Long-term efficacy and safety of direct oral anticoagulants in venous thrombotic antiphospholipid syndrome patients not candidate to warfarin: A pilot prospective case series study
Daniele Pastori, Danilo Menichelli, Gian Marco Podda, Bianca Clerici, Simone Birocchi, Tommaso Bucci, Paul RJ Ames, Pasquale Pignatelli

TL;DR
This study explores the safety and effectiveness of direct oral anticoagulants in patients with venous thrombotic antiphospholipid syndrome who cannot take warfarin.
Contribution
The study provides preliminary evidence that DOACs may be a viable alternative to warfarin in this specific patient group.
Findings
No recurrent venous thromboembolism or arterial thrombotic events occurred during follow-up.
Four bleeding events, including two major ones, were reported with an incidence rate of 5.3 per 100 patient-years.
No intracranial bleeding was observed among the patients.
Abstract
Data on direct oral anticoagulants (DOACs) in venous thrombotic antiphospholipid antibody syndrome (APS) are controversial. This pilot study aimed to assess the safety and efficacy of DOACs in APS patients requiring oral anticoagulation for venous thromboembolism (VTE) but unsuitable for treatment with vitamin K antagonists (VKAs). We performed a prospective multi-centre case-series including APS patients with previous VTE who were receiving treatment with DOACs due to ineligibility for VKAs. Main outcomes were bleeding, arterial and recurrent venous thrombotic events and all-cause death. We included 18 patients (median age 59.6 years, 66.7% women). The antiphospholipid antibody pattern was single positivity for 33.3% patients, double positivity for 33.3%, and triple positivity for 27.8%. Only one patient had seronegative APS. Apixaban, dabigatran, rivaroxaban and edoxaban were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
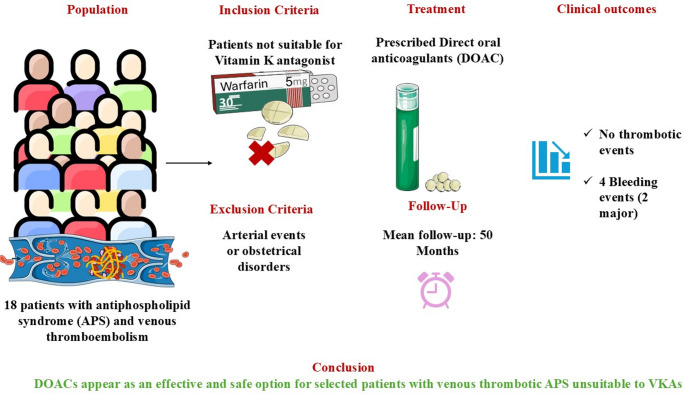 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Systemic Lupus Erythematosus Research · Liver Disease and Transplantation
Introduction
Patients with antiphospholipid antibody syndrome (APS) have an increased risk of venous (VTE) and arterial thromboembolism (ATE); treatment of thrombotic events and prevention of recurrences is mainly based on the administration of oral anticoagulation therapy [1, 2]. Vitamin K antagonists (VKAs), such as warfarin, have long been the standard treatment option for APS patients requiring anticoagulation. However, some patients may experience recurrences of thrombosis despite oral anticoagulation therapy [3], and high-intensity VKA therapy was proven ineffective for the prevention of recurrent VTE [4].
In addition, anticoagulation in APS patients may be challenging for a number of reasons, including the so-called warfarin resistance, the instability of anticoagulation (i.e., low time in therapeutic range, TTR) [5] and the need for frequent INR checks for VKA monitoring and dosing. Furthermore, a significant proportion of warfarin patients discontinue anticoagulation therapy during follow-up [5].
For a long time, the only alternative to VKAs was represented by aspirin, which, however, has uncertain efficacy in preventing VTE [6].
Direct oral anticoagulants (DOACs) are effective and generally safe for managing conditions such as VTE or atrial fibrillation (AF), and they represent an alternative for patients who are unsuitable for VKA therapy [7]. Of note, in patients unsuitable for VKAs, DOACs reduced the risk of thromboembolism without a significant increase of the risk of major bleeding or intracranial haemorrhage compared to aspirin.
Despite the potential advantages of DOACs, their use in patients with APS is controversial particularly following the results of the TRAPS trial, which was stopped for an excess of thrombotic and bleeding events [8]. Nevertheless, this trial’s results were limited to a specific patient subset (triple-positive APS) and included around 20% of patients with a history of arterial events, leaving uncertainty regarding the broader population of APS patients with venous thrombotic events [9].
