from endemic regions, underscoring the need to boost community vaccination awareness campaigns [39]. The country has administered over 73% of all Mpox vaccines delivered in Africa [40]. The screening capacity was constrained by shortage of medical supplies and limited staffing, resulting in increased turnaround time (TAT) [41]. The TAT was later reduced from 10 days to 24–48 h [41, 42] due to improved supply of sample collection kits, personal protective equipment, and decentralization of laboratory capacity.
Status of Mpox in Burundi
2.2
Burundi experienced a rapid geographical spread of Clade Ib MPXV [40] reaching nearly all health districts by early 2025, with the highest transmission in Bujumbura and Gitega [43, 44]. The Clade Ib MPXV reported in Burundi had been circulating in South Kivu [45], suggesting cross‐border movement of people in the region. Although the national CFR remained low, Mpox was more prevalent among children under 15, highlighting distinct demographic vulnerability [28].
Burundi's response initiatives included a large‐scale IPC training, providing psychosocial support to affected individuals, expansion of WASH services in schools, establishment of isolation centers, and community sensitization [46]. The government, in collaboration with Africa CDC, initiated plans to introduce vaccination targeting high‐risk groups, such as health workers, sex workers, MSM, eco‐guards/hunters, and other high‐risk groups [47]. Such measures enabled Burundi to control Mpox through a strong system resulting in a low CFR.
Mpox Status in Uganda
2.3
Uganda reported geographical spread, particularly with high transmission in Kampala and Wakiso [36]. After a few days of confirming the first two cases, the outbreak was declared with 41 confirmed cases, revealing a high transmission rate in Uganda [48, 49]. The outbreak was exclusively driven by Clade Ib MPXV, mostly affecting young adults (18–29 years) and males. The outbreak continued to spread rapidly and widely, affecting 82% of the districts, with a constant resurgence in high‐burden districts [50, 51]. Similar to other areas affected by Clade Ib, immunocompromised individuals were greatly affected, and 47.9% of Mpox‐related deaths occurred in HIV‐coinfected people [50].
The Ugandan Ministry of Health implemented extensive containment measures, including early detection, contact tracing to promptly identify and isolate cases, public health awareness campaigns, and the establishment of treatment units in affected districts [52, 53]. Early in the outbreak, the introduction of Mpox cases into schools led to joint efforts of the Ministry of Health and the Ministry of Education to enhance contact tracing and develop disease control protocols specific to schools [48, 49]. Within communities, outbreak response was reinforced by training field responders, building capacity of laboratories, and enforcing electronic surveillance systems, all of which promoted early detection and treatment [52]. Vaccination efforts began in the capital city of Uganda (Kampala), prioritizing high‐risk populations and healthcare workers, and it was supported by vaccine donations from Africa CDC and the European Commission [54].
Status of Mpox in Rwanda
2.4
In Rwanda, the outbreak began in July 2024, with early cases linked to travel history from the DRC before the onset of symptoms [46]. Transmission remained comparatively limited, with no recorded deaths. Clade Ib MPXV was identified as the circulating strain in Rwanda, consistent with regional trends [50, 55]. Rwanda, through the Rwanda Biomedical Centre (RBC), put efforts in advanced diagnostic capacity by implementing genomic sequencing and bioinformatics analysis as key measures in surveillance of infectious and outbreak diseases [24].
Rwanda's response emphasizes strong diagnostic capacity, including polymerase chain reaction (PCR) testing for all suspected cases, genomic sequencing, and decentralized testing hubs. Confirmation of MPXV infection was based on nucleic acid amplification testing (NAAT), and positive samples were sequenced [56]. Three testing hubs were established in different provinces to promote proximity of testing services to the high‐risk sites. Additionally, surveillance was strongly enhanced through contact tracing and regular follow‐up of high‐risk individuals [50, 55]. A few months after the outbreak declaration, Rwanda launched a vaccination campaign against Mpox in September 2024, targeting health workers, cross‐border business operators, hospitality workers, truck drivers, and sex workers [57].
