Pulsed dye versus neodymium-doped yttrium aluminum garnet lasers for refractory warts: a systematic review and meta-analysis
Joon-Goon Kim

TL;DR
This study compares two laser treatments for stubborn warts and finds they work equally well, but one causes fewer bleeding issues.
Contribution
The study provides a systematic review and meta-analysis comparing PDL and Nd:YAG lasers for refractory warts, highlighting their efficacy and safety differences.
Findings
PDLs and Nd:YAG lasers showed similar complete clearance rates for refractory warts.
PDLs had significantly fewer hemorrhagic complications compared to Nd:YAG lasers.
Single-arm studies showed wide variability in clearance rates for both laser types.
Abstract
Refractory cutaneous warts often persist despite conventional treatments. Pulsed dye lasers (PDLs) and long-pulsed neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers are commonly used in clinical practice. However, comparative data on refractory cases remain limited. Following PRISMA 2020 guidelines, PubMed, Embase, Scopus, and Cochrane Library were searched through October 11, 2025, for studies evaluating PDL or Nd:YAG treatment for refractory warts. Head‑to‑head studies were meta-analyzed using Inverse Variance fixed‑effect odds ratios (ORs), whereas single‑arm evidence was summarized narratively following the SWiM guidelines. The primary outcome was complete clearance, with hemorrhagic complications as the key safety outcome. Fifteen studies met the inclusion criteria: three head‑to‑head (n=224; 115 PDLs and 109 Nd:YAG lasers) and 12 single‑arm series. Complete clearance was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
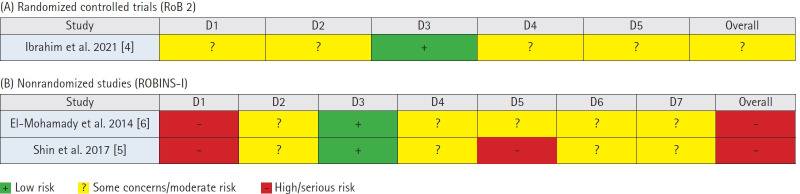 Figure 1
Figure 1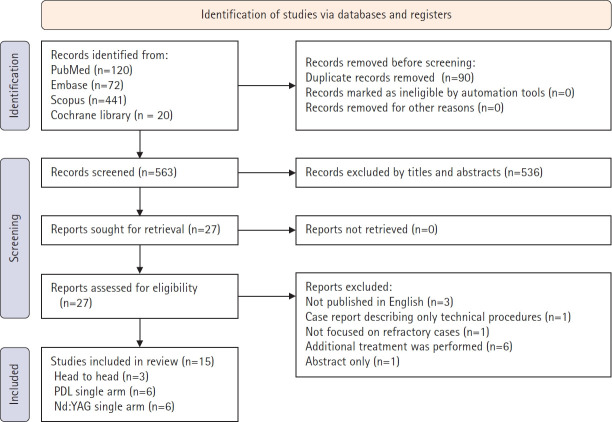 Figure 2
Figure 2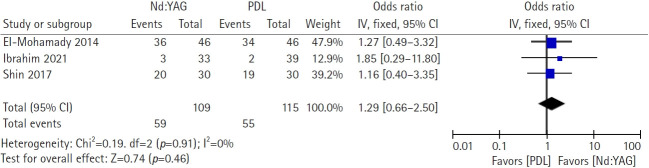 Figure 3
Figure 3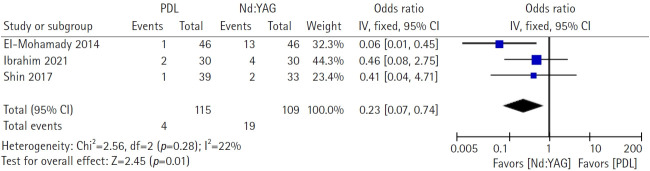 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Gynecological conditions and treatments · Ectopic Pregnancy Diagnosis and Management
Introduction
Cutaneous warts (verrucae) are benign epithelial proliferations caused by infection of keratinocytes with human papillomavirus (HPV), with an estimated prevalence of 5% to 30% in children and young adults [1,2]. Common warts account for approximately 70% of cases, whereas plantar and plane warts account for 24% and 3.5%, respectively [3]. Although many warts undergo spontaneous resolution within 1 to 2 years in children, clearance in adults can be significantly slower, and persistence for 5 to 10 years is common. Traditional first-line treatments, including salicylic acid treatment and cryotherapy, frequently fail to achieve complete remission, particularly in recalcitrant cases [1].