Currently, there is no solid evidence regarding the safety and efficacy of DOACs in APS patients with single or double antiphospholipid antibodies (aPL) positivity and/or venous thrombotic events only. Current EULAR [9] and British Society Haematology guidelines suggest the use of DOACs as an alternative treatment to VKAs after a shared decision with patients [9]. This study seeks to address this gap by investigating the long-term safety and efficacy of DOACs in APS patients with VTE who not suitable candidates for VKAs are.
Methods
We conducted a prospective, multi-centre case series including patients with APS and previous VTEs (venous thrombotic APS) treated with DOACs because they were unsuitable for VKA therapy. Patients were followed up at the anticoagulation outpatient clinics of the Policlinico Umberto I of Rome and ASST Santi Paolo e Carlo of Milan. The study included patients who fulfilled all the clinical and laboratory diagnostic APS Sydney criteria [10] and had a history of VTE but no arterial thrombotic or obstetric manifestations of APS. Two consecutive positive aPL tests, conducted at least 12 weeks apart, were required for all APS patients. Additionally, aPL levels were reassessed on a yearly basis. Before prescribing DOACs, patients were informed on current data from the literature and on the potential risks and benefits of DOACs for the management of their condition. A signed informed consent was obtained from all patients for clinical data collection. Patients with APS and ATE and/or obstetrical manifestations were excluded.
Comorbidities, concomitant therapy, laboratory tests and, for patients taking VKA before starting DOACs, TTR (using the linear interpolation method of Rosendaal [11]) were collected at baseline.
The study was approved by the Ethical Committee of Sapienza University of Rome (n° 823/17) and was performed according to the ethical guidelines of the 1975 Helsinki Declaration.
Follow-up
After starting DOACs, patients were closely monitored with sequential fibrinogen and D-dimer testing to detect any symptomatic or asymptomatic clotting activation. Patients were regularly seen at the anticoagulation outpatient clinic for the follow-up of DOAC therapy. Patients were treated with long-term anticoagulation due to the permanent risk factor for VTE represented by APS. Records about hospital admissions and complications related to oral anticoagulation therapy (such as bleeding events) were collected during each visit. Bleeding events were classified according to the International Society on Thrombosis and Haemostasis (ISTH) classification [12]. If patients missed 1 or more visits, follow-up was performed by telephone.
Data synthesis
Categorical variables are reported as counts (percentages). Continuous variables are expressed as means with standard deviations or medians with interquartile ranges (IQR), as appropriate. The annual incidence of adverse events was reported as the number of events per 100 patient-years, with 95% confidence intervals, calculated by dividing the total number of events by the total patient follow-up time (in years).
Results
We included 18 patients, 12 of which were female (66.7%). Non-aggregate aPL profile and patient characteristics are reported in Table 1 (description of Methods were reported in the supplementary material). In all patients the clinical indication to oral anticoagulation therapy was VTE, but 3 patients (16.7%) had also concomitant AF.
Table 1. Non-aggregate clinical characteristics of eligible patients with APS and venous thromboembolismPatient #SexAge (years)Auto-antibody positivityComorbiditiesVenous thrombosis site (at diagnosis)1Female58LAC+Hypertension, Parkinson’s diseaseDVT of gastrocnemius and popliteal veins and SVT of lower limb2Male32LAC+NoneMonolateral PE3Male77LAC+Hypertension, atrial fibrillation. Parkinson’s diseaseDVT of lower limb4Female74LAC + aCL + aB2GPI+HypertensionBilateral PE5Female57LAC + aCL + aB2GPI+SmokingDVT of posterior tibial vein6Female57LAC+Hypertension, thrombocytopeniaBilateral DVT of lower limb7Female21LAC+, aCL+NoneBilateral PE8Male63aCL+, aB2GPI+DepressionRecurrent DVT of lower limbs9Male30aCL/ antiVimentin +Smoking, thrombocytopeniaPE with Pulmonary infarction10Female52LAC + aCL + aB2GPI+NoneDVT of gastrocnemius and popliteal veins11Male39LAC + aCL + aB2GPI+HypertriglyceridemiaDVT of cava, femoral, iliac and popliteal veins12Female34LAC+NoneDVT and