Internal Limiting Membrane Flap Versus Conventional Peeling for Idiopathic Full Thickness Macular Holes: A Registry Analysis of 2990 Eyes
Zi Jin, Mohammad Amin Honardoost, Ee Lin Ong, Ahmad Reza Pourghaderi, Fred K. Chen, Weng Onn Chan, Prakshi Chopra, Mitchell Lee, Abhishek Sharma, Gurmit Uppal, Penelope J. Allen, Rohan W. Essex, Adrian T. Fung

TL;DR
This study compares two surgical techniques for repairing macular holes and finds that one method is better at closing the holes but does not improve vision more than the other.
Contribution
The study provides real-world evidence that ILM flap technique improves macular hole closure rates compared to conventional peeling.
Findings
ILM flap showed higher odds of hole closure compared to conventional ILM peeling.
Adjusted closure rates exceeded 95% for all hole sizes with ILM flap.
No significant difference in visual acuity outcomes between the two techniques.
Abstract
To compare the anatomical and functional outcomes of internal limiting membrane (ILM) flap and conventional ILM peeling in idiopathic full‐thickness macular holes (FTMHs). Retrospective cohort study of all eyes treated with vitrectomy and ILM peeling (ILM‐P) with or without ILM flap (ILM‐F) for primary idiopathic FTMH repair in the Australian and New Zealand Society of Retinal Specialists (ANZSRS) Registry between 2006 and 2023. Propensity score weighting and multivariable regression analysis adjusted for baseline characteristics and covariates, including surgeon grade, lens status, and follow‐up duration, were used to evaluate hole closure rate and best corrected visual acuity (BCVA) change at 3 months. Two thousand nine hundred ninety eyes of 2905 patients were included (mean age 69 ± 9 years). One Hundred Ninety‐nine eyes underwent ILM‐F and 2871 underwent ILM‐P. On weighted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
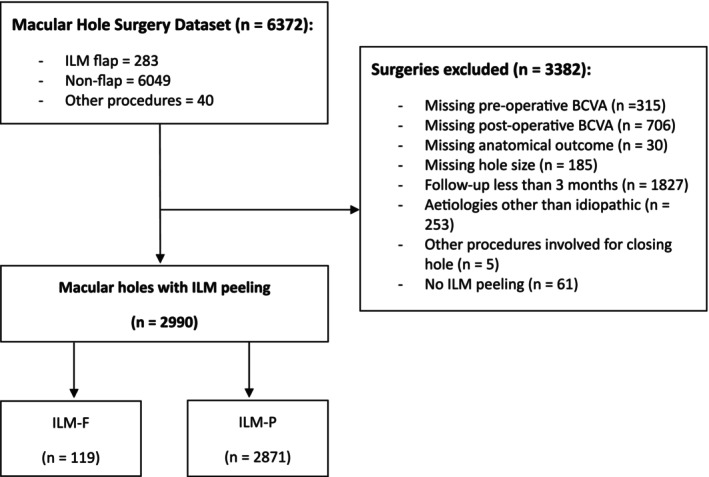 FIGURE 1
FIGURE 1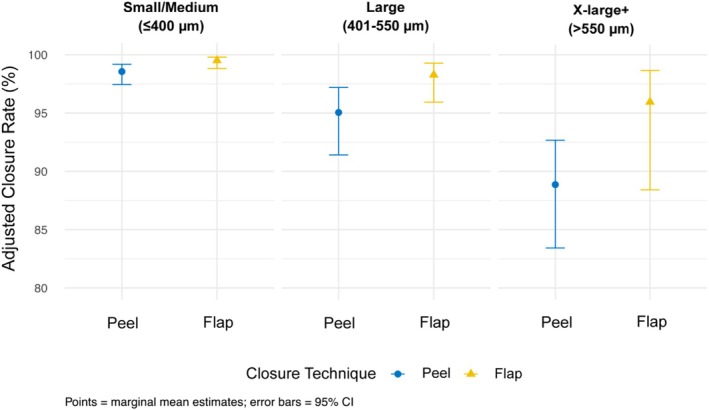 FIGURE 2
FIGURE 2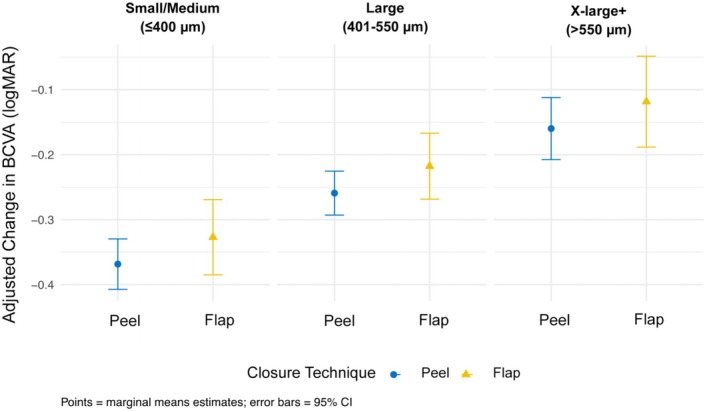 FIGURE 3
FIGURE 3| Baseline characteristic | ILM‐F | ILM‐P |
|
|---|---|---|---|
| Age, mean (SD), years | 71 (7) | 69 (9) | 0.013 |
| Female sex, | 82 (68.9%) | 1937 (67.5%) | 0.7 |
| Pre‐operative MH size, Me (Q1, Q3), μm | 521 (428650) | 296 (200408) | < 0.001 |
| Pre‐operative MHs classified into size groupings, | < 0.001 | ||
| Group 1 | |||
| Small (≤ 250 μm) | 1 (0.8%) | 1094 (38.1%) | |
| Medium (> 250 and ≤ 400 μm) | 22 (18.5%) | 1042 (36.3%) | |
| Group 2 | |||
| Large (> 400 and ≤ 550 μm) | 41 (34.5%) | 450 (15.7%) | |
| Group 3 | |||
| X‐Large (> 551 and ≤ 800 μm) | 48 (40.3%) | 230 (8.0%) | |
| XX‐Large (> 801 and ≤ 999 μm) | 6 (5.0%) | 35 (1.2%) | |
| Giant (≥ 1000 μm) | 1 (0.8%) | 20 (0.7%) | |
| Duration of hole, Me (Q1, Q3), months | 6 (4.12) | 3 (2.6) | < 0.001 |
| Pre‐operative vitreous attached to hole margins, | 49 (42.6%) | 1390 (50.4%) | 0.10 |
| Pre‐operative lens status, | 0.082 | ||
| Phakic | 85 (71.4%) | 2238 (78.2%) | |
| Aphakic/Pseudophakic | 34 (28.6%) | 625 (21.8%) | |
| Baseline BCVA, Me (Q1, Q3), logMAR | 0.9 (0.7, 1.0) | 0.7 (0.5, 0.9) | < 0.001 |
