Genotypic and Phenotypic Detection of Fosfomycin and Tigecycline Resistance Genes From Clinical Isolates of Enterobacter cloacae
Sanjida Hossain, Shahnaz Choudhury, AKM Mohiuddin Bhuiyan, Adneen Moureen, Redoy Ranjan, SK Jakaria Been Sayeed, Abdullah Yusuf

TL;DR
This study identifies antibiotic resistance genes in Enterobacter cloacae isolates from clinical samples in Bangladesh.
Contribution
The study provides new insights into the prevalence of fosfomycin and tigecycline resistance genes in clinical isolates of Enterobacter cloacae.
Findings
56.7% of isolated Enterobacter species were multidrug-resistant.
fosA was the most common fosfomycin resistance gene detected in 65% of resistant isolates.
Only 27.3% of tigecycline-resistant isolates carried the tetA gene.
Abstract
Background The emergence of multidrug-resistant (MDR) Enterobacter species is a growing concern, driving increased morbidity and mortality, particularly due to hospital-acquired infections. Objective This study aimed to identify multidrug-resistant Enterobacter cloacae through the detection of antibiotic resistance genes. Methodology This cross-sectional study was conducted in the Department of Microbiology at Dhaka Medical College, Dhaka, Bangladesh, from November 2022 to June 2023 for a period of one year. All the clinically suspected patients who were presented with the infection of different body sites were divided into two groups: male and female. Then, each group is segmented into four specific age brackets: 20-30, 31-40, 41-50, and 51-60. The multidrug-resistant Enterobacter cloacae were isolated from patients admitted to Dhaka Medical College Hospital, Dhaka, Bangladesh.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
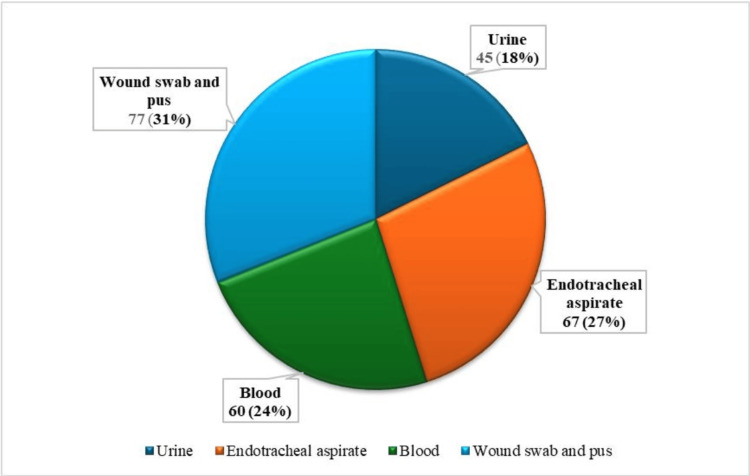 Figure 1
Figure 1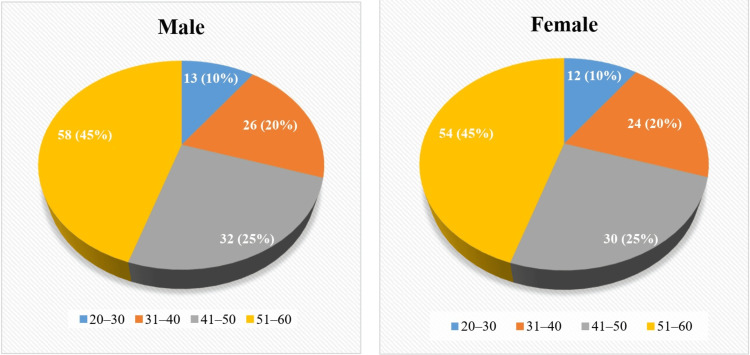 Figure 2
Figure 2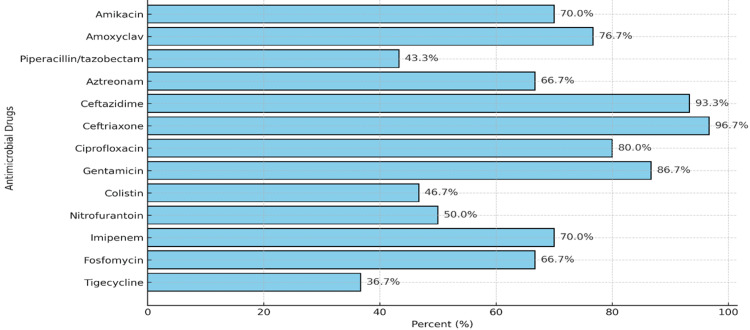 Figure 3
Figure 3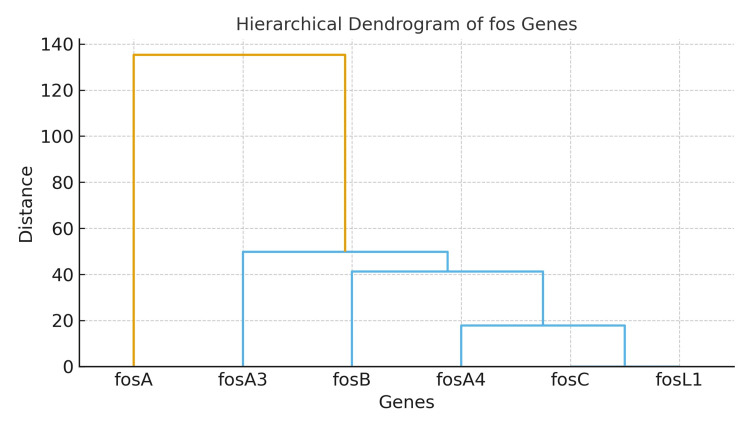 Figure 4
Figure 4| Genes | Primer name | Primer sequence (5'-3') | bp (base pair) |
| fosA | fosA-F fosA-R | ATCTGTGGGTCTGCCTGTCGT ATGCCCGCATAGGGCTTCT | 271 |