SVT of lower limb13Female54LAC + aCL + aB2GPI+Hypertension, autoimmune thyroiditis with hypothyroidismBilateral PE and DVT of femoral and popliteal veins14Female61LAC + aB2GPI+SLE and rheumatoid arthtritisBilateral PE and DVT of popliteal and gastrocnemius veins15Female91aCL + aB2GPI+DementiaBilateral PE16Female88aCL + aB2GPI+Hypertension, Atrial fibrillation, rheumatoid arthtritisBilateral PE and DVT of popliteal vein and SVT of lower limb17Female61LAC + aB2GPI+Hypertension, Atrial fibrillation, smoking, autoimmune thyroiditis with hypothyroidismBilateral PE18Male80LAC+SmokingBilateral PE and DVT of popliteal and calf veinsAbbreviations – DVT: deep vein thrombosis, LAC: lupus anticoagulant; aB2GPI: anti-β_2_-Glycoprotein I antibody; aCL anticardiolipin antibody, PE: pulmonary embolism, SLE: systemic lupus erythematosus, SVT: superficial vein thrombosis
Aggregate laboratory values and eligible patients’ clinical characteristics are reported in Table 2. Patients’ median age was 59.6 years (IQR, 38–76). Six out of 18 patients (33.3%) were only lupus anticoagulant (LAC)-positive, 6 (33.3%) had double aPL positivity, 5 (27.8%) had triple aPL positivity, and 1 patient was affected by seronegative APS with anti-cardiolipin/vimentin positivity. None of the patients had moderate-severe kidney disease or a history of chronic liver disease. Mean haemoglobin and platelet count were 13.2 ± 1.67 g/dl and 269.9 ± 140.5 × 10^3^/µL, respectively.
Table 2. Aggregate characteristics of eligible patients with APS and venous thromboembolismVariableValues Clinical characteristics Age (years) – Median and IQR59.6 (38.0-76.2) *Females (%)*66.7 *Hypertension (%)*38.9 *Atrial fibrillation (%)*16.7 *Autoimmune diseases (%)*22.2 *Neurological disorders (%)*16.7 Thrombocytopenia (%)*11.1 *Smoking (%)*16.7 Laboratory test Haemoglobin – Mean and SD13.2 ± 1.67 g/dl Platelet count – Mean and SD269.9 ± 140.5 × 10^3^/µL *Platelet count – Mean and SD (excluding patients with thrombocytopenia)*286.7 ± 141.35 × 10^3^/µL Creatinine – Mean and SD0.95 ± 0.31 mg/dl AST – Median and IQR19.5 (17.8–23.3) ALT – Median and IQR17.5 (11.8–20.8) aPL positivity profile (%) Single positivity Double positivity Triple positivity Seronegative APS33.333.327.85.6 DOAC (%) Apixaban44.4 Dabigatran27.8 Edoxaban11.1 Rivaroxaban16.7 *DOAC as first line of treatment (%)*27.8 *Previous therapy with VKA (%)72.2Abbreviations – IQR: interquartile range; SD: standard deviation; aPL, antiphospholipid antibody; APS: antiphospholipid antibody syndrome; DOAC: direct oral anticoagulant; VKA: vitamin K antagonistmild thrombocytopenia in 2 patients 148.0 × 10^3^/µL and 139.0 × 10^3^/µL
Detailed data on anticoagulation are reported in Table 3. Five out of 18 patients were prescribed a DOAC from the start of anticoagulant treatment. For the remaining 13 patients, the main reasons for switching from VKA/low-molecular-weight heparin (LMWH) to a DOAC were: (1) instability of anticoagulation with VKAs (i.e., TTR < 60%), (2) patients’ unwillingness of undergoing INR monitoring, and (3) recurrent VTE while on VKA/therapeutic LMWH dose. In detail, the reasons for switching were poor TTR in 6 patients (range 19–55%), unwillingness to continue INR monitoring in 5 patients, and recurrent VTE under VKA in 1 patient. Dabigatran was prescribed to 5 patients (27.8%; full dosage in 4 and reduced dosage in 1), apixaban to 8 patients (44.4%), 5 of which were started on apixaban 2.5 mg BID for extended thromboprophylaxis. Rivaroxaban was prescribed to 16.7% of patients (20 mg OD in 2 patients and 10 mg OD in 1 patient). Finally, low dose edoxaban was prescribed to 2 patients (11.1%); no patients received the full dose in our cohort. We monitored patients for adverse outcomes including bleeding, thrombotic events and death. The mean follow-up was 50.1 ± 24.1 months. During the observation period, no VTE relapses or other thrombotic events were recorded. All patients had persistently within normal range D-dimer values during follow-up except for Patient 12, in whom apixaban was increased from 2.5 mg BID to 5 mg BID for an asymptomatic increase of the D-dimer, which returned to normal afterwards. Patient 11, who was initially switched to a DOAC for poor TTR, returned to a VKA for no evidence of thrombus resolution under rivaroxaban. The incidence rate of bleeding in our cohort was 5.3 per 100 patient-years (95% confidence interval [95%CI] 1.4–13.6).
