Sex-disparate safety profile of Obinutuzumab: a pharmacovigilance analysis using the FDA adverse event reporting system
Zhixun Bai, Jiaxi Chen, Yongping Lan, Houze Li, Rubin Zheng, Miao Deng, Wenyi Pang

TL;DR
This study finds that Obinutuzumab, a cancer drug, poses higher safety risks for women, particularly for certain blood disorders and rare conditions like pure red cell aplasia.
Contribution
The study identifies sex-specific adverse event signals for Obinutuzumab, including novel risks like pure red cell aplasia and enteroviral meningitis in women.
Findings
Women experience higher risks of severe hematologic toxicities with Obinutuzumab compared to men.
Novel adverse event signals for pure red cell aplasia and enteroviral meningitis were found exclusively in female patients.
Blood and lymphatic system disorders showed the strongest adverse event signals in both genders.
Abstract
•Obinutuzumab safety evaluated using FAERS data from 2013–2024.•Blood and lymphatic disorders show the highest signal strength in both sexes.•Women show a higher risk of severe hematologic toxicities with Obinutuzumab.•Novel signals for pure red cell aplasia and enteroviral meningitis in women. Obinutuzumab safety evaluated using FAERS data from 2013–2024. Blood and lymphatic disorders show the highest signal strength in both sexes. Women show a higher risk of severe hematologic toxicities with Obinutuzumab. Novel signals for pure red cell aplasia and enteroviral meningitis in women. Obinutuzumab, a type II anti‐CD20 monoclonal antibody used for treating B-cell hematologic malignancies, improves outcomes and prolongs progression-free survival. However, its use is linked to adverse reactions that vary by gender. This study aims to assess adverse event signals related to Obinutuzumab…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
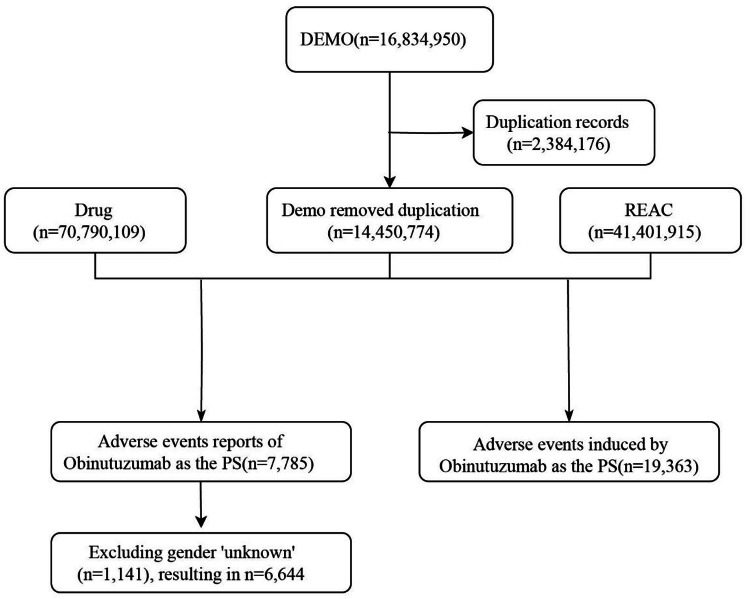 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · HER2/EGFR in Cancer Research · Inflammatory mediators and NSAID effects
Introduction
Obinutuzumab is a type II anti-CD20 monoclonal antibody,1 primarily used for the treatment of B-cell-related hematologic and lymphatic malignancies, such as non-Hodgkin lymphoma and chronic lymphocytic leukemia.2^,^3 In clinical trials, Obinutuzumab, when used in combination with other targeted therapies, typically demonstrates a significant improvement in treatment outcomes and progression-free survival. For example, the combination of Venetoclax and Obinutuzumab has been shown to significantly improve survival rates in previously untreated chronic lymphocytic leukemia patients.4
Obinutuzumab was first approved by the FDA in 2013 for the treatment of chronic lymphocytic leukemia and later received approval for other types of non-Hodgkin lymphoma. Currently, Obinutuzumab has become a key drug in the treatment regimens for many hematologic and lymphatic malignancies.5, 6, 7 However, the use of Obinutuzumab appears to be associated with a higher risk of adverse reactions. A randomized, controlled phase 3 trial in chronic lymphocytic leukemia showed that the incidence of adverse events was higher in the Obinutuzumab combination therapy group.8 Furthermore, multiple studies have similarly indicated that while adding Obinutuzumab improves efficacy, it also increases the risk of adverse events.5^,^9^,^10
The FDA Adverse Event Reporting System (FAERS) is one of the largest drug safety databases in the world, used to collect and analyze Adverse Drug Events (ADEs) related to drug use.11 This database provides an opportunity to explore the potential ADEs of Obinutuzumab. This study aims to retrospectively review the data on Obinutuzumab from the FAERS database between the fourth quarter of 2013 and the fourth quarter of 2024, evaluating the occurrence of drug-related adverse events to promote the rational use of clinical medications.