| fosA3 | fosA3-F fosA3- R | CCTGGCATTTTATCAGCAGT CGGTTATCTTTCCATACCTCAG | 221 |
| fosA4 | fosA4-F fosA4-R | CTGGCGTTTTATCAGCGGTT CTTCGCTGCGGTTGTCTTT | 230 |
| fosB | fosB-F fosB-R | CAGAGATATTTTAGGGGCTGACA CTCAATCTATCTTCTAAACTTCCTG | 312 |
| fosC | fosC-F fosC-R | CCTTGCTCACTGGGGATCTG TACAAGACCCGACGCACTTC | 354 |
| fosX | fosX-F fosX-R | TGTCCCTCACCTTCGACTCT TTGCTGGTCTGTGGATTTGC | 382 |
| FosL1 | fosL1-F fosL1-R | GCAAGCGCAGACACAGACAG CTTGGCACAAGGTGGAACTTC | 516 |
| tetX4 | tetX4-F tetX4-R | TTGGGACGAACGCTACAAAG CATCAACCCGCTGTTTACGC | 181 |
| tetA | tetA-F tetA-R | GTGAAACCCAACATACCCC GAAGGCAAGCAGGATGTAG | 850 |
| Sample source | Enterobacter species | MDR (%) | XDR (%) | PDR (%) |
| Urine | E. cloacae | 15 | 5 | 2 |
| Wound swab annd pus | E. cloacae | 20 | 5 | 3 |
| Endotracheal aspirate (ETA) | E. cloacae | 10 | 3 | 3 |
| Blood | E. cloacae | 11.7 | 3.7 | 2 |
| Urine | E. aerogenes | 40.0 | 0.0 | 0.0 |
| Sample | Genes | |
| Urine (n=6) | 0 (0.0%) | 2 (33.3%) |
| Wound swab and pus (n=4) | 0 (0.0%) | 1 (25.0%) |
| Endotracheal aspirate (ETA) (n=1) | 0 (0.0%) | 0 (0.0%) |
| Blood (n=0) | 0 (0.0%) | 0 (0.0%) |
| Total (n=11) | 0 (0.0%) | 3 (27.3%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Urinary Tract Infections Management · Neutropenia and Cancer Infections
Introduction
Enterobacter species are widely present in nature and often inhabit the intestinal microbiota of both humans and animals, with the capacity to survive on skin and dry surfaces, as well as to proliferate in contaminated liquids [1-2]. Enterobacter species are significant contributors to hospital-acquired infections and are frequently isolated [3]. Among the *Enterobacter *genus, Enterobacter cloacae and Enterobacter aerogenes are the species most commonly recovered [4]. The *Enterobacter *species mainly cause nosocomial infections, including UTIs, respiratory infections, soft tissue infections, osteomyelitis, and endocarditis [5]. In the United States, *Enterobacter *spp. ranks as the second most prevalent carbapenem-resistant Enterobacteriaceae (CRE) [6].
