Optimal enteral feeding after surgery for necrotising enterocolitis: a systematic review
Mythili Chawan, Mehak Gupta, Tatyana Podoprigora, Iain Yardley

TL;DR
This systematic review examines the best enteral feeding strategies for infants after surgery for necrotising enterocolitis (NEC), finding limited high-quality evidence but suggesting early feeding may improve outcomes.
Contribution
The study systematically evaluates post-surgery feeding regimes for NEC infants, highlighting gaps in evidence and potential benefits of early enteral nutrition.
Findings
Three studies showed reduced liver dysfunction with standardized feeding regimes.
Early enteral nutrition was not linked to increased NEC recurrence.
Limited data suggest early feeding may reduce parenteral nutrition dependence and improve growth.
Abstract
To review the evidence for enteral feed modification after surgery for Necrotising Enterocolitis (NEC) and determine the optimal feeding regime for these babies. A systematic review of the Scopus and PubMed databases was carried out. Papers reporting feed regimes in babies following surgery for NEC and reporting at least one clinical outcome were included. The ROBINS-I tool was utilised to evaluate the risk of bias. The search strategy returned 2772 records. After deduplication and screening against the inclusion/exclusion criteria, 11 studies were included in the review. Three studies reported the implementation of a standardised feeding regime; one led to earlier introduction of enteral feed, two found no increase in NEC recurrence and all three saw a reduction in liver dysfunction. There is a paucity of high quality evidence to guide specific post-operative feeding strategies in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
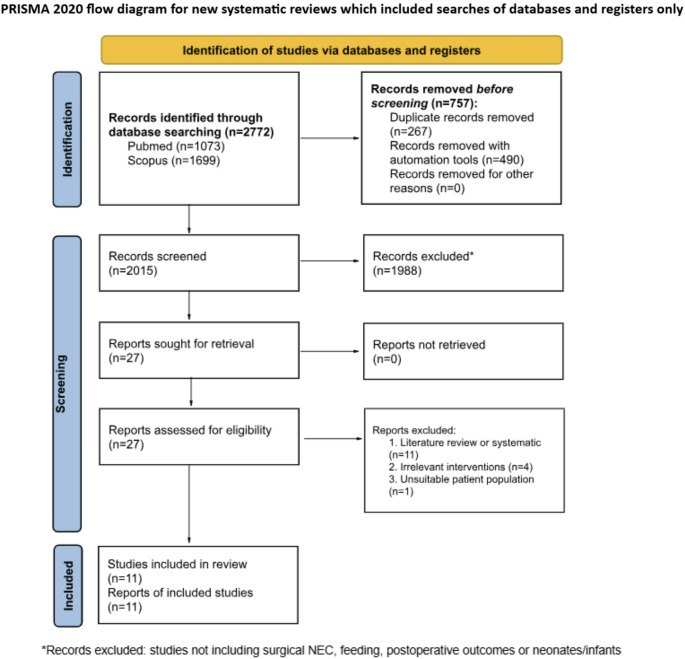 Figure 1
Figure 1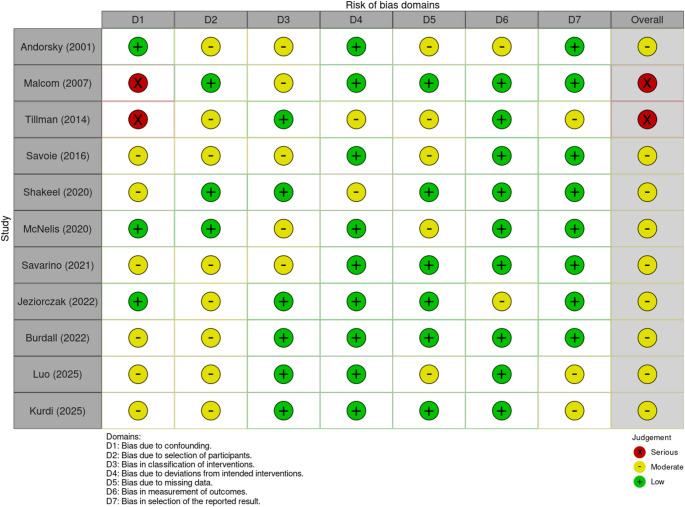 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Nutrition and Health · Clinical Nutrition and Gastroenterology · Breastfeeding Practices and Influences
Introduction
Necrotising enterocolitis (NEC) is a disease affecting predominantly premature infants and is the most common emergency of the gastrointestinal tract occurring in the neonatal period [1]. It is characterised by ischaemia and inflammation of the intestine, resulting in bacterial translocation and later necrosis. Whilst there is uncertainty surrounding the causes of NEC, risk factors include low birth weight, low gestational age, sepsis, respiratory distress and formula feeds [2].