| Surgeon grade, | < 0.001 | ||
| Consultant | 90 (75.6%) | 2494 (89.1%) | |
| Fellow/Registrar | 29 (24.4%) | 304 (10.9%) |
| Variables | Univariable regression | Multivariable regression | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI |
| OR | 95% CI |
| |
| Technique (baseline = ILM‐P), ILM‐F | 0.962 | 0.394, 3.185 | > 0.9 | 2.969 | 1.075, 8.199 | 0.036 |
| Significant variables in multivariable regression | ||||||
| Pre‐operative vitreous attached to hole margins (baseline = no), Yes | 1.928 | 1.265, 2.992 | 0.003 | 2.632 | 1.382, 5.014 | 0.003 |
| Surgeon grade (baseline = consultant), Fellow/registrar | 0.423 | 0.263, 0.705 | < 0.001 | 0.451 | 0.205, 0.993 | 0.048 |
| MH size (baseline = small/medium), Large | 0.295 | 0.176, 0.499 | < 0.001 | 0.282 | 0.151, 0.525 | < 0.001 |
| MH size (baseline = small/medium), X‐Large+ | 0.139 | 0.086, 0.225 | < 0.001 | 0.117 | 0.061, 0.226 | < 0.001 |
| Non‐significant variables in multivariable regression | ||||||
| Age (in years) | 0.981 | 0.957, 1.005 | 0.14 | — | — | — |
| Gender (baseline = female), Male | 1.256 | 0.810, 2.003 | 0.3 | — | — | — |
| Pre‐operative duration of hole (in months) | 0.979 | 0.968, 0.990 | < 0.001 | 0.988 | 0.972, 1.003 | 0.12 |
| Pre‐operative lens status (baseline = phakic), Aphakic/pseudophakic | 0.966 | 0.606, 1.602 | 0.9 | — | — | — |
| Post‐operative lens status (baseline = phakic), Aphakic/pseudophakic | 1.107 | 0.733, 1.675 | 0.6 | — | — | — |
| Baseline BCVA | 0.280 | 0.161, 0.497 | < 0.001 | 0.747 | 0.286, 1.950 | 0.6 |
| Follow‐up duration (in days) | 1.001 | 1.000, 1.003 | 0.3 | — | — | — |
| Variables | Univariable regression | Multivariable regression | ||||
|---|---|---|---|---|---|---|
| Beta | 95% CI |
| Beta | 95% CI |
| |
| Technique (baseline = ILM‐P), ILM‐F | −0.025 | −0.079, 0.029 | 0.4 | 0.041 | −0.005, 0.088 | 0.081 |
| Significant variables in multivariable regression | ||||||
| Baseline BCVA | −0.619 | −0.652, −0.587 | < 0.001 | −0.659 | −0.721, −0.597 | < 0.001 |
| Post‐operative lens status (baseline = phakic), Aphakic/pseudophakic | −0.128 | −0.148, −0.108 | < 0.001 | −0.144 | −0.201, −0.087 | < 0.001 |
| Pre‐operative lens status (baseline = phakic), Aphakic/pseudophakic | −0.030 | −0.054, −0.007 | 0.012 | 0.061 | 0.006, 0.117 | 0.031 |
| MH size (baseline = small/medium), Large | −0.048 | −0.078, −0.017 | 0.002 | 0.109 | 0.058, 0.161 | < 0.001 |
| MH size (baseline = small/medium), X‐large+ | −0.009 | −0.053, 0.035 | 0.7 | 0.209 | 0.145, 0.272 | < 0.001 |
| Non‐significant variables in multivariable regression | ||||||
| Age (in years) | 0.000 | −0.001, 0.001 | 0.5 | — | — | — |
| Gender (baseline = female), Male | 0.006 | −0.015, 0.027 | 0.6 | — | — | — |
| Pre‐operative duration of hole (in months) | 0.002 | 0.000, 0.004 | 0.049 | 0.003 | 0.000, 0.006 | 0.054 |
| Pre‐operative vitreous attached to hole margins (baseline = no), Yes | −0.004 | −0.024, 0.017 | 0.7 | — | — | — |
| Follow‐up duration (in days) | 0.000 | 0.000, 0.000 | < 0.001 | 0.000 | 0.000, 0.000 | 0.6 |
| Surgeon grade (baseline = consultant), Fellow/registrar | 0.019 | −0.016, 0.055 | 0.3 | — | — | — |