Methods
Data source and preprocessing
Considering the market launch of Obinutuzumab, this study downloaded the American Standard Code for Information Interchange (ASCII) report files from the FAERS database for the period from the fourth quarter of 2013 to the fourth quarter of 2024,12 and processed the data using the R language. Drug names were standardized using Medex UIMA 1.3.8,13 and adverse event classification was performed using MedDRA version 26.1.14 Duplicate reports were removed, and in cases with the same CASEID, only the report with the most recent date was retained.15
Data extraction and analysis
Reports related to Obinutuzumab as the primary drug associated with Adverse Drug Events (ADEs) were extracted, covering information such as the report date, patient age and gender, reporter, and region. After preprocessing, this study obtained 14,450,774 report records, 70,790,109 drug cases, and 41,401,915 REAC records (Fig. 1).Fig. 1. The flow diagram of selecting Obinutuzumab-related ADEs from FAERS database.Fig 1 dummy alt text
This study used the Reporting Odds Ratios (ROR) and Proportional Reporting Ratios (PRR) from disproportionality analysis to assess Adverse Drug Event (ADE) signals. To ensure the comprehensiveness and accuracy of the results, the study stratified by gender, separately evaluating the ROR and PRR values for male and female patients. The advantage of ROR lies in its ability to correct for biases caused by low report volumes of certain events. Compared to ROR, the advantage of PRR is its higher specificity. This study employed both ROR and PRR methods to leverage their respective strengths, aiming to detect more reliable safety signals.
Statistical analysis
The ROR and PRR are based on Table 1, where a ≥ 3, ROR 95% CI (lower limit) > 1, and PRR 95% CI (lower limit) ≥ 1 are considered as positive ADE signals.16 The higher the ROR and PRR values, the stronger the ADE signal. The drug retrieval information for this study is provided in Supplementary 1.
Table 1. Four grid table.Table 1 dummy alt textObinutuzumab-related ADEsNon-Obinutuzumab-related ADEsTotal****Obinutuzumababa + bNon-Obinutuzumabcdc + dTotala + cb + dN = a + b + c + d
Data analysis was conducted using R (version 4.4.2), and the flowchart was created using draw.io software. This study was conducted following the STROBE guidelines.