NEC can often be managed with non-operative means, including gut rest and intravenous antibiotics [3]. However, in severe cases surgical intervention is indicated, with intestinal resection and enterostomy formation being the commonest surgical approach [4, 5]. Following surgery, standard practice is to delay the re-initiation of enteral feeds for a period to allow the intestine to recover. In the meantime, parenteral nutrition (PN) is commenced and transition to enteral nutrition (EN) only occurs when deemed safe [6].
Modifications to the enteral nutrition used following surgery for NEC have been suggested, such as lipid or protein supplementation and partially or fully hydrolysed feeds [7, 8]. There is good evidence that breast milk plays a role in reducing the incidence of NEC, but its role and potential benefit to neonates following surgical NEC remains unclear [9]. It is also uncertain at what time point and how rapidly enteral feeds should be reintroduced following surgical NEC. Therefore, we performed a systematic review to identify the evidence for modifying feeds and to determine the optimal feed regime after surgery for NEC.
Methods
Protocol and registration: A systematic review protocol was registered with PROSPERO (CRD42023467607).
Data sources and search strategy: PubMed and Scopus databases were searched on 10/10/2023 and 14/01/2026 using terms including ‘surgical’, ‘feeding’, ‘newborn’, ‘outcomes’ and MeSH terms for ‘necrotising enterocolitis’. The limitations implemented were: English language, articles from 1990-present and human studies. Table 1 summarises the search strategy used. The reference lists of systematic reviews, meta-analyses and included studies were hand-checked for other potentially missed studies.
Table 1. Search strategyDatabases searchedSearch termsLimitsScopusTITLE ( necrotic? ing AND enterocolitis ) AND ( surg* ) AND ( outcome* ) AND ( ( feed* ) OR ( nutrition* ) OR (diet* ) ) AND ( ( neonat* ) OR ( infant* ) OR ( newborn* )) AND ( LIMIT-TO ( LANGUAGE, “English” ) ) AND ( LIMIT-TO ( EXACTKEYWORD, “Human” ) OR LIMIT-TO ( EXACTKEYWORD, “Humans” ) )English languageHuman studiesStudies from 1990-currentPubMed((( “Enterocolitis, Necrotizing”[Mesh])) AND ((feed*) OR (nutrition*) OR (diet*)))English languageHuman studiesStudies from 1990-current
Study selection: duplicates were removed using Mendeley, and remaining results were then title- and abstract-screened by two of three authors (MC, MG or TP) against the inclusion and exclusion criteria shown in Table 2
Table 2. Inclusion and exclusion criteriaInclusion criteriaExclusion criteria● Neonates and infants● Controlled trials and observational studies (case-series, case-control and cohort studies)● Post-necrotising enterocolitis surgery● Reporting an enteral feed intervention● Reporting at least one outcome● Studies not reporting surgical NEC● Systematic reviews and meta-analyses
Full texts of remaining articles were then assessed by three authors (MC, MG, TP) against the aforementioned criteria, with inconsistencies resolved by consensus.
Data extraction and analysis: The data extracted from the included studies are shown in Table 3.
Table 3. Data extractedData extractedAuthorYear of publicationStudy aimStudy settingStudy locationRecruitment methodPopulationInclusion and exclusion criteriaNumber of participantsAge of participants at presentationType/mechanism of feedingPrimary outcomes (recurrence of NEC, mortality, morbidity, neurodevelopmental outcomes, duration of parenteral nutrition)Secondary outcomes (growth measures, time to full enteral feeding, feeding complications, length of hospital stay, biochemical outcomes, e.g. cholestasis)
Quality of included studies: Risk of bias was assessed for all included studies using the Risk of Bias in Non-Randomised studies of interventions (ROBINS-I) tool [10]. The domains assessed were: (1) bias due to confounding, (2) bias in selection of participants into the study, (3) bias in classification of interventions, (4) bias due to deviations from intended interventions, (5) bias due to missing data, (6) bias in measurement of outcomes, (7) bias in selection of the reported result. Studies were classified as being at severe, moderate or low risk of bias, with any inconsistencies resolved by discussion.