The rising antimicrobial resistance of Enterobacter cloacae is a significant concern. It has particularly given over 60.0% resistance to critical antibiotics such as polymyxin B, tigecycline, and nitrofurantoin. Despite ongoing efforts to develop new antibiotics for treating these resistant infections, progress has been minimal. This situation necessitates coordinated efforts at multiple levels to improve the management of AMR infections [7]. While most cases are linked to healthcare environments, instances in community settings are on the rise. Alterations in porin channels, the presence of integrons and insertion sequence common region 1 (ISCR1) carrying resistance genes, along with the activity of efflux pumps, collectively play a role in conferring these resistance traits [8].
The rise of carbapenem non-susceptible strains is largely due to the production of carbapenemases, as well as extended-spectrum beta-lactamases (ESBL) and AmpC beta-lactamases. The action of efflux pumps also contributes to antimicrobial resistance [9]. It's not unexpected that carbapenem-resistant Enterobacter species are classified as ESKAPE pathogens, which are deemed some of the most concerning healthcare-associated pathogens globally [10]. This study aimed to identify multidrug-resistant Enterobacter cloacae through the detection of antibiotic resistance genes.
Materials and methods
Study settings and population
This cross-sectional study was conducted in the Department of Microbiology at Dhaka Medical College, Dhaka, Bangladesh, from November 2022 to June 2023 for a period of one year. All the clinically suspected patients who were presented with the infection of different body sites were divided into two groups: male and female. Then, each group is segmented into four specific age brackets: 20-30, 31-40, 41-50, and 51-60. The multidrug-resistant *Enterobacter cloacae *were isolated from patients admitted to Dhaka Medical College Hospital, Dhaka, Bangladesh. Dhaka Medical College Hospital, Dhaka, is situated in the capital of Bangladesh with a capacity of 1500 beds. However, there are more than 4000 patients who were admitted to this hospital. This is a public general teaching hospital. All the subjects related to the departments of medicine and surgery are available here. Bangladesh is a densely populated country with a population of 18 million. Patients from all corners of this country are admitted with different infectious diseases.
Selection criteria
In this study, the suspected cases of nosocomial infection were included, and the samples according to the site of infection were collected, which included urine, blood, wound swab, and pus samples from patients who were admitted to different indoor departments of Dhaka Medical College Hospital, Dhaka, Bangladesh. The endotracheal aspirates from ICU patients on mechanical ventilation for over 48 hours were also collected. Samples containing more than one organism were excluded from this study.
Study procedure
All samples were processed in the microbiology department for culture and sensitivity testing. Furthermore, the isolated bacteria were monitored for their antibiotic resistance pattern by the disk diffusion method.
Sample collection and species identification
The study collected 35 Enterobacter isolates from various clinical samples, including urine, wound swabs, endotracheal aspirates, and blood. Two Enterobacter species, Enterobacter cloacae and Enterobacter aerogenes, were identified through a series of biochemical tests, which included the Lysine decarboxylase test.
Antibiotic susceptibility testing
The antibiotic susceptibility of Enterobacter cloacae was evaluated using the Kirby-Bauer disc diffusion technique on Mueller-Hinton agar, with antibiotic discs obtained from Oxoid Ltd, UK. The antibiotics evaluated in this study were amikacin (30 µg), amoxiclav (30 µg), ceftazidime (30 µg), colistin (10 µg), ceftriaxone (30 µg), ciprofloxacin (30 µg), piperacillin/tazobactam (110/10 µg), imipenem (10 µg), tigecycline (15 µg), and gentamicin (30 µg). For the evaluation of tigecycline, imipenem, and fosfomycin susceptibility, provided by Beximco Pharma Limited, the agar dilution method was utilized to determine the minimum inhibitory concentration (MIC). The disc content and inhibition zones were interpreted according to the Clinical Laboratory Standards Institute guidelines (CLSI, 2022), while the interpretation of tigecycline results specifically followed criteria established by the United States Food and Drug Administration (2010). A 0.5 McFarland standard (equivalent to 1×10⁸ cfu/ml) was used for inoculum preparation and MIC testing, followed by a tenfold dilution to obtain a final concentration of 1×10⁷ cfu/ml. The inoculated plates were incubated aerobically at 37ºC overnight, and the MIC was recorded as the lowest antibiotic concentration on Mueller-Hinton agar that prevented visible bacterial growth. The definition and classification of multidrug-resistant (MDR), pan drug-resistant (PDR), and extensively drug-resistant (XDR) were based on the standard criteria of the CDC. *Escherichia coli *ATCC 25922 served as the quality control organism.