Mpox Status in Kenya
2.5
Kenya reported Mpox outbreak in July 2024, with cases concentrated in coastal and border counties, such as Nakuru, Mombasa, and Busia [58, 59]. Most of the confirmed cases were reported from truck drivers or their close contacts, and 63% of all cases were mostly linked to sexual transmission [60, 61]. Sequencing of Clade Ib Mpox isolated from the index Kenyan case, who was a truck driver with travel history to Uganda, revealed that the virus was linked to the regional outbreak [60, 61]. Although overall caseload remains lower than in neighboring countries, the CFR is relatively high in Kenya, suggesting potential delays in seeking care or severity among affected populations. Clade Ib is the circulating strain in Kenya, and only human‐to‐human transmission has been recorded [60, 61].
Response activities included public awareness campaigns to educate communities on Mpox prevention, WASH interventions, and multisectoral resource mobilization. Most of the containment measures were directed to high‐risk counties, where case detection was enhanced through deployment of rapid response teams and large‐scale travelers screening at entry points [62]. However, response was initially hindered by low public risk perception and inadequate resources, which were mitigated through community awareness campaigns and supplies for infection prevention in congregated settings [63]. Nonetheless, the number of cases are steadily increasing, undermining the effectiveness of control measures, probably due to the high cross‐border mobility and failure to identify all high‐risk individuals. All Mpox‐related deaths in Kenya were recorded among HIV‐coinfected individuals, highlighting that PLHIV constitute a vulnerable group needing much care to contain the outbreak.
Status of Mpox in the United Republic of Tanzania
2.6
Tanzania confirmed its first Mpox cases in March 2025, involving individuals in Dar es Salaam [36, 64, 65, 66]. Similar to Kenya, Mpox was introduced by a truck driver, leading to border screening and case investigation. However, community transmission persisted [25, 64, 65]. The dominance of Clade Ib Mpox, coupled with its high transmissibility, contributed to the widespread of the virus in different countries; however, no deaths have been reported so far [25].
Tanzania adopted various containment measures including strengthened port health services, border screening, community surveillance, health education campaigns, and prioritization of vaccination for vulnerable populations such as PLHIV [67, 68]. The country also benefited from the EAC initiative of deploying mobile laboratories for strengthening surveillance at the borders to prevent the spread of infection and conducting genomic surveillance among the EAC members [17].
Status of Mpox in South Sudan
2.7
South Sudan confirmed its first Mpox case in February 2025, mostly travel‐related, with no deaths to date [25, 36]. This person was a Ugandan national living in Juba and was confirmed by the National Public Health Laboratory (NPHL) [69]. Clade Ib is the circulating strain, consistent with reports in other countries [69].
The Ministry of Health coordinated responses, including contact tracing, strengthened surveillance at major entry points, laboratory capacity building, and the provision of IPC and WASH resources at the community and facility levels [17, 70].
Status of Mpox in Somalia
2.8
Somalia has not yet reported any confirmed Mpox cases as of November 2025 [71]. This may be linked to a weakened health system and limited testing capacity following more than 25 years of civil war and instability. However, the country remains vigilant at its borders and is strengthening its health infrastructure, to migitage the risk of Mpox virus spread from neighboring regions [71]. Somalia, like other countries in EAC, where healthcare infrastructure and disease surveillance are not advanced, requires greater efforts to address and prepare for outbreaks like Mpox [72, 73].
The country is strengthening preparedness through training of healthcare workers, laboratory scientists, and epidemiologists who will help in the implementation of managing outbreaks in Somalia [71]. Additionally, the Ministry of Health launched an awareness campaign to educate the public about Mpox symptoms, prevention, and transmission.
Table 2 summarizes Mpox containment measures in the EAC that include enhanced surveillance, contact tracing, public awareness campaigns, and vaccination efforts. Mobile laboratories support high‐risk areas, and regional collaboration strengthens cross‐border surveillance. Challenges such as limited vaccine access and misinformation remain significant barriers.