Refractory or recalcitrant warts are defined as lesions that persist despite multiple attempts at conventional treatment, presenting a significant therapeutic challenge in dermatological practice. These resistant warts are often associated with specific HPV genotypes, particularly HPV types 2, 27, and 57, and tend to occur at anatomically challenging sites, such as periungual and plantar locations [2]. Therefore, the management of refractory warts requires alternative treatment modalities beyond the standard approaches.
Over the past few decades, laser therapy has emerged as a promising treatment option for recalcitrant warts. Among the various laser modalities, non-ablative lasers, including pulsed dye lasers (PDLs) and neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers, have demonstrated favorable efficacy in multiple studies. PDLs operate at wavelengths of 585 to 595 nm, targeting hemoglobin within dilated capillaries that supply warts, thereby inducing ischemic necrosis. Nd:YAG lasers, operating at a wavelength of 1,064 nm, offer deeper tissue penetration and similar vascular-targeting mechanisms, targeting hemoglobin to coagulate and destroy dermal blood vessels in warts. This longer wavelength allows deeper penetration into the hyperkeratotic epidermis than PDLs. Histologically, it causes dermo-epidermal junction separation, epidermal necrosis, and capillary coagulation. A systematic review of 35 studies involving 2,149 patients reported clearance rates ranging from 47% to 100% for PDL and 46% to 100% for Nd:YAG laser treatment of nongenital warts [3].
Despite growing evidence supporting the efficacy of both PDLs and Nd:YAG lasers in wart treatment, direct comparative studies between these two non-ablative modalities remain limited, particularly in the context of refractory warts. Therefore, this systematic review was conducted with a particular focus on refractory cutaneous warts to (1) synthesize head‑to‑head comparisons of PDL versus Nd:YAG laser therapy regarding complete clearance and key safety outcomes, and (2) contextualize the performance of each modality from single‑arm studies without making indirect between‑laser comparisons. This approach aims to align clinical decision-making with the best available comparative evidence while transparently summarizing single-arm data for real-world applicability.
Methods
Ethics statement: Not applicable.
1. Data sources and search strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (the protocol was prospectively designed and not registered). The narrative syntheses of single-arm studies adhered to the Synthesis Without Meta-analysis (SWiM) guidelines. PubMed, Embase, Scopus, and the Cochrane Library were searched on October 11, 2025, using the following terms: (wart OR verruca) AND (dye OR PDL OR neodymium‑doped yttrium‑aluminum‑garnet OR YAG) AND (recalcitrant OR resistant OR refractory OR persistent OR recurrent OR relapse). No restrictions were imposed on the dates. Full non-English texts were excluded from eligibility.
2. Study selection
Studies were included if they met the following criteria: (1) patients with refractory, recalcitrant, or treatment-resistant warts (defined as failure of at least one prior conventional therapy); (2) treatment with a PDL (585–595 nm) or Nd:YAG laser (1,064 nm); (3) reporting of complete clearance rates; and (4) prospective or retrospective cohort studies, comparative trials, or case series with ≥10 patients. The exclusion criteria were as follows: (1) case reports with <10 patients focusing solely on technique description, (2) studies combining laser with concurrent adjuvant therapies, (3) studies without a clear definition of refractory status, (4) duplicate publications, (5) conference abstracts without full text, and (6) studies not published in English.
The study selection was performed in two phases. First, titles and abstracts were screened against the eligibility criteria. Subsequently, the full texts of potentially eligible studies were retrieved and assessed for final inclusion. Studies were categorized as: (1) head-to-head comparative studies eligible for meta-analysis or (2) single-arm studies eligible for descriptive synthesis only. Any uncertainty regarding eligibility or categorization was resolved through reexamination of the original inclusion criteria and consultation with a senior dermatologist when necessary. The study selection process was documented using a PRISMA flow diagram.
3. Data extraction and quality assessment
Data were extracted using standardized forms to capture study characteristics (design, setting, and sample size), patient numbers, wart characteristics (location and type), laser parameters (wavelength, fluence, spot size, pulse duration, and number of sessions for clearance), and outcomes (complete clearance, defined as 100% lesion resolution, and adverse events).