Table 3. Data on anticoagulation, reasons for switching to a DOAC and follow-up dataPatient #DOAC type and dosePrior oral anticoagulation therapyReason for switching to a DOACAdverse eventsTime on VKA before starting DOAC (months)1Dabigatran 150 mg BIDVKARecurrent VTE under VKANone62Dabigatran 150 mg BIDVKAPoor TTR (55%)None363Dabigatran 150 mg BIDVKAPoor TTR (39%)No thrombotic events. minor Hemorrhoidal bleeding. Died for colorectal cancer124Dabigatran 150 mg BIDVKAUnwilling to continue INR monitoring despite good TTR (75%) due to living aloneNone425Apixaban 2.5 mg BIDVKAUnwilling to continue INR monitoring despite good TTR (81%) for reduced mobilityNone486Apixaban 5 mg BIDVKAUnwilling to undergo frequent blood sample collectionNone427Rivaroxaban 20 mg ODVKAUnwilling to undergo frequent blood sample collectionNone68Apixaban 2.5 mg BIDVKAPoor TTR (19%)None489Dabigatran 110 mg BIDNoneUnwilling to undergo frequent blood sample collectionNone010Apixaban 2.5 mg BIDVKAPoor TTR (32%)None611Rivaroxaban 20 mg ODVKAPoor TTR (36%)Return to VKA with good TTR (91%) due to non-resolution of VTE on rivaroxaban1212Apixaban 2.5 mg BIDVKAPoor TTR (56%)Apixaban increased to 5 mg BID for asymptomatic elevation of the D-dimer4413Rivaroxaban 10 mg ODVKARenal angiomyolipoma hematomaNone8614Apixaban 5 mg BIDVKAPoor TTR, patient’s choiceNone4115Edoxaban 30 mg ODNonePatient’s choiceNo thrombotic events. Minor hemorrhoidal bleeding.016Edoxaban 30 mg ODNonePatient’s choiceNo thrombotic events. Major bleeding from the superior mesenteric artery during acute pancreatitis.017Apixaban 5 mg BIDNonePatient’s choiceNone018Apixaban 2.5 mg BIDNonePatient’s choiceNo thrombotic events. Major genitourinary bleeding.0Abbreviations – DOAC: direct oral anticoagulant; BID: bis in die; VKA: vitamin K antagonist; VTE, venous thromboembolism; TTR, time in therapeutic range; OD: once dailyincluding bleeding events, thrombotic events and death
Of the total of 4 bleeding events occurred during follow-up, two were major bleeding events. Patient 16 experienced major bleeding from the superior mesenteric artery during acute pancreatitis while on treatment with edoxaban 30 mg OD, while patient 18 experienced major genitourinary bleeding on apixaban 2.5 BID. We recorded two minor hemorrhoidal bleedings in patients 3 and 15 (on dabigatran 150 mg BID and on edoxaban 30 mg OD, respectively). Patient 3 was eventually diagnosed with a fatal colon cancer. None of the patients died because of APS. Indeed, all the remaining patients are on active thromboprophylaxis with no other complications. No other side effects were registered. All APS patients that experienced bleeding during follow-up had no hepatic and kidney impairment and were not treated with concomitant antiplatelet therapy.
Discussion
Our case series of 18 patients with venous thrombotic APS ineligible to VKAs, proved that DOACs are safe and effective: there were no VTE recurrences nor ATEs. During the mean follow-up of 50.1 months, none of the patients died because of APS-related causes or experienced recurrent VTE or ATE, highlighting the long-term safety and efficacy of DOACs in this specific patient population.