Data synthesis and analysis: Where possible, data were extracted from the included articles with the intention of carrying out a meta-analysis where possible.
Results
Study selection: The PRISMA flowchart (Fig. 1) details study selection and numbers included and excluded at each stage. A full record of reasons for exclusion at full-text stage can be found in Supplementary Table 1.
Fig. 1A PRISMA diagram showing the identification of studies
Quality of included studies: A summary of the ROBINS assessment of the relevant studies can be found in Fig. 2. Malcolm et al. scored a low or moderate risk for all domains except bias due to confounding, as they were unable to attribute the increased weight gain of the infants with NEC to ‘increased calories delivered, improved calories absorbed or water weight owing to decreased ostomy losses’ [11]. The retrospective papers were more likely to have a higher risk of bias due to confounding or in the classification of interventions [12–19].
Fig. 2ROBINS-I table for risk of bias assessment of included articles [10]
Study characteristics: Table 4 summarises a description of study characteristics. The papers selected consisted of seven cohort studies and one case series. All studies were retrospective, other than Shakeel et al., where the intervention cohort was prospective but historic controls were used for comparison, and Burdall et al. which is a prospective cohort study [14, 20].
Table 4. Summary of study characteristicsAuthorsDateLocationStudy typeNumber of patientsDirection of studyInterventionsPrimary outcomesSecondary outcomesAndorsky et al. [13]2001United StatesCohort13 with necrotising enterocolitisRetrospectiveEnteral feeding with breast milk and protein hydrolysed formulaDuration of PN use, peak serum direct bilirubin concentrationSuccessful weaning from PN, mortality, need for intestinal transplantMalcolm et al. [11]2007United StatesCase Series9 with necrotising enterocolitis; 1 with isolated intestinal perforationRetrospectiveSoluble dietary fat supplement to enteral feedsOstomy outputDaily weight gainTillman et al. [19]2014United StatesCohort64 with surgical necrotising enterocolitisRetrospectiveImplementation of enteral feeding guidelinesParenteral nutrition duration, nil by mouth duration, parenteral nutrition dependence at 90 days, PNALD incidence, direct bilirubinWeight before and after feeding guidelinesSavoie et al. [18]2016United StatesCohort132RetrospectiveStandardised feed re-introduction regimeTime to full EN after surgeryDays on PN, severity of cholestasis, breast milk useShakeel et al. [20]2020United StatesCohort72 with necrotising enterocolitis; 67 with spontaneous intestinal perforationProspective with historic controlsStandardised feed re-introduction regimeIntestinal failure-associated liver disease incidence (IFALD), time to reach 50% and 100% of energy from enteral nutritionDays on PN, postoperative NEC incidence, length of hospital stayMcNelis et al. [21]2020United StatesCohort33RetrospectiveEnteral feeding advancementDuration of PN use, differences in growth measurements (including weight, height, head circumference)Comparative growth trajectory between surgical NEC and spontaneous intestinal perforation infantsSavarino et al. [15]2021ItalyCohort43RetrospectiveNone - observational onlySurvival rates of preterm infants with NECTime to EN after NEC onset, duration of PN, type of EN and nutritional management descriptive outcomesJeziorczak et al. [12]2022United StatesCohort14RetrospectiveAbility to achieve enteral feedingSurvivalBacterial infection rate, surgical intervention rate, NEC incidence, birth weight and gestational age differencesBurdall et al. [14]2022United KingdomCohort143ProspectiveEarly (< 7 days) vs. Late Enteral FeedingComposite of death before 28 days post-surgery, ongoing need for PN at 28 days post-surgeryAlive and off PN at 28 days, timing of feed reintroductionLuo et al. [16]2025ChinaCohort90RetrospectiveTiming of enteral - early enteral nutrition (EEN, < 7 days) and late enteral nutrition (LEN, ≥ 7 days) nutrition resumptionProgression of EN - faster increase (FI, ≥ 20 ml/kg/d) and slower increase (SI, < 20 ml/kg/d)Method of EN - intact protein formula, special medical formula and mixed feedingParenteral nutrition-associated liver disease, stoma necrosis, bowel obstruction, intestinal stenosis, reoperationLength of stay, parenteral nutrition duration, weight gainKurdi et al. [17]2025Saudi ArabiaCohort500RetrospectiveAbility to achieve enteral nutrition (early (5 days), intermediate (8–14 days), and delayed (≥ 15 days) )Early tolerance of oral intake after surgery, NEC recurrence, need to revert to PNFeeding-related complications, validation of a predictive feeding-readiness scoring system66 out of 132 infants had necrotising enterocolitis
- When is the optimal time to reinitiate enteral feeding?