| Year | Author | Study type | MH size (μm) | ILM peel, | ILM flap, | Follow‐up (months) | Closure rate | Visual acuity |
|---|---|---|---|---|---|---|---|---|
| 2018 | Kannan [ | RCT | 600–1500 | 30 | 30 (classic) | 6 |
|
|
| 2018 | Manasa [ | RCT | > 600 | 48 | 43 (inverted cover) | 3 |
|
|
| 2018 | Velez‐Montoya [ | RCT | > 400 | 12 | 12 (classic), 14 (free) | 3 |
|
|
| 2010 | Michalewska [ | RCT | > 400 | 51 | 50 (classic) | 12 |
|
|
| 2025 | Jin | Retrospective cohort | Mean: 300 μm (IQR: 200 to 422) | 2871 | 119 | 3 |
|
|
| 2024 | Bencheqroun [ | Retrospective cohort | > 650 | 58 | 16 (classic) | 10 |
|
|
| 2024 | Macchi [ | Retrospective cohort | > 500 | 59 | 18 (classic), 36 (pedicle transposition), 16 (free) | 6 |
|
|
| 2024 | Riding [ | Retrospective cohort (BEAVRS) | > 500 | 110 | 80 (superior) | Min. 2 |
|
|
| 2024 | Chen [ | Retrospective cohort | 400–650 | 37 | 32 (temporal) | 6 |
|
|
| 2024 | Suarez [ | Retrospective cohort | 38–1109 | 130 | 30 (inverted—‘cover’) | Min. 3 |
|
|
| 2024 | Morikawa [ | Retrospective cohort | Mean: ILM flap (415 ± 173) vs. ILM peel (396 ± 201) | 41 | 25 (classic) | 12 |
|
|
| 2024 | Ďurana [ | Retrospective cohort | 46–724 | 43 | 24 (inverted ILM flap without extra manipulation) | 2 |
|
|
| 2023 | Koçak [ | Retrospective cohort | > 600 | 32 | 28 (temporal) | 6 |
|
|
| 2023 | Dera [ | Retrospective cohort | > 400 | 52 | 65 (classic and temporal) | 14 |
|
|
| 2023 | Chen [ | Retrospective cohort | Mean: 519.46 | 34 | 15 (classic) | 12 |
|
|
| 2023 | Michalewicz [ | Retrospective cohort | ILM flap (421.90 ± 158.53) vs. ILM Peel (322.61 ± 159.62) | 61 | 48 (classic) | Max. 6.4 years |
|
|
| 2023 | Kwak [ | Retrospective cohort | Mean: ILM Flap (393.69) vs. ILM Peel (385.73) | 26 | 26 (superior) | 12 |
|
|
| 2023 | Carballés [ | Retrospective cohort | 183–760 | 36 | 44 (superior) | 6 |
|
|
| 2021 | Yan [ | Retrospective cohort | 154–1066 | 19 | 29 (inverted—‘cover’) | 6 |
|
|
| 2020 | Baumann [ | Retrospective cohort | > 400 | 49 | 68 (classic) | 12 |
|
|
| 2019 | Avci [ | Retrospective cohort | > 400 | 18 | 15 (temporal) | 12 |
|
|
| 2018 | Yamashita [ | Retrospective cohort | > 400 | 105 | 60 (classic) | Min. 6 |
|
|
| 2018 | Rizzo [ | Retrospective cohort | Not stated | 300 | 320 (classic) | 9 |
|
|
| 2025 | Tzoumas [ | Systematic Review | Mainly large MHs (IQR 450–744 μm) | 13 RCTs, 792 eyes | ILM flap (509–315, 61.9% ‘classic’ vs. 194, 38.1% ‘cover’ inverted), 283 ILM peel | 6 |
|
|
| 2024 | Zhang [ | Systematic Review | 227.0–803.3 | 68 papers incl. 19 RCTs, 7257 eyes | ILM peel (6112), inverted ILM flap (1145) | — |
|
|
| 2023 | Rezende (CLOSE study) [ | Systematic Review | > 400 | 31 papers, 1135 eyes | ILM peel (683), ILM flap (233), macular hydrodissection (64), human amniotic mem‐ brane graft (59), and autologous retinal transplantation (96) | 3 years |
|
|
| 2023 | Ghoraba [ | Systematic Review | > 400 | 4 RCTs, 285 eyes | ILM peel, classic flap | Min. 3 |
|
|
| 2020 | Shen [ | Systematic Review | > 400 | 4 RCTs and 4 case series, 593 eyes | ILM peel (325), inverted ILM flap (268) | Min. 3 |