Our results are in line with an analysis from the RE-COVER/RE-COVER II and RE-MEDY trials, which showed a similar safety and efficacy of dabigatran compared to warfarin in patients with VTE and thrombophilia, 20% of whom had APS [9]. However, the safety of DOACs in APS patients remains a matter of debate, especially following the TRAPS trial. two metanalyses showed that the excess of thrombotic risk in APS patients treated with DOACs is due to arterial thrombosis rather than to VTE [13, 14]; however, the length of follow-up of included studies was relatively short (< 2 years) [13, 14]. Our patients were followed for a mean of 4 years, providing useful information on long-term outcomes of APS patients on DOACs for VTE. Our results are coherent with a recent observational study [15] performed on 152 APS patients (66 treated with apixaban) during a median follow-up of 53 months, that showed no difference for recurrence of VTE and major bleeding between apixaban and VKA groups [15].
The clinical management of these patients was at the discretion of the treating physicians and the choice of anticoagulation with DOACs was based on some clinical considerations, as well as on patients’ preferences. Firstly, based on guidelines and on existing literature, the use of DOACs was discussed only with patients with VTE as an indication to oral anticoagulation therapy, while patients with previous ATE were kept on warfarin. In addition, given the high prothrombotic burden of APS and the lack of data on extended anticoagulation in these patients, we decided for most patients to use full dose anticoagulation also beyond the first 6 months after the VTE event. In two cases (patients 5 and 8) we decided to adopt an extended treatment with a low-dose of apixaban after at least 6-months of treatment with VKA according to the extended management suggested by international guidelines [16, 17] and AMPLIFY-EXT trial [18], taking account also the type of venous thrombosis (distal deep vein thrombosis for patient 5) and aPL profile (low-risk profile for patient 8).
The use of low dose extended therapy as apixaban 2.5 mg BID [18] or rivaroxaban 10 mg OD [19] was investigated in two clinical trials and showed a low recurrence of VTE compared to placebo. However, no direct comparison between full and low dose of DOAC was available in VTE patients, especially ones with APS. Recently a small, randomized trial, the ASTRO-APS [20], investigated the use of apixaban 2.5 mg BID compared to VKA in APS patients. Apixaban group had a higher number of ischemic stroke events, while no VTE were registered in both groups. However, the trial was stopped prematurely, and the small sample size did not give strong evidence.
Finally, when possible, we preferred DOACs with double daily administration to minimize the time in which patients are exposed to low through plasma levels.
Moreover, the careful selection of patients was accompanied by close monitoring of D-dimer levels during follow-up. This may partially explain the low rate of thrombotic events we found in our study.
Although the DULCIS trial [21] evaluated the role of D-dimer during follow-up to establish patients with low-risk of VTE recurrence and anticoagulation duration, no data was available on the use of D-dimer for the choice of anticoagulant dose. Furthermore, an asymptomatic rise of D-dimer did not reflect the presence of venous thrombosis, so the clinical choice to increase apixaban dose in patient 12 is still a matter of debate and was not supported by clinical evidence.
During follow up, 4 bleeding events occurred of which 2 were major. Although our data were limited by small sample size, the incidence of 5.3 hemorrhages per 100 patient-year found in our case series is similar to that reported in previous clinical trials on DOAC in patients with VTE.
The results of our study should be read in light of its limitations. Despite the fact that data were collected within a multi-center study, we have a limited sample size underpowered to detect differences in thrombotic and bleeding events with heterogeneous patients, as most patients had single-positive or double-positive APS (66.6%), whereas the number of triple-positive patients was low. In particular, there were no events in triple-positive patients of our cohort, but the low sample did not permit to ensure the effectiveness and safety of DOACs in these patients.
Moreover, no comparisons were made with similar patients prescribed VKA, limiting the strength of the evidence derived regarding DOACs efficacy and safety. The majority of our study population (72.2%) was on treatment with DOACs administered twice daily, thus our findings mainly apply to dabigatran and apixaban. Additionally, the absence of thrombotic events, although encouraging, was likely overestimated due to the low sample size and the exclusion of patients with previous arterial thrombotic events or triple positivity, in which warfarin remains the standard of care [2]. Finally, the majority of patients were enrolled due to unsuitability for VKA, and this may represent a potential selection bias.
In conclusion, currently the use of DOACs should be cautious due to controversies raised by international guidelines [9]. Preliminary findings from this prospective series highlight the potential role of DOACs in venous thrombotic APS patients who are ineligible for VKA therapy. Nevertheless, given the limited sample size and the underrepresentation of high-risk subgroups, such as triple-positive patients, larger studies are necessary to confirm these findings and explore the long-term safety of DOACs across diverse APS profiles.