Several papers emphasise the significance of achieving enteral autonomy following surgical NEC. As expected, McNelis et al. concluded that most of this population have a delay in achieving enteral autonomy, compared to neonates with medical NEC or spontaneous intestinal perforation [21]. Furthermore, Burdall et al. found no effect on mortality or need for parenteral nutrition when re-starting EN less than 7 days post-surgery [14]. Jeziorczak et al. and Savarino et al. both report that the inability to reintroduce EN after surgery for NEC is associated with higher mortality rates [12, 15]. Additionally, both papers report the potential advantages of using breast milk in EN and conclude that it does not harm babies post-surgery for NEC; however, both only report small cohorts, so the broader significance of their findings remains unclear.
Expanding on the literature for timing of initiation of EN, Luo et al. conducted a retrospective study on 90 term infants who developed perforation following NEC which required surgical intervention. It was found that earlier initiation of EN, within seven days of surgery, was significantly associated with reduced incidence of reoperation and intestinal stenosis when compared with later EN initiation. This study also reported that a faster rate of increase of EN, ≥ 20 ml/kg/day, significantly shortened PN duration and length of hospital stay, although this was associated with a slower rate of weight gain. The authors also examined types of EN feed, and it was found that infants fed with an intact protein formula had the quickest speed of advancement and no intestinal stenosis, however there were only two infants in this cohort, so generalisability is limited.
- 2.Are there clinical parameters that predict successful early feeding?
As retrospective or non-randomised studies, although all the above studies supported or at least found no harm from earlier feeding, it is not apparent if the babies fed sooner were systematically different from those fed later, which could account for the differences in outcomes. Kurdi et al. [17] found that early enteral feeding initiated five days after surgery was successfully tolerated in selected infants. The criteria identified as being compatible with earlier feeding included those with limited bowel resection, early stoma function and rapid normalisation of inflammatory markers, all factors that might be expected to be associated with better outcomes. The authors describe a scoring system incorporating these preoperative, intraoperative, and postoperative variables to predict feeding readiness, with no reported cases of recurrent NEC or feeding-related complications.
- 3.What type of milk and feeding advancement protocols are recommended post-operatively?
Two papers reported the effects of modifying the make-up of the enteral feed used following surgical NEC. Andorsky et al. included thirty neonates with short bowel syndrome, 13 following surgery for NEC, but did not segregate results according to diagnosis [13]. They found that enteral feeding with an amino acid-based formula or breast milk was associated with a reduced duration on PN and that supplementing EN with a protein hydrolysate was associated with a lower peak direct bilirubin concentration than EN alone [13]. Malcolm et al., report the effect of dietary lipid supplementation in 10 infants with enterostomies, (9 following surgery for NEC) [11]. They observed a decrease in ostomy output and an increase in daily weight gain after the addition of a soluble dietary fat supplement EN and hypothesise that this is due to the “ileal brake” phenomenon where dietary fats slow transit through the small intestine.
Shakeel et al. and Savoie et al. both report the effect of implementing standardised feeding regimes with a shared primary outcome of time to full EN [18, 20]. Both guidelines involved initiating lipid-based PN immediately after surgery, followed by EN (preferentially with breast milk) in a standardised (but different in the two studies) manner [22]. A meta-analysis of the data in these two studies was considered; however, the lack of granularity in the data and multiple different diagnoses being included made data aggregation and meta-analysis impossible. Table 5 summarises the data from these two studies.