Results
Basic characteristics of Obinutuzumab-related ADEs
In the adverse event reports related to Obinutuzumab, the number of male patients (59.23%) was significantly higher than that of female patients (40.77%). Among the reports with clear age data, the most common adverse events were reported in patients over 45-years-old, with fewer reports from those under 45. The majority of reports (67.99%) were from physicians, which increased the reliability of the ADEs information. Reports came from several countries and regions, including the United States (25.86%), Japan (15.58%), China (9.87%), France (7.10%), and Australia (2.97%). In terms of clinical outcomes, hospitalization was the most common (43.19%), followed by other serious outcomes (37.80%) and death (12.32%). Detailed information can be found in Table 2.Table 2. Basic information on ADEs related to Obinutuzumab from the FAERS database.Table 2 dummy alt text**Factors****Total events (%)****Female (%)****Male (%)**Year20138 (0.12)4 (50)4 (50)2014162 (2.44)71 (43.83)91 (56.17)2015293 (4.41)129 (44.03)164 (55.97)2016536 (8.07)215 (40.11)321 (59.89)2017607 (9.14)221 (36.41)386 (63.59)2018561 (8.44)201 (35.83)360 (64.17)2019458 (6.89)188 (41.05)270 (58.95)2020576 (8.67)213 (36.98)363 (63.02)2021455 (6.85)195 (42.86)260 (57.14)2022822 (12.37)328 (39.9)494 (60.1)2023859 (12.93)361 (42.03)498 (57.97)20241307 (19.67)583 (44.61)724 (55.39)2013‒202466442709 (40.77)3935 (59.23)Age (year)< 1820 (0.30)7 (35)13 (65)18‒45399 (6.01)212 (53.13)187 (46.87)45‒651799 (27.08)754 (41.91)1045 (58.09)≥ 653149 (47.40)1236(39.25)1913 (60.75)Unknow1277 (19.22)500(39.15)777 (60.85)Weight (kg)70.00 (60.00, 83.00)62.00 (54.00, 71.00)77.00 (67.30, 88.00)ReporterPhysician4517 (67.99)1873 (41.47)2644 (58.53)Pharmacist1329 (20.00)527 (39.65)802 (60.35)Consumer397 (5.98)173 (43.58)224 (56.42)Other health-professional382 (5.75)130 (34.03)252 (65.97)Unknown19 (0.29)6 (31.58)13 (68.42)Reported countriesUnited states1718 (25.86)661 (38.47)1057 (61.53)Japan1035 (15.58)472 (45.6)563 (54.4)Other849 (12.78)355 (41.81)494 (58.19)China656 (9.87)298 (45.43)358 (54.57)France472 (7.10)190 (40.25)282 (59.75)Germany424 (6.38)144 (33.96)280 (66.04)Italy306 (4.61)125 (40.85)181 (59.15)United Kingdom227 (3.42)97 (42.73)130 (57.27)Australia197 (2.97)90 (45.69)107 (54.31)Russia117 (1.76)50 (42.74)67 (57.26)Canada108 (1.63)31 (28.7)77 (71.3)Spain101 (1.52)40 (39.6)61 (60.4)Poland90 (1.35)42 (46.67)48 (53.33)Brazil89 (1.34)32(35.96)57 (64.04)Israel88 (1.32)27 (30.68)61 (69.32)Switzerland61 (0.92)13 (21.31)48 (78.69)Greece54 (0.81)18 (33.33)36 (66.67)Korea, south52 (0.78)24 (46.15)28 (53.85)RouteIntravenous4377 (65.88)1769 (40.42)2608 (59.58)Other1367 (20.57)544 (39.8)823 (60.2)Intravenous drip900 (13.55)396 (44)504 (56)OutcomesHospitalization2790 (43.19)1109 (39.75)1681 (60.25)Other serious2442 (37.80)1015 (41.56)1427 (58.44)Death796 (12.32)274 (34.42)522 (65.58)Life threatening341 (5.28)129 (37.83)212 (62.17)Disability72 (1.11)30 (41.67)42 (58.33)Required intervention to prevent permanent impairment/damage18 (0.28)4 (22.22)14 (77.78)Congenital anomaly1 (100.00)1 (100)Adverse event occurrence time (days)< 71544 (33.54)639 (41.39)905 (58.61)7‒28506 (10.99)229 (45.26)277 (54.74)28‒60297 (6.45)122 (41.08)175 (58.92)≥ 601318 (28.63)503 (38.16)815 (61.84)Unknow939 (20.40)386 (41.11)553 (58.89)