Polymerase chain reaction
To identify MDR genes in *Enterobacter *spp., polymerase chain reaction (PCR) was performed. A loopful of bacterial colonies from Mueller-Hinton agar (MHA) was collected and suspended in a microcentrifuge tube containing sterile tryptic soy broth (TSB), then incubated overnight at 37ºC. After incubation, the tube was centrifuged at 4000 g for 10 minutes, the supernatant discarded, and the bacterial pellet stored at -20ºC for subsequent DNA extraction. For DNA extraction, 300 µl of sterile distilled water was added to the pellet, vortexed thoroughly, and heated at 100ºC for 10 minutes. The tubes were then cooled on ice for five minutes and centrifuged at 14,000 g for six minutes at 4ºC, after which the supernatant containing DNA was transferred to a new tube. Extracted DNA was stored at 4ºC for 7-10 days or at -20ºC for long-term use. For PCR, a 25 µl reaction mixture was prepared in a PCR tube, containing 12.5 µl of mastermix (with dNTPs, Taq polymerase, MgCl₂, and PCR buffer), 2 µl each of forward and reverse primers (Promega Corporation, USA), 2 µl of extracted DNA, and 6.5 µl of nuclease-free water. The mixture was briefly vortexed and centrifuged. Amplification was carried out using a thermal cycler (Gene Atlas, Master cycler gradient, Model 482, Japan). After PCR, the amplified products were either analyzed by gel electrophoresis or stored at -20ºC for future experiments.
Agarose gel electrophoresis
PCR products were visualized using agarose gel electrophoresis on a 1.5% agarose gel prepared with 1X TBE buffer (Tris-EDTA). To prepare the gel, 0.18 g of agarose powder (LE, analytical grade, Promega, Madison, USA) was dissolved in 1.25 ml of TBE buffer, poured into a gel tray with a comb, and allowed to solidify. For loading, 5 µl of the PCR product was mixed with 1 µl of loading dye on parafilm and placed into the wells, while 2 µl of a 100 bp DNA ladder was combined with 1 µl of loading dye and loaded into a separate well. Electrophoresis was conducted at 230 V for 30 minutes. The gel was then stained with ethidium bromide (20 µl in 200 ml distilled water) and visualized under a UV transilluminator (Gel Doc, Major Science, Taiwan). DNA bands were sized by comparison to the 100 bp DNA ladder. For sequencing, the PCR-amplified bacterial DNA was purified using FAVOGEN DNA purification kits (Biotech Corp).
Statistical analysis
Statistical analysis was performed by Windows-based Statistical Package for Social Science (SPSS) software, version 22.0 (IBM Inc., Armonk, New York). Continuous data were expressed as mean, standard deviation, minimum, and maximum. Categorical data were summarized in terms of frequency counts and percentages. The sample size was based on the number of isolated bacteria during the sample collection period.
Ethical consideration
All procedures of the present study were carried out in accordance with the principles for human investigations (i.e., Helsinki Declaration 2013) and also with the ethical guidelines of the institutional research ethics. Formal ethics approval was granted by the local ethics committee. Participants in the study were informed about the procedure and purpose of the study and the confidentiality of information provided. All participants consented willingly to be a part of the study during the data collection periods. All data were collected anonymously and were analyzed using the coding system.
Results
A total of 390 samples were analyzed in this study, among which 251 (64.4%) showed positive culture growth. The blood culture was positive in 60 (24.0%) cases. However, the urine culture was found in 45 (18.0%) cases. Endotracheal aspirate was positive in 67 (27.0%) cases. The positive culture was found in 77 (31.0%) cases in wound swab and pus culture (Figure 1).
Culture positivity from different clinical samples
A comparative visualization of age distribution across genders, segmented into four distinct age brackets. The data highlights a significant contrast, with a higher concentration of females in the 20-30 age group and males in the 51-60 age group (Figure 2).