Table 5. Summary of data reported in Savoie et al. [18] and Shakeel et al. [20]Number of participantsSavoie et al. [18]Shakeel et al. [20]n = 132n = 139Control ^a^ (n = 66)Guidelines (n = 66) P NEC (n = 73)SIP (n = 67)Control ^b^ (n = 49)Guidelines (n = 24) P Control ^b^ (n = 38)Guidelines (n = 29) P DiagnosisNEC33331N/AN/AN/AN/AN/AN/AGastroschisis22200.66Atresia11130.62OutcomesPost-operative NEC (%)360.4210130.704871Time to full enteral nutrition (days)16150.8747290.02145360.354Peak direct bilirubin (mg/dL)5.63.90.016.53.50.0194.43.50.391IFALD/PNALD (%)55440.2180580.04773660.597NEC necrotising enterocolitis, SIP spontaneous intestinal perforation, IFALD intestinal failure-associated liver disease, PNALD parenteral nutrition-associated liver disease^a^ Control group had no standardized feeding advancement regimen, and feeding advancement was determined based on individual physician preferences and on individual infant needs^b^ Control group comprised a historical pre-implementation cohort managed before introduction of standardized postoperative feeding guidelines, in whom enteral feeding initiation and advancement were determined by usual clinician practice
Savoie et al. used a standardised feeding guideline that defined initiation, advancement rate and monitoring of enteral feeding after surgery for NEC [18]. Infants were stratified by residual bowel length and weight and assigned to fixed 1, 3 or 7 day advancement pathways with predetermined starting volumes and increments. Shakeel et al. implemented standardised postoperative enteral feeding guidelines for surgical infants that defined early initiation, initial feed volume and daily advancement of feeds [20]. Guidelines recommended starting feeds at 20 mL/kg/day with daily increases of 20 mL/kg/day in the absence of intolerance, with a slower alternative protocol for infants < 1000 g. Feeding tolerance criteria were predefined, and adherence was monitored using timing and volume of initial feeds and advancement rates.
Both papers report the feeding regimes being well-tolerated with no increase in post-operative NEC. Shakeel et al. reported a statistically significant reduction in time to full EN in NEC babies, but this was not seen in the Savoie study. Both studies reported potential liver protection from the standardised feeding regimes with significantly lower peak direct bilirubin levels. Furthermore, there was a lower incidence of IFALD diagnosed in all guideline groups.
Overall, Savoie et al. and Shakeel et al. both advocate for initiation of EN, with Shakeel demonstrating a significant reduction in the time taken to reach full EN. Both studies conclude that the standardised feeding regimen not only provides adequate nutrition for growth but also reduces the incidence of IFALD due to prolonged time on PN. Furthermore, both studies recognise implementing standardised clinical guidelines as feasible and encourages this to achieve improved and consistent care for patients. However, the absence of a contemporaneous control group, the lack of granular data and failure to segregate results according to diagnosis in Shakeel et al., leave the potential for several confounding factors to be at play, which may inflate apparent treatment effects and increase the risk of type I error. Alongside these factors, the small sample size also needs to be considered and the potential for type II errors that cause complications of their approach to go undetected.
Similarly to Savoie et al. and Shakeel et al., Tillman et al. investigated the impact of implementing multidisciplinary EN feeding guidelines in a retrospective before–after study of 64 infants with surgical NEC. After guideline implementation, median PN duration decreased from 106 to 65 days and median time nil by mouth from 29 to 16 days, with fewer infants remaining PN–dependent at 90 days. The incidence of PNALD declined from 73% to 42% and peak direct bilirubin concentrations were lower post-implementation. Interpretation of these findings is limited by the retrospective design, use of historical controls, small sample size, and incomplete data on parenteral nutrition exposure and residual bowel length.
Discussion
We present a systematic review of the current literature on the optimal enteral feed regime following surgery for NEC. All included studies evaluated enteral nutrition following NEC surgery, with no evidence of harm, as evidenced by the absence of recurrent NEC in those that reported this outcome [CHANGE REFERENCE]. There is also some evidence that standardised feeding regimes can be helpful in both achieving enteral feeding and reducing IFALD and PNALD [18–20]. One study suggested earlier initiation of EN, and rapid feed advancement may mitigate long-term surgical complications, this reinforces the observation that standardised feeding regimes do not increase the risk of NEC recurrence and may improve clinical outcomes by reducing PN dependence (18). Furthermore, enteral nutrition after surgical NEC may be guided by objective radiologic, operative and postoperative recovery markers rather than fixed fasting intervals, supporting individualized early feeding strategies that may safely reduce prolonged PN, although prospective validation is required [17].