Obinutuzumab signal mining
This study found that adverse reactions associated with Obinutuzumab involved 23 System Organ Classes (SOCs). The results showed that eight systems had both ROR 95% CI (lower limit) > 1 and PRR 95% CI (lower limit) ≥ 1. The most common and strongest signal was observed in blood and lymphatic system disorders [N_male_ = 956, ROR_male_ = 5.31 (95% CI: 4.97‒5.68), PRR_male_ = 4.89 (95% CI: 4.61‒5.19); N_female_ = 765, ROR_female_ = 8.62 (95% CI: 7.99‒9.29), PRR_female_ = 7.77 (95% CI: 7.33-8.24)]. The next most significant systems were infections and infestations [N_male_ = 1316, ROR_male_ = 2.56 (95% CI: 2.42‒2.71), PRR_male_ = 2.35 (95% CI: 2.22‒2.49); N_female_ = 911, ROR_female_ = 2.53 (95% CI: 2.36‒2.71), PRR_female_ 2.32 (95%CI: 2.19‒2.46)) and immune system disorders (N_male_ = 214, ROR_male_ = 2.27 (95% CI: 1.98‒2.60), PRR_male_ = 2.24 (95% CI: 1.95‒2.57); N_female_ = 155, ROR_female_ = 1.69 (95% CI: 1.44‒1.98), PRR_female_ = 1.67 (95% CI: 1.43‒1.95)] (Table 3).Table 3. The signal strength of ADEs of Obinutuzumab at the SOC level in FAERS database.Table 3 dummy alt text**System organ classMale case reportsMale ROR (95% CI)****Male PRR (95% CI)Female case reportsFemale ROR (95% CI)****Female PRR (95% CI)**Blood and lymphatic system disorders9565.31 (4.97, 5.68)4.89 (4.61, 5.19)7658.62 (7.99, 9.29)7.77 (7.33, 8.24)Infections and infestations13162.56 (2.42, 2.71)2.35 (2.22, 2.49)9112.53 (2.36, 2.71)2.32 (2.19, 2.46)Immune system disorders2142.27 (1.98, 2.6)2.24 (1.95, 2.57)1551.69 (1.44, 1.98)1.67 (1.43, 1.95)Investigations10181.63 (1.52, 1.73)1.56 (1.47, 1.65)6981.85 (1.72, 2.01)1.77 (1.64, 1.91)Hepatobiliary disorders1541.57 (1.34, 1.84)1.56 (1.33, 1.82)1072.04 (1.69, 2.47)2.03(1.67, 2.47)Vascular disorders3811.71 (1.55, 1.9)1.69 (1.53, 1.86)2041.55 (1.34, 1.78)1.53 (1.33, 1.75)Cardiac disorders4211.48 (1.34, 1.63)1.46 (1.32, 1.61)2111.6 (1.39, 1.83)1.58(1.38, 1.81)Respiratory, thoracic and mediastinal disorders7291.51 (1.4, 1.63)1.47 (1.36, 1.59)4931.49 (1.36, 1.64)1.46 (1.35, 1.58)Metabolism and nutrition disorders2420.98 (0.87, 1.12)0.98 (0.87, 1.1)1401.03 (0.87, 1.22)1.03 (0.88, 1.2)Neoplasms benign, malignant and unspecified (incl cysts and polyps)3620.97 (0.87, 1.08)0.97 (0.88, 1.07)1761.11 (0.96, 1.29)1.11 (0.97, 1.27)General disorders and administration site conditions14830.83 (0.79, 0.88)0.86 (0.83, 0.89)10340.75 (0.71, 0.81)0.79 (0.74, 0.84)Gastrointestinal disorders5840.71 (0.65, 0.77)0.73 (0.67, 0.79)4790.74 (0.67, 0.81)0.76 (0.7, 0.82)Injury, poisoning and procedural complications7090.65 (0.61, 0.71)0.68 (0.63, 0.74)5660.73 (0.67, 0.8)0.75 (0.69, 0.81)Renal and urinary disorders1540.61 (0.52, 0.72)0.62 (0.53, 0.73)640.61 (0.48, 0.79)0.62 (0.49, 0.78)Skin and subcutaneous tissue disorders3050.61 (0.54, 0.68)0.62 (0.55, 0.7)2560.56 (0.49, 0.63)0.57 (0.51, 0.64)Nervous system disorders4300.52 (0.47, 0.57)0.54 (0.49, 0.6)3620.59 (0.53, 0.65)0.61 (0.55, 0.67)Ear and labyrinth disorders150.36 (0.22, 0.6)0.36 (0.22, 0.6)130.39 (0.22, 0.66)0.39 (0.23, 0.68)Endocrine