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Macular Surgery · Ocular Disorders and Treatments · Corneal Surgery and Treatments
Introduction
1
Full thickness macular holes (FTMHs) are anatomical defects at the fovea, characterised by a disruption in the neural retinal layers [1]. They have a significant impact on vision, which may present as a loss of central vision, metamorphopsia, or scotomas. Idiopathic FTMHs are more common in the elderly and have an estimated incidence of 7.8 eyes per 100,000 individuals [2]. Surgical treatment of FTMHs involves pars plana vitrectomy, posterior hyaloid detachment if attached, and intravitreal gas tamponade. The internal limiting membrane peeling (ILM‐P) was introduced in 1997 by Eckardt et al. [3] and has become the mainstay approach for FTMHs, with up to 100% anatomical success [4, 5]. However, the challenge lies in large (> 400 μm) and chronic FTMHs where closure rates fall below 90% [4, 6, 7].
The inverted ILM flap (ILM‐F) was first described by Michalewska et al. [8] in 2009 to improve surgical outcomes in large FTMHs. In 50 eyes treated with ILM‐F, 98% closure was achieved [8]. Since its introduction, closure rates have reached 98.5% in large (> 400 μm) FTMHs [8, 9, 10]. Recent studies suggest that a higher threshold of approximately 500–650 μm may be more appropriate for the ILM‐F technique due to a lack of anatomical benefit in smaller holes and adverse effects on the outer retinal layers [4, 5, 11, 12]. Many of these studies primarily focus on anatomical outcomes rather than functional outcomes.
To address this knowledge gap, the anatomical and functional outcomes of the ILM‐F and conventional ILM‐P techniques for idiopathic FTMHs were evaluated within a large, bi‐national surgical registry dataset.
Methods
2
A retrospective analysis was performed on all patients from the Australian and New Zealand Society of Retinal Specialists Retinal Surgery (ANZSRS) Registry with idiopathic full thickness macular holes (FTMHs) who underwent vitrectomy surgery for primary macular hole repair between October 2006 and November 2023. The ANZSRS Registry is an online registry of vitreoretinal surgery performed by participating public and private operating centres in Australia and New Zealand. This study was approved by the Royal Australian and New Zealand College of Ophthalmologists Human Research Ethics Committee (Study 101.19 e A Retinal Surgery Logbook and Audit Tool) and adhered to the tenets of the Helsinki Declaration and the Good Medical Practice Guidelines.
Eyes were included if the FTMH was repaired using ILM‐F (inversion of ILM into or over the hole) or conventional ILM‐P (complete removal of ILM around the hole). As this was a registry‐based study, the exact ILM‐F technique performed was not specified and was at the discretion of the surgeon. Exclusion criteria included: FTMHs secondary to trauma, myopia, or any other ocular pathologies; recurrent or persistent FTMHs; other procedures to close the MH; a follow‐up duration of less than 3 months; and inadequate baseline or follow‐up documentation. In cases of bilateral FTMH repairs, both eyes were included if they met the inclusion and exclusion criteria.