The risk of bias was assessed using a qualitative domain-based approach. For head-to-head comparative studies, RoB 2 (for randomized studies) and ROBINS‑I (for nonrandomized studies) tools were used, and results were summarized descriptively (traffic‑light plot, Fig. 1). For single-arm studies, descriptive quality assessment focused on selection, performance, detection, attrition, and reporting biases. Study quality was rated on a 5-point scale based on methodological rigor.
4. Data synthesis and analysis
1) Meta-analysis of head-to-head comparative studies
A quantitative meta-analysis was conducted on the three head-to-head comparative studies that directly compared PDL with Nd:YAG laser treatments. Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated as primary effect measures for efficacy and safety outcomes. ORs were selected because they are appropriate for binary outcomes and allow for a clear interpretation of relative treatment effects.
Fixed-effects models based on the Inverse Variance method were used for all meta-analyses.
2) Assessment of statistical heterogeneity
Statistical heterogeneity across head-to-head comparative studies was assessed using the I² statistic, with values interpreted according to standard thresholds: I²<25%, low heterogeneity; 25%≤I²≤75%, moderate heterogeneity; and I²>75%, high heterogeneity.
3) Descriptive synthesis of single-arm studies
Single-arm studies (i.e., those evaluating PDL monotherapy or Nd:YAG monotherapy without direct comparison groups) were qualitatively and descriptively summarized. For these studies, the range of complete clearance rates observed across the PDL and Nd:YAG studies was calculated and reported separately.
Quantitative pooling or statistical comparisons of single-arm PDL and single-arm Nd:YAG studies were not performed because of the high risk of confounding inherent in such indirect comparisons. Differences in patient populations, wart characteristics, treatment protocols, outcome assessment methods, and follow-up durations across single-arm studies precluded valid statistical inferences regarding comparative efficacy.
The single-arm studies were included in the systematic review to provide contextual evidence for each laser modality and to describe the range of treatment responses reported in the literature. However, conclusions regarding comparative efficacy and safety were derived exclusively from the head-to-head comparative studies included in the meta-analysis.
Publication bias was not assessed using funnel plots because the number of eligible studies was insufficient (<10). All analyses were conducted using RevMan 5.4 software (Cochrane Collaboration, Copenhagen, Denmark). Statistical significance was set at p<0.05.
Results
1. Literature search and selection of studies
The database search identified 653 records (PubMed, 120; Embase, 72; Scopus, 441; and Cochrane Library, 20). After removing 90 duplicate articles, 563 titles and abstracts were screened, of which 536 were excluded. Twenty-seven full texts were assessed for eligibility, and all were retrieved. Twelve reports were excluded for predefined reasons (non‑English, case reports describing only technical procedures, absence of refractory cases, concurrent additional treatments, or abstract‑only reports). Ultimately, 15 studies were included in the qualitative synthesis: three head‑to‑head comparisons of PDLs and Nd:YAG lasers, six single‑arm PDL studies, and six single‑arm Nd:YAG laser studies (Fig. 2).
2. Study characteristics and quality
Across all included reports, participants had refractory (recalcitrant/resistant) warts following the failure of at least one prior therapy. Interventions employed a PDL (585–595 nm) or Nd:YAG laser (1,064 nm) according to each study protocol. The study designs were predominantly nonrandomized prospective or retrospective cohorts. Outcome definitions were consistent, with complete clearance defined as 100% lesion resolution.
3. Comparative efficacy of pulsed dye lasers versus Nd:YAG lasers (complete clearance)
Three head‑to‑head studies (Ibrahim et al. [4] in 2021, Shin et al. [5] in 2017, and El‑Mohamady et al. [6] in 2014) comprising 224 participants were pooled using a fixed‑effect model (Nd:YAG, n=109; PDL, n=115). Complete clearance occurred in 59 of 109 participants in the Nd:YAG arms and 55 of 115 in the PDL arms. The meta‑analysis revealed no significant difference between PDL and Nd:YAG in complete clearance (OR, 1.29; 95% CI, 0.66–2.50; Z=0.74; p=0.46). Statistical heterogeneity was negligible (χ^2^=0.19, degrees of freedom [df]=2, p=0.91, I²=0%), supporting the use of a fixed‑effect model. These findings indicated a broadly comparable efficacy for complete wart clearance between the two laser modalities in direct comparisons (Fig. 3).