Comparative Analysis of Epidemiological Differences Across EAC Countries
3
Epidemiological outcomes across EAC member states show marked variation, driven by differences in surveillance systems, demographic profiles, healthcare access, and local transmission dynamics. Apart from DRC, which had an ongoing of Mpox outbreak, Burundi, Kenya, Rwanda, and Uganda all reported their first cases in 2024. Contrarily, Tanzania and South Sudan have limited documentation on how the Mpox outbreak was managed.
In addition, apart from DRC known to be the epicenter of the Mpox outbreak, Kenya reported a higher CFR (1.78%) compared to 0.02% for Burundi, which may be influenced by several factors. Kenya's affected population includes more adults and mobile populations along major trade routes [60, 61], which may contribute to delayed care‐seeking or higher prevalence of comorbidities. In contrast, Burundi reported that Mpox was predominant in a younger population (children under 15) who generally presented with milder disease. So far, no deaths have been reported in Rwanda, Tanzania, and South Sudan. It is important to mention that CFR estimates depend strongly on case detection and death reporting systems, which vary widely among EAC countries.
Differences in surveillance and diagnostic capacity also contribute to heterogeneous outcomes [24]. For example, Rwanda and Uganda, through the EAC, benefited from strengthened laboratory and surveillance networks, including genomic sequencing and decentralized testing hubs [17]. Furthermore, fragile health systems and conflict‐related disruptions in the Eastern Part of the DRC, South Sudan, and Somalia may limit access to timely care and complicate diagnosis. Lastly, the degree of urbanization and mobility patterns, including high‐traffic transport corridors between Kenya, Uganda, and Tanzania, shape exposure risk and influence the outbreak severity. These variations highlight the need for tailored, country‐specific response strategies while reinforcing regional coordination across the EAC.
Challenges and Future Directions
4
Despite ongoing response efforts, several challenges continue to hinder effective Mpox control in East Africa and other regions. One major barrier is unequal vaccine access, which has led to increased cases and deaths in countries with limited supply or delayed vaccination rollouts [74]. This inequity reflects broader systemic gaps in global distribution of health resource [75]. Vaccine disparities represent not only logistical failures but also ethical shortcomings in justice and global solidarity, where populations in low‐resource settings are consistently last to receive life‐saving interventions [76].
Misinformation regarding Mpox is also increasing, especially on social media platforms. On X (formerly Twitter), large volumes of misleading or false information circulate about the transmission of the virus, its severity, and origins [77, 78, 79]. Such misinformation not only undermines public awareness but also weakens the trust in different health interventions and institutional strategies to combat Mpox in different countries. This critical challenge needs much attention to ensure effective disease control in the community [24]. Transparent communication and trust‐building are essential pillars of outbreak response, and failure to address misinformation threatens both public accountability and community resilience [76].
Mpox‐related stigma remains another major challenge globally. Stigma contributes to delayed healthcare seeking, nondisclosure of the disease, discrimination in some health settings, and affects mental health [80, 81]. In Burundi, a motorcyclist recovering from Mpox experienced severe stigma resulting in social isolation, loss of livelihood, and housing instability due to visible scars [82]. Political instability affects the mitigation strategies to control Mpox in the region [83]. In settings such as the DRC, South Sudan, and Somalia, insecurity disrupts humanitarian operations, limits access to healthcare, and complicates disease surveillance, laboratory diagnostics, and treatment [11].
Infrastructure and laboratory capacity remain critical gaps across many EAC countries. Limited availability of genomic sequencing platforms, testing kits, and bioinformatics expertise delays identification of circulating clades in the region and reduces the implementation of public health interventions [11]. Although Africa CDC, WHO, and other partners pledged to increase vaccine availability across the continent, logistic challenges including cold chain requirements and transport constraints, continue to impede equitable distribution [84].