Baseline characteristics included patient demographics, best corrected visual acuity (BCVA) measured with a Snellen chart and converted to logarithm of the minimum angle of resolution (logMAR) for statistical analysis, laterality, FTMH size, patient‐reported duration of symptoms, lens status, and whether vitreous was attached to FTMH margins. FTMHs were classified as small (≤ 250 μm), medium (> 250 and ≤ 400 μm), or large (> 400 and ≤ 550 μm) as described by the International Vitreomacular Traction Study (IVTS) [13], and X‐large (> 550 and ≤ 800 μm), XX‐large (> 800 and ≤ 1000 μm) or giant (> 1000 μm) based on the Classification for Large Macular Hole Studies (CLOSE study group) [14]. Surgical information included surgeon grade (consultant/trainee), gauge of surgical instrumentation, posterior vitreous detachment induction, ILM stain, combined phacoemulsification/vitrectomy surgery, type of tamponade agent, and duration of prescribed face‐down posturing. At the final follow‐up, time (in days post‐operatively), BCVA, macular hole closure, and lens status were also recorded.
Outcomes
2.1
The primary endpoint of this study was the rate of hole closure on optical coherence tomography (OCT) scans after a single procedure at the follow‐up visit. The secondary endpoint was BCVA change (∆ logMAR) calculated by the difference between pre‐operative BCVA and post‐operative BCVA at the 3‐month follow‐up.
Statistical Analysis
2.2
All statistical analyses were carried out using statistical software R (version 4.2.2, R Core Team, 2021) [15]. Due to limited sample sizes in the small, XX‐large, and giant groups, the MH size groupings were consolidated into three categories: small/medium, large, and X‐large + (including XL, XXL, and giant). Categorical variables were summarised as frequencies and proportions, while continuous variables were presented as either median (Me) and interquartile range (Q1, Q3) or mean and standard deviation (SD). For categorical data, Chi‐square (χ2) test and Fisher's exact test were applied based on sample size. For continuous data, independent t‐test and Wilcoxon rank‐sum test differences were used depending on the normality of the data. A p value of < 0.001 indicates non‐normality using the Shapiro–Wilk test.
Univariable regression analysis was first conducted to identify covariates significantly associated with the outcome, including surgical technique, age, gender, pre‐operative BCVA, MH size, duration of MH, lens status (pre‐ and post‐operative), vitreous attachment to hole margins, duration of follow‐up, and grade of the surgeon. Significant covariates (p < 0.05) were included in the stratified overlap‐weight propensity adjustment and weighted multivariable regression analysis. To account for covariate imbalance and potential residual confounding, first overlap‐weight propensity‐score adjustment (estimand = average treatment effect in the overlap population) within each hole‐size stratum was applied using the WeightIt package. Covariate balance before and after weighting was evaluated with standardised mean differences, targeting |SMD| < 0.10 as the balance criterion. Stratum‐specific weights were combined, and a weighted multivariable regression model was fit using the svyglm function with a binomial or gaussian error distribution for binary and continuous outcomes, respectively. In all multivariable regression analyses, interaction terms between hole size groupings and closure technique were assessed and included in the final model where they were statistically significant. Overlap‐weighted estimated marginal means (EMMs) were calculated and reported. In all regression analyses, only complete cases (i.e., cases with valid values for both the outcome variables and all covariates) were included. A p value of < 0.05 was considered statistically significant.
Results
3
Clinical Profile
3.1
Two thousand nine hundred ninety eyes from 2905 patients were identified from the Macular Hole Surgery dataset of the ANZSRS registry, 119 eyes underwent ILM‐F and 2871 eyes underwent conventional ILM‐P (Figure 1). The mean age of the population was 69 ± 9 years. 2019 (67.5%) eyes were from female patients. The median MH size was 300 μm (interquartile range [IQR], 200–422 μm) and the median follow‐up time was 112 days (IQR, 84–153 days). Bilateral FTMHs were present in 85 patients.
Flowchart illustrating identification of patients included from the ANZSRS registry macular hole surgery dataset. Abbreviations: BCVA, best corrected visual acuity, ILM, internal limiting membrane; ILM‐F, internal limiting membrane flap; ILM‐P, internal limiting membrane peeling.