4. Adverse events (hematoma/hemorrhagic bullae)
Hemorrhagic complications were analyzed across the same three comparative studies. These events were less frequent with PDLs (4/115) than with Nd:YAG lasers (19/109). Pooled analysis using a fixed‑effect model demonstrated a statistically significant advantage for PDLs (OR, 0.23; 95% CI, 0.07–0.74; Z=2.45; p=0.01). Heterogeneity was low to moderate (χ^2^=2.56, df=2, p=0.28, I²=22%). Thus, although the clearance efficacy was similar, PDL use was associated with a significantly lower risk of hemorrhagic adverse events than Nd:YAG laser use in head-to-head studies (Fig. 4).
5. Pulsed dye laser single-arm outcomes
Six single-arm PDL studies indicated complete clearance rates ranging from 5.1% to 89.0%. Given the between-study variability in patient selection, lesion characteristics, and treatment parameters, pooled estimates were not generated. The outcomes are summarized in Table 1. Collectively, these series confirmed that PDLs can achieve complete clearance in a meaningful proportion of recalcitrant cases, albeit with substantial variability across settings. When adverse events were reported, hemorrhagic complications were uncommon, which was consistent with the comparative safety analysis. Detailed study‑level characteristics and outcome proportions are summarized in Table 1.
6. Nd:YAG laser single-arm outcomes
Six single-arm Nd:YAG studies indicated complete clearance rates ranging from 9.1% to 100%. As with PDLs, heterogeneity in inclusion criteria and laser parameters precluded meta‑analytic pooling; therefore, the results were synthesized narratively. These data indicate that Nd:YAG lasers can produce high clearance in selected cohorts, including reports of complete response in all treated lesions, but with considerable dispersion across studies. Reporting of adverse events varied, and events of bleeding or hemorrhagic bullae were documented in some series, aligning with the higher odds observed in the comparative analysis. The complete study-level data are presented in Table 2.
Discussion
Across three head‑to‑head studies (n=224), complete‑clearance efficacy did not differ between PDLs and Nd:YAG lasers (OR, 1.29; 95% CI, 0.66–2.50; I²=0%). In contrast, hemorrhagic complications (hematoma/hemorrhagic bullae) occurred less frequently with PDLs (OR, 0.23; 95% CI, 0.07–0.74; I²=22%) [4–6]. Absolute event rates were approximately 3.5% for PDLs (4/115) versus 17.4% for Nd:YAG lasers (19/109), yielding an absolute risk difference of approximately 14% and an approximate number needed to harm of 7 when choosing Nd:YAG lasers over PDLs. Clinically, these results convey a pragmatic message that selection should be guided by safety and context rather than by expected clearance.
The strong hemoglobin absorption and short pulse durations of PDLs focus energy within superficial plexuses, whereas 1,064 nm Nd:YAG lasers penetrate more deeply with broader thermal effects [7]. Classic PDL histology demonstrates intravascular erythrocyte aggregation and thrombus formation, which is direct evidence for selective photothermolysis in vivo [8]. These differences offer a biologically plausible explanation for the lower hemorrhagic reactogenicity observed with PDLs in the direct comparison.
The broader laser literature has confirmed that both modalities are effective against warts [3]. Beyond laser‑versus‑laser comparisons, Nd:YAG lasers have demonstrated superiority to cryotherapy in a randomized controlled trial (RCT), underscoring the clinical efficacy of vascular‑targeted lasers [2]. Single-arm Nd:YAG series have demonstrated a wide range of outcomes (approximately 9%–100%), with higher‑fluence protocols frequently associated with hemorrhagic bullae and procedural pain [9-14]. In contrast, single‑arm PDL cohorts—especially those employing careful paring, targeting pinpoint bleeding, and using purpura as the endpoint at approximately 8 to 12 J/cm² with a 5-mm spot and short pulses—reveal consistent, often high, clearance with favorable tolerability [8,15-19]. These contextual data align with our head-to-head findings of efficacy parity, with a safety differential favoring PDLs.
For PDLs, effective parameters typically include fluence values of 6 to 15 J/cm², spot sizes of 5 to 7 mm, and pulse durations of 0.45 to 1.5 milliseconds, with purpura serving as the clinical endpoint. For Nd:YAG lasers, wider parameter ranges have been reported: fluence values of 100 to 300 J/cm², spot sizes of 2 to 7 mm, and pulse durations of 10 to 30 milliseconds. Higher fluence settings tend to improve clearance rates but increase hemorrhagic complications and procedural pain. The use of cooling devices (e.g., cold air or ice) appears to mitigate these adverse effects, although reports have been inconsistent across studies.