Ensuring adequate nutrition following surgery for NEC is vital to support adequate growth during a crucial period in a baby’s development. It is already known that babies living with an enterostomy are at significant risk of poor growth [23], but relying on parenteral nutrition creates the risk of liver dysfunction [24]. As babies of even lower gestational age undergo surgery for NEC [25], we can anticipate their living with enterostomies for longer periods, making enteral nutrition following surgery ever more important.
Our finding of no evidence of increased risk of recurrent NEC from enteral feeding following surgery is important and should encourage clinicians to feed babies via their gut sooner after surgery. Manipulating feed content, for example with fat supplements [11], has the potential to maximise enteral intake despite the presence of short gut or an enterostomy.
Prior efforts to systematically review the literature on enteral feeding after NEC has primarily focused on the timing of re-initiation of feeds. Patel et al. evaluated earlier versus later refeeding after NEC, demonstrating no increase in adverse outcomes with earlier initiation [26]. However, their analysis was limited to timing alone and largely included medically managed NEC. In contrast, the present review examines enteral feeding after surgical NEC as a comprehensive post-operative strategy, encompassing multiple aspects of enteral nutrition beyond timing, including feeding protocols, advancement strategies and nutritional outcomes.
Standardised feeding protocols appear to have potential to improve enteral feeding following surgery for NEC. Their use safely allows a more rapid introduction of enteral feeds and provides a framework for clinicians to refer to when managing these fragile patients. The optimum regimen however remains unclear, with differing approaches reported.
Strengths and weaknesses
This is a thorough and reproducible systematic review with a clearly defined search strategy and a standardised screening process involving multiple researchers. We identified ten studies related to our objective and were able to retrieve full texts of all papers. A risk of bias assessment was conducted, with most articles being of low or moderate risk of bias.
However, the cohorts reported were heterogeneous, with little segregation of babies treated surgically for NEC from other diagnoses such as SIP, making the direct application of findings to surgical NEC babies unclear and an aggregated analysis impossible. In addition, surgical NEC cohorts themselves were heterogeneous, with limited differentiation between infants managed with enterostomy and those without diversion, despite these subgroups having potentially different postoperative feeding trajectories. Stratified analysis by stoma status was therefore not possible due to limited reporting in the literature and should be addressed in future studies. Almost all studies were retrospective and uncontrolled, with only two being prospective. No study included a contemporaneous comparator to their intervention, the single study that did report a control group used historical controls, making the risk of confounding significant.
Future work
There is currently a lack of evidence to guide the enteral nutrition of infants following surgery for NEC. Further work is needed, ideally in the form of randomised or otherwise controlled trials, but if these are not felt to be feasible, then large-scale, multi-centre, prospective studies would be a useful addition. The application of standardised feeding regimes seems the most promising intervention to study. Core outcome sets for NEC [27] should be used to ensure consistent reporting across studies.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gephart SM, Mc Grath JM, Effken JA, Halpern MD (2012) Necrotizing enterocolitis risk: state of the science. Adv Neonatal Care 12(2):77–87; quiz 88–89. 10.1097/ANC.0b 013e 31824 cee 9410.1097/ANC.0b 013e 31824 cee 94PMC 335763022469959 · doi ↗ · pubmed ↗
- 2Christian VJ, Polzin E, Welak S (2018) Nutrition management of necrotizing enterocolitis. Nutrition in clinical practice, vol 33. John Wiley and Sons Inc, pp 476–482. 4 10.1002/ncp.1011510.1002/ncp.1011529940075 · doi ↗ · pubmed ↗
- 3Altobelli E, Angeletti PM, Verrotti A, Petrocelli R (2020) The impact of human milk on necrotizing enterocolitis: a systematic review and meta-analysis. Nutrients. 10.3390/nu 1205132210.3390/nu 12051322 PMC 728442532384652 · doi ↗ · pubmed ↗
- 4Cochrane Methods (2025) Risk of Bias in Non–Randomized Studies – of Interventions (ROBINS–I). https://methods.cochrane.org/bias/risk-bias-non-randomized-studies-interventions
- 5Vallant N, Haffenden V, Peatman O, Khan H, Lee G, Thakkar H, Yardley I (2022) Outcomes for necrotising enterocolitis (NEC) in babies born at the threshold of viability: a case-control study. BMJ Paediatrics Open. 10.1136/bmjpo-2022-00158310.1136/bmjpo-2022-001583 PMC 971731736645754 · doi ↗ · pubmed ↗