Table 1 summarizes the baseline characteristics of the ILM‐F and ILM‐P groups. There were no statistically significant differences between the two groups in terms of sex, pre‐operative vitreous attachment to hole margins, and pre‐operative lens status. The mean age was significantly higher in the ILM‐F group (71 ± 7 years) compared to the ILM‐P group (69 ± 9 years, p = 0.013). The median pre‐operative MH size was significantly greater in the ILM‐F group (521 μm) compared to the ILM‐P group (296 μm, p < 0.001). The distribution of MH size groupings differed between the two groups, with a greater proportion of MHs > 400 μm in the ILM‐F group (80.6%) compared to the ILM‐P group (25.6%, p < 0.001). The MHs in the ILM‐F group had a longer median symptom duration (6 vs. 3 months, p < 0.001) and a worse median pre‐operative BCVA (0.9 logMAR vs. 0.7 logMAR, p < 0.001) compared to those in the ILM‐P group. In contrast, the ILM‐P group had a higher consultant‐to‐trainee ratio (8.2:1) compared to the ILM‐F group (3.1:1; p < 0.001). Post‐operatively, the proportion of aphakic/pseudophakic eyes was significantly higher in the ILM‐F group (64.7%) compared to the ILM‐P group (48.6%).
Anatomical Outcomes
3.2
Unadjusted MH closure was achieved in 115/119 cases (96.6%) in the ILM‐F group and 2778/2871 cases (96.8%) in the ILM‐P group. In the univariable analysis, significant variables were namely pre‐operative vitreous attachment to hole margins, MH size, duration of MH, baseline BCVA, and surgeon grade (Table 2). Closure rates following adjustment for covariables were 98.5% in the ILM‐F group and 95.6% in the ILM‐P group. Weighted multivariable regression analysis showed that ILM‐F was significantly associated with higher odds of hole closure compared to ILM‐P (OR = 2.969, 95% CI: 1.075 to 8.199, p = 0.036). No significant interaction effects were observed, indicating that the odds of anatomical success with ILM‐F and ILM‐P did not significantly differ by MH size. Among the independent predictors of MH closure, pre‐operative vitreous attachment to the hole margins significantly increased the odds of closure (OR = 2.632, 95% CI: 1.382 to 5.014, p = 0.003). Factors associated with reduced odds of anatomical success were MH size groupings > 400 μm (X‐large + OR = 0.117, 95% CI: 0.061 to 0.226, p < 0.001; large OR = 0.282, 95% CI: 0.151 to 0.525, p < 0.001) and surgeries performed by fellows/registrars (OR = 0.451, 95% CI: 0.205 to 0.993, p = 0.048). Figure 2 illustrates a reduction in the adjusted closure rates with increasing MH size for both ILM‐F and ILM‐P techniques. Closure rates dropped below 95% for X‐large+ MHs in the ILM‐P group, while rates of ILM‐F remained consistently above 95% across all size groupings.
Estimated marginal means of 3‐month hole closure rate for ILM flap and ILM peel techniques across macular hole sizes.
Functional Outcomes
3.3
The adjusted gain in BCVA from baseline to 3‐month follow‐up was −0.221 logMAR in the ILM‐F group and −0.262 logMAR in the ILM‐P group. In the univariable analysis, baseline BCVA, MH size, duration of MH, pre‐operative and post‐operative lens status, and follow‐up duration were found to be significantly associated with BCVA change (Table 3). After adjusting for these covariates, there was no significant difference in BCVA change between the two closure techniques (β = 0.041, 95% CI: −0.005 to 0.088, p = 0.081). Figure 3 illustrates the adjusted visual improvement with both ILM‐F and ILM‐P techniques across all MH size groupings. No significant interaction effects suggest that comparable visual outcomes between ILM‐F and ILM‐P were consistent across all MH sizes. Two predictors of greater BCVA gain were worse baseline BCVA (β = −0.659, 95% CI: −0.721 to −0.597, p < 0.001) and post‐operative aphakic/pseudophakic lens status (β = −0.144, 95% CI: −0.201 to −0.087, p < 0.001). Both large (β = 0.109, 95% CI: 0.058 to 0.161, p < 0.001) and X‐large + (β = 0.209, 95% CI: 0.145 to 0.272, p < 0.001) MHs were associated with less BCVA gain at 3 months. Pre‐operative aphakic/pseudophakic lens status was also significantly associated with less BCVA gain (β = 0.061, 95% CI: 0.006 to 0.117, p = 0.031).
Estimated marginal means of 3‐month visual acuity change for ILM flap and ILM Peel techniques across macular hole sizes.
Discussion
4
Using binational registry data from a cohort of 2990 eyes, our results showed that the ILM flap technique has an anatomical benefit in the primary closure of idiopathic FTMHs with an OR of 2.97. Visual outcomes were no different using ILM‐F and conventional ILM‐P.
There is ongoing debate on whether ILM flaps yield anatomical and functional benefits over conventional complete ILM peeling and whether there is a size cut‐off at which FTMHs are most likely to benefit. Prior studies assessing this show conflicting results and are presented in Table 4. Limitations of many of these studies include small sample sizes, non‐randomisation and non‐comparative analyses, inclusion of non‐idiopathic macular holes, heterogeneity in follow‐up duration, different surgical techniques, different definition of hole closure [10, 17], lack of reporting of functional outcomes and poor adjustment for baseline characteristics including macular hole size, duration and lens status.