Age group distribution by gender
The distribution of Enterobacter species was recorded along with their multidrug-resistant (MDR), extensively drug-resistant (XDR), and pan drug-resistant (PDR) patterns, categorized by patient variables including age, sex, and clinical sample sources (Table 2).
The percentage of susceptibility to different antimicrobial drugs was recorded. Ceftriaxone (96.7%) and ceftazidime (93.3%) had the highest susceptibility, while tigecycline (36.7%) and piperacillin/tazobactam (43.3%) showed the lowest. Overall, β-lactam antibiotics demonstrated the greatest activity against the isolates (Figure 3).
Antibiotic resistance pattern of isolated Enterobacter cloacae
The hierarchical cluster dendrogram below illustrates the clustering of fosfomycin resistance genes (fosA, fosA3, fosA4, fosB, fosC, and fosL1) according to their percentage distribution among different clinical samples. Genes with similar occurrence patterns, such as fosA and fosA3, are closely grouped, indicating possible co-occurrence or shared resistance mechanisms, while rarely detected genes like fosB, fosC, and fosL1 form separate branches (Figure 4).
Hierarchical dendrogram showing clustering of fos genes based on percentage prevalence across clinical samples
Table 3 summarizes the prevalence of two tetracycline resistance genes, tetX and tetA, across 11 clinical samples from four sources.
Discussion
This study presents novel insights into the genetic determinants of antibiotic resistance among Enterobacter cloacae isolates in Bangladesh. For the first time, the coexistence of fosA, fosA3, and fosA4 genes was detected, indicating diverse fosfomycin resistance mechanisms circulating in local clinical settings. The detection of the chromosomal tetA gene in 27.27% of isolates further suggests the role of efflux pumps in multidrug resistance. The co-occurrence of fos and tetA genes implies possible genetic linkage and co-selection under antibiotic pressure. Moreover, the absence of known tigecycline resistance genes highlights a gap in molecular surveillance, suggesting that tigecycline remains an effective treatment option in the region.
The global rise in antibiotic resistance represents a serious public health concern, contributing to significant morbidity and mortality [11]. Multidrug-resistant *Enterobacter *species are particularly concerning because of their role in nosocomial infections and their impact on therapeutic outcomes. In the present study, 251 out of 390 samples (64.36%) were culture positive, with 35 (13.94%) identified as Enterobacter species. This finding aligns with studies from Dhaka Medical College Hospital (DMCH), which reported culture positivity rates between 63.0% to 65.0% across different clinical specimens, including urine, wound swabs, blood, sputum, and pus [12-13]. Globally, *Enterobacter *accounts for approximately 11.0% of hospital-acquired infections involving the bloodstream, respiratory tract, and urinary tract [14].
Among the identified isolates, Enterobacter cloacae (85.7%) was the predominant species, followed by *Enterobacter aerogenes *(14.3%). This distribution corresponds with findings from previous studies in Bangladesh and India, which reported Enterobacter cloacae prevalence ranging from 77.0% to 79.0% isolates [15]. The predominance of *Enterobacter cloacae *may be linked to environmental persistence, antibiotic selection pressure, and similar infection control challenges shared across South Asian healthcare facilities.
Comparable findings have been reported in other Bangladeshi investigations, where Enterobacter cloacae accounted for more than 80.0% of *Enterobacter *infections and was strongly associated with ventilator-associated pneumonia and bloodstream infections [16]. International studies conducted in Iran, China, and other regions also describe *Enterobacter cloacae as the most frequently isolated Enterobacter species, often carrying multidrug resistance genes and integrons. These observations support the global emergence of Enterobacter cloacae *as an adaptable pathogen capable of acquiring and maintaining diverse resistance mechanisms.
The current study found a 70.0% imipenem resistance rate among *Enterobacter cloacae *isolates, similar to previous DMCH reports showing 70.97% resistance [16]. In contrast, lower rates have been reported in India (53.8%) and Palestine (12.2%), reflecting regional differences in antibiotic use and infection control practices [17-18]. The observed 66.7% fosfomycin resistance among isolates in this study was notably higher than the 36.0% resistance reported in Indian isolates [19].
Among fosfomycin-resistant isolates, 65.0% were positive for fosA, 20.0% for fosA3, and 15.0% for* fos*A4, demonstrating the predominance of fosA-mediated inactivation. This is consistent with earlier findings from DMCH, where fosA, fosA5, and fosB2 were reported among multidrug-resistant *Enterobacter *isolates [20]. In contrast, a study from China detected fosA3 in 26.1% of Enterobacter cloacae isolates [21], suggesting regional variability in resistance gene profiles likely influenced by differences in antimicrobial use and horizontal gene transfer events.