When cosmesis or minimizing bleeding risk is paramount (e.g., periungual or facial warts, or patient anticoagulant use), PDLs should be prioritized because of their lower hemorrhagic risk [4-6]. For thick, hyperkeratotic plantar lesions, Nd:YAG lasers remain a reasonable option, provided that the parameters (i.e., fluence, pulse duration, and spot size) and cooling are optimized, and patients are counseled regarding pain and hematoma risk [9-12]. When using an Nd:YAG laser, careful selection of anesthesia methods that consider the patient’s pain is necessary. For PDLs, standardizing paring and achieving a visible purpura endpoint improves consistency; limiting stacked pulses per zone on the sole may reduce hematoma formation while preserving ambulation [15,18].
Emerging energy-based and immunomodulatory approaches are reshaping the management strategies for recalcitrant cutaneous warts and complementing vascular-targeted lasers. In one RCT, combining Er:YAG ablation with long‑pulsed Nd:YAG treatment (1,064 nm) produced a higher single‑session complete response than Er:YAG ablation alone (48% vs. 29%), supporting a sequential “debulk‑then‑coagulate” strategy for thick, hyperkeratotic lesions [20]. In contrast, in palmoplantar disease, a comparative study found that adding 755 nm alexandrite laser to 1,064 nm Nd:YAG laser treatment did not significantly improve outcomes compared to Nd:YAG laser alone, suggesting a limited incremental value for routine dual-wavelength use [21].
The strengths of this study include a prespecified focus on refractory disease and reliance on direct comparisons for inferential conclusions, using single-arm data only for contextual interpretation. The limitations include the small number of comparative studies (k=3), mixed designs with nonrandomized components, and variability in adverse-event ascertainment.
In most settings, PDLs offer comparable clearance with fewer hemorrhagic events. Future trials should be adequately powered and stratified according to treatment site (periungual vs. plantar), lesion thickness, and histological features (e.g., parakeratosis, presence of koilocytes, vessel density, and epidermal thickness). Adopting patient-reported outcomes (e.g., pain, downtime, and successful cosmesis) and predefined safety endpoints with severity grading will further strengthen evidence for optimal laser selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sterling JC Gibbs S Haque Hussain SS Mohd Mustapa MF Handfield-Jones SE British Association of Dermatologists' guidelines for the management of cutaneous warts 2014 Br J Dermatol 201417169671210.1111/bjd.1331025273231 · doi ↗ · pubmed ↗
- 2Liu JJ Li HT Ren YY Yang F Cheng ZH Xia TB Long-pulsed neodymium-doped yttrium-aluminum-garnet laser versus cryotherapy for the treatment of cutaneous warts: a randomized controlled trial J Am Acad Dermatol 20228713283510.1016/j.jaad.2020.09.08533031838 · doi ↗ · pubmed ↗
- 3Nguyen J Korta DZ Chapman LW Kelly KM Laser treatment of nongenital verrucae: a systematic review JAMA Dermatol 201615210253410.1001/jamadermatol.2016.082627119270 · doi ↗ · pubmed ↗
- 4Ibrahim SMA Soliman M Mohamed SKA Soliman MM Pulsed dye laser versus Nd:YAG laser in the treatment of recalcitrant plantar warts: an intraindividual comparative study J Cosmet Laser Ther 202123130610.1080/14764172.2021.201684334978499 · doi ↗ · pubmed ↗
- 5Shin YS Cho EB Park EJ Kim KH Kim KJ A comparative study of pulsed dye laser versus long pulsed Nd:YAG laser treatment in recalcitrant viral warts J Dermatolog Treat 201728411610.1080/09546634.2016.125530327791434 · doi ↗ · pubmed ↗
- 6El-Mohamady Ael-S Mearag I El-Khalawany M Elshahed A Shokeir H Mahmoud A Pulsed dye laser versus Nd:YAG laser in the treatment of plantar warts: a comparative study Lasers Med Sci 2014291111610.1007/s 10103-013-1479-y 24218179 · doi ↗ · pubmed ↗
- 7Anderson RR Parrish JA Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation Science 1983220524710.1126/science.68362976836297 · doi ↗ · pubmed ↗
- 8Tan OT Hurwitz RM Stafford TJ Pulsed dye laser treatment of recalcitrant verrucae: a preliminary report Lasers Surg Med 1993131273710.1002/lsm.19001301208426521 · doi ↗ · pubmed ↗