Michalewska et al. first described a 98% closure rate with the inverted ILM flap technique compared to 88% with conventional ILM peeling for large (> 400 μm) macular holes in a randomised controlled trial (RCT) [8]. Six retrospective cohort studies focusing on large idiopathic FTMHs showed that the ILM‐F technique achieved higher closure rates compared to the ILM‐P technique (Table 4) [9, 10, 11, 20, 24, 30]. In two systematic reviews, Ghoraba et al. [35] and Shen et al. [36] found that the ILM‐F increased anatomical closure by a relative risk of 10% and an OR of 3.95, respectively. Another recent systematic review by Tzoumas et al. [33], including 13 RCTs and 792 eyes of all MH sizes, showed a similar adjusted OR of 4.80. The authors found that ILM‐F was more likely beneficial for holes > 500 μm (OR = 3.14 to 9.64, p < 0.001). In this study, a hole closure rate of above 95% was achieved using the ILM‐F technique, which is considered a benchmark of success with MH repair.
The proposed mechanism of benefit for the inverted ILM‐F is its potential to act as a scaffold to promote the proliferation and migration of Müller cells and gliosis [8, 37, 38]. Using experimental monkey models, Shiode et al. [39] observed neuronal modelling from activated Müller cells produced neurotrophic factors and basic fibroblast growth factors on the ILM surface, only 10 days after ILM flap surgery. In addition, the ILM‐F is thought to function as a barrier to fluid entry from the vitreous into the subretinal space [39, 40].
Despite higher closure rates with the ILM‐F technique, our study did not find a functional benefit of the ILM‐F compared to conventional peeling. However, the follow up time was relatively short and many more eyes in the ILM‐F group had larger or more chronic holes that may take longer to recover full visual acuity. Greater BCVA gain was found in eyes with worse baseline BCVA. This likely reflects a ceiling effect in those with better baseline BCVA. The benefit of post‐operative aphakic/pseudophakic lens status probably reflects the impact of cataract surgery improving vision.
One RCT and 7 retrospective studies have found comparable visual outcomes between ILM‐F and ILM‐P [16, 21, 22, 23, 25, 29, 31]. Five retrospective studies corroborate our study findings where despite an anatomical superiority of ILM‐F, functional outcomes were no different [9, 11, 20, 24, 26]. In these cases, there was no difference in the recovery of the outer retinal layers [9, 10]. Two studies even showed that ILM‐P had a favourable visual acuity benefit over ILM‐F for idiopathic FTMHs. Bencheqroun et al. [19] conducted a retrospective study, which found that conventional ILM‐P was superior in BCVA gain compared to ILM‐F (p = 0.04) at a mean of 10 months. Chen et al. [12] found a better post‐operative BCVA at 1, 3, and 6 months (p = 0.039, 0.005, and 0.006) with ILM‐P [12]. They hypothesized that an ILM‐F might fill the hole after air‐gas exchange and impede external limiting membrane (ELM) and ellipsoid zone (EZ) recovery. Excessive gliosis could have cytotoxic effects on retinal neurons, leading to a worse visual prognosis [39]. Earlier studies identified this as foveal hyperreflective lesions, which were associated with EZ disruption [8, 39]. Iatrogenic trauma can also occur with insertion of ILM into the fovea [41, 42]. Larger FTMHs often favour ILM flap, where photoreceptor loss or atrophy may result in limited visual improvement.
Conversely, three studies showed that ILM‐F achieved a better post‐operative absolute or gain in visual acuity in larger MHs [10, 17, 30]. Recent studies suggest that the ILM‐F technique may offer superior early visual recovery compared to conventional ILM peeling, but longer‐term visual outcomes appear comparable between the two techniques. Carballés et al. [28] noticed a quicker recovery in visual acuity at 3 months using ILM‐F, but the difference in absolute BCVA was not significant at 6 months. Kwak et al. [27] observed an early recovery at 1 month, but no significant difference between the two groups at 3 months. Similarly, a meta‐analysis by Shen et al. [36] described a significantly greater visual acuity improvement using ILM‐F compared to ILM‐P at 3 months, which did not reach significance at 6 months. As visual acuity recovery is driven by the restoration of outer retinal layers, the wide range of follow‐up durations (2 months to 6.4 years) may confound unadjusted visual outcomes analyses [43]. The 3‐month timepoint in this study was chosen to most accurately reflect the typical post‐operative assessment timepoint and to minimise confounding from post‐operative cataract development.