The presence of tetA genes in 27.3% of isolates indicates active efflux-mediated resistance, particularly via the major facilitator superfamily (MFS) mechanism. The coexistence of multiple resistance genes, such as fosA and tetA, raises concerns regarding plasmid-mediated gene transfer and the rapid dissemination of multidrug-resistant Enterobacter strains. The absence of known tigecycline resistance genes in local isolates is encouraging; however, continuous molecular surveillance for genes such as tet(X) and ramR mutations remains essential.
In summary, the findings of this study underscore the emergence of *Enterobacter cloacae *as a predominant multidrug-resistant pathogen in Bangladesh. The simultaneous presence of multiple resistance determinants reflects both local and global trends in antibiotic resistance evolution. Strengthening molecular surveillance, enforcing antibiotic stewardship, and improving infection control measures are vital to mitigating the further spread of resistance and preserving the efficacy of existing therapeutic options.
Limitations
The study was unable to detect certain resistance genes due to limitations in time and resources. Specifically, other tigecycline resistance genes, such as tetX6, were not analyzed. Similarly, some fosfomycin resistance genes, including fosL2, fosM1, and fosM2, could not be investigated. These constraints prevented a more comprehensive screening of all potential resistance determinants. Again, the small sample size, single-center design, lack of sequencing data, and absence of clinical outcome correlation are also limitations of the study.
Conclusions
In conclusion, Enterobacter cloacae shows a high rate of multidrug resistance, with the majority (around half) of isolates classified as MDR. There are several *fos genes that are responsible for resistance to antibiotics. *Among fosfomycin-resistant strains, the fosA gene was most common, while fosA3 and fosA4 appeared less frequently. This indicates the MDR profiles of the bacteria. In tigecycline-resistant isolates, the tetA gene was found at a lower level. This highlights the need for antimicrobial susceptibility testing before antibiotic use. However, it is very important to implement antibiotic stewardship to prevent the development of genes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Enterobacter cloacae complex: clinical impact and emerging antibiotic resistance Future Microbiol Mezzatesta ML Gona F Stefani S 887902720122282730910.2217/fmb.12.61 · doi ↗ · pubmed ↗
- 2Enterobacter bugandensis: a novel enterobacterial species associated with severe clinical infection Sci Rep Pati NB Doijad SP Schultze T 5392820182959951610.1038/s 41598-018-23069-z PMC 5876403 · doi ↗ · pubmed ↗
- 3Clinical features and outcomes of spontaneous bacterial peritonitis caused by Streptococcus pneumoniae: a matched case-control study Medicine (Baltimore) Kim T Hong SI Park SY 095201610.1097/MD.0000000000003796 PMC 490072127258513 · doi ↗ · pubmed ↗
- 4Extended-spectrum β-lactamase production among Enterobacter cloacae and Enterobacter aerogenes at a tertiary care center in coastal Karnataka Nat J Lab Med Vishwanath S Swetha PS Su Sh Ma M 052016 http://chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://njlm.net/articles/PDF/2131/18469_F(GH)_PF 1(Vsu GH)_PFA(GH)_PF 2(Vsu GH).pdf
- 5Enterobacter infections Ramirez D Giron M Treasure Island, FL Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/32644722/32644722 · pubmed ↗
- 6Carbapenem-resistant Enterobacter cloacae in patients from the US Veterans Health Administration, 2006-2015 Emerg Infect Dis Wilson BM El Chakhtoura NG Patel S Saade E Donskey CJ Bonomo RA Perez F 8788802320172841831810.3201/eid 2305.162034 PMC 5403041 · doi ↗ · pubmed ↗
- 7Virulence characteristics and an action mode of antibiotic resistance in multidrug-resistant Pseudomonas aeruginosa Sci Rep Hwang W Yoon SS 487920193067973510.1038/s 41598-018-37422-9PMC 6345838 · doi ↗ · pubmed ↗
- 8The global epidemiology of carbapenemase-producing Enterobacteriaceae Virulence van Duin D Doi Y 460469820172759317610.1080/21505594.2016.1222343 PMC 5477705 · doi ↗ · pubmed ↗