To strengthen future Mpox preparedness and response, EAC member states must combine operational improvements with an ethically grounded framework that emphasizes justice, solidarity, and respect for rights. By improving vaccine equity, combating misinformation through transparent communication, addressing stigma, expanding laboratory capacity, and enhancing cross‐border collaboration, the region can significantly improve its resilience and ensure a more equitable and effective response to emerging infectious diseases.
Conclusion
5
The Mpox outbreak surged in 2024 and remains ongoing in the EAC region, with the DRC and Burundi being the most affected countries. Major containment measures were implemented, including monitoring cross‐border movement and improving testing capacity and vaccination coverage. This outbreak serves as another wake‐up call for the EAC to strengthen public health responses to recurrent emerging infectious diseases. Although significant progress was made in containing the outbreak, addressing systemic gaps in healthcare infrastructure and resource distribution remains essential. The EAC must prioritize investments in health systems, advance international partnerships, and influence community‐driven approaches to build resilience and ensure equitable health outcomes across the region.
Author Contributions
Reuben Sindayiheba and Noel Gahamanyi contributed to the design of the work, data collection, analysis, and drafting of the manuscript. Edouard Ntagwabira, Emmanuel Kabalisa, Gashegu Misbah, Isabelle Mukagatare, Leon Mutesa, and Claude Mambo Muvunyi significantly revised the manuscript and supervised the work. All authors read and approved the final version of the manuscript.
Funding
The authors have nothing to report.
Disclosure
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1O. Mitjà , A. Alemany , M. Marks , et al., “Mpox in People With Advanced HIV Infection: A Global Case Series,” Lancet 401, no. 10380 (2023): 939–949, 10.1016/S 0140-6736(23)00273-8.36828001 · doi ↗ · pubmed ↗
- 2D. B. Olawade , O. Z. Wada , S. C. Fidelis , et al., “Strengthening Africa's Response to Mpox (Monkeypox): Insights From Historical Outbreaks and the Present Global Spread,” Science in One Health 3 (2024): 100085, 10.1016/j.soh.2024.100085.39583938 PMC 11582772 · doi ↗ · pubmed ↗
- 3A. Karagoz , H. Tombuloglu , M. Alsaeed , et al., “Monkeypox (Mpox) Virus: Classification, Origin, Transmission, Genome Organization, Antiviral Drugs, and Molecular Diagnosis,” Journal of Infection and Public Health 16 (2023): 531–541, 10.1016/j.jiph.2023.02.003.36801633 PMC 9908738 · doi ↗ · pubmed ↗
- 4C. L. J. Ugwu , N. L. Bragazzi , J. Wu , et al., “Risk Factors Associated With Human Mpox Infection: A Systematic Review and Meta‐Analysis,” BMJ Global Health 10, no. 2 (2025): e 016937, 10.1136/bmjgh-2024-016937.PMC 1179541339900427 · doi ↗ · pubmed ↗
- 5S. Hasan and S. Saeed , “Monkeypox Disease: An Emerging Public Health Concern in the Shadow of COVID‐19 Pandemic: An Update,” Tropical Medicine and Infectious Disease 7 (2022): 283, 10.3390/tropicalmed 7100283.36288024 PMC 9607171 · doi ↗ · pubmed ↗
- 6E. M. Bunge , B. Hoet , L. Chen , et al., “The Changing Epidemiology of Human Monkeypox—A Potential Threat? A Systematic Review,” PLOS Neglected Tropical Diseases 16, no. 2 (2022): e 0010141, 10.1371/journal.pntd.0010141.35148313 PMC 8870502 · doi ↗ · pubmed ↗
- 7A. Yinka‐Ogunleye , O. Aruna , M. Dalhat , et al., “Outbreak of Human Monkeypox in Nigeria in 2017–18: A Clinical and Epidemiological Report,” Lancet Infectious Diseases 19, no. 8 (2019): 872–879, 10.1016/S 1473-3099(19)30294-4.31285143 PMC 9628943 · doi ↗ · pubmed ↗
- 8WHO , Multi‐Country Monkeypox Outbreak in Non‐Endemic Countries (WHO, 2022).