There was a trend of more surgeons performing fewer ILM‐F procedures compared to the number of surgeons performing ILM‐P only surgeries. This may suggest less experience with the ILM‐F technique. Our data showed that despite better hole closure with consultants, visual acuity was not significantly different between consultants and trainees. However, the surgeon's experience with one technique cannot be deduced by their grade (consultant or trainee). The relative use of ILM‐F compared to ILM‐P has increased from 2017 to the end of 2023.
To our best knowledge, our study has the largest number of subjects undergoing ILM flap or ILM peeling. We are the first to systematically report macular holes exceeding 400 μm using the CLOSE study classifications, which incorporate the debated 500–600 μm cutoff point. A robust regression model was used to adjust for covariates and allowed us to test the effect of hole size and closure technique. The use of a binational multicentre registry data reduced selection bias, thereby improving the generalizability of our findings. Limitations of this study include its retrospective nature. The ILM‐F technique was not documented. Some studies have found similar closure rates between single‐layered ‘cover’ and classic ‘fill’ techniques, [40, 41, 44] whilst others have shown superior visual recovery with a pedicle transposition flap over a free flap [20]. The follow‐up of 3 months may be too short to fully appreciate visual gains following surgery. Visual acuity measurement does not account for reductions in scotoma size and metamorphopsia [45]. Other measures of vision, such as multifocal electroretinogram, microperimetry, and metamorphopsia assessments, may form a more comprehensive functional analysis.
In conclusion, the ILM‐F technique was superior to conventional ILM‐P in achieving FTMH closure but there was no additional visual acuity benefit. Given the ultimate goal of surgery is to improve visual outcomes, ILM‐F is not required in smaller and medium sized holes where MH closure rates are already high with ILM‐P. We recommend other surgical registries to study their data on ILM flaps, with particular attention to any functional benefit or detriment compared to conventional ILM peeling. More studies including comparative analyses of ILM flap techniques are required.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. D. M. Gass , “Idiopathic Senile Macular Hole: Its Early Stages and Pathogenesis,” Archives of Ophthalmology 106, no. 5 (1988): 629–639, 10.1001/archopht.1988.01060130683026.3358729 · doi ↗ · pubmed ↗
- 2F. S. Ali , J. D. Stein , T. S. Blachley , S. Ackley , and J. M. Stewart , “Incidence of and Risk Factors for Developing Idiopathic Macular Hole Among a Diverse Group of Patients Throughout the United States,” JAMA Ophthalmology 135, no. 4 (2017): 299–305, 10.1001/jamaophthalmol.2016.5870.28208188 PMC 5470400 · doi ↗ · pubmed ↗
- 3C. Eckardt , U. Eckardt , S. Groos , L. Luciano , and E. Reale , “Entfernung der Membrana limitans interna bei Makulalöchern,” Der Ophthalmologe 94, no. 8 (1997): 545–551, 10.1007/s 003470050156.9376691 · doi ↗ · pubmed ↗
- 4D. H. Steel , P. H. J. Donachie , G. W. Aylward , D. A. Laidlaw , T. H. Williamson , and D. Yorston , “Factors Affecting Anatomical and Visual Outcome After Macular Hole Surgery: Findings From a Large Prospective UK Cohort,” Eye 35, no. 1 (2021): 316–325, 10.1038/s 41433-020-0844-x.32231259 PMC 7852599 · doi ↗ · pubmed ↗
- 5S. W. Ch'ng , N. Patton , M. Ahmed , et al., “The Manchester Large Macular Hole Study: Is It Time to Reclassify Large Macular Holes?,” American Journal of Ophthalmology 195 (2018): 36–42, 10.1016/j.ajo.2018.07.027.30071212 · doi ↗ · pubmed ↗
- 6M. S. Ip , “Anatomical Outcomes of Surgery for Idiopathic Macular Hole as Determined by Optical Coherence Tomography,” Archives of Ophthalmology 120, no. 1 (2002): 29, 10.1001/archopht.120.1.29.11786054 · doi ↗ · pubmed ↗
- 7B. Gupta , D. A. H. Laidlaw , T. H. Williamson , S. P. Shah , R. Wong , and S. Wren , “Predicting Visual Success in Macular Hole Surgery,” British Journal of Ophthalmology 93, no. 11 (2009): 1488–1491, 10.1136/bjo.2008.153189.19635721 · doi ↗ · pubmed ↗
- 8Z. Michalewska , J. Michalewski , R. A. Adelman , and J. Nawrocki , “Inverted Internal Limiting Membrane Flap Technique for Large Macular Holes,” Ophthalmology 117, no. 10 (2010): 2018–2025, 10.1016/j.ophtha.2010.02.011.20541263 · doi ↗ · pubmed ↗