disorders90.32 (0.17, 0.62)0.32 (0.17, 0.61)40.22 (0.08, 0.58)0.22 (0.08, 0.59)Musculoskeletal and connective tissue disorders1200.26 (0.21, 0.31)0.26 (0.22, 0.31)1350.3 (0.25, 0.35)0.31 (0.26, 0.37)Eye disorders580.32 (0.25, 0.42)0.33 (0.26, 0.43)250.16 (0.11, 0.23)0.16 (0.11, 0.24)Reproductive system and breast disorders130.18 (0.1, 0.31)0.18 (0.1, 0.31)130.21 (0.12, 0.36)0.21 (0.12, 0.36)Psychiatric disorders1090.17 (0.14, 0.2)0.17 (0.14, 0.21)670.18 (0.14, 0.23)0.19 (0.15, 0.24)Congenital, familial and genetic disorders50.17 (0.07, 0.4)0.17 (0.07, 0.41)
At the PT level, excluding results with unknown gender, our study identified a total of 147 PTs, with detailed information available in Supplementary 2. Based on the ROR rankings, Table 4 displays the top 30 PTs for different gender groups. The results revealed PTs with high signal strength, such as myelosuppression [N_male_ = 162, ROR = 32.5 (95% CI: 27.78‒38.02), PRR = 31.98 (95% CI: 27.34‒37.41); N_female_=136, ROR = 43.95 (95% CI: 37.05‒52.14), PRR = 43.10 (95% CI: 36.13‒51.41)], pure red cell aplasia [N_female_ = 5, ROR = 23.67 (95% CI: 9.82‒57.06), PRR = 31.98 (95% CI: 9.79‒57.13)], and febrile neutropenia [N_female_ = 123, ROR = 22.97(95% CI: 19.21‒27.47), PRR = 22.58 (95% CI: 18.93‒26.94)]. The most common events included infusion-related reactions, myelosuppression, tumor lysis syndrome, and febrile neutropenia. In addition to the aforementioned results, this study also found that lymphoma transformation, follicular lymphoma, and chronic lymphocytic leukemia recurrence showed high signal strengths in both genders. Notably, although meningitis enteroviral occurred less frequently, its signal strength was the highest and it occurred exclusively in females.Table 4. The top 30 signal strength of adverse events of Obinutuzumab ranked by ROR at the PTs level in FAERS database.Table 4 dummy alt text**SocPtMale case reports****Male ROR (95% CI)****Male PRR (95% CI)Female case reportsFemale ROR (95% CI)****Female PRR (95% CI)**Blood and lymphatic system disordersMyelosuppression16232.5 (27.78, 38.02)31.98 (27.34, 37.41)13643.95 (37.05, 52.14)43.1 (36.13, 51.41)Blood and lymphatic system disordersAplasia pure red cell523.67 (9.82, 57.06)23.65 (9.79, 57.13)Blood and lymphatic system disordersFebrile neutropenia12322.97 (19.21, 27.47)22.58 (18.93, 26.94)Infections and infestationsPost-acute COVID-19 syndrome1369.42 (39.77, 121.2)69.33 (40.05, 120.02)1690.3 (54.93, 148.45)90.09 (55.19, 147.06)Infections and infestationsCytomegalovirus chorioretinitis2243.91 (28.71, 67.15)43.81(28.46, 67.43)13128.12 (73.59, 223.05)127.88 (73.87, 221.38)Infections and infestationsCytomegalovirus enterocolitis842.06 (20.82, 85)42.03 (20.75, 85.11)7129.48 (60.83, 275.58)129.35 (60.23, 277.81)Infections and infestationsCOVID-19 pneumonia9729.08 (23.76, 35.59)28.8 (23.67, 35.04)4430.68 (22.78, 41.32)30.49 (22.72, 40.91)Infections and infestationsNeutropenic infection434.78 (12.89, 93.81)34.77 (12.8, 94.48)Infections and infestationsPneumonia haemophilus332.5 (10.35, 102.11)32.49 (10.42, 101.26)Infections and infestationsCampylobacter infection525.99 (10.73, 62.96)25.98 (10.75, 62.76)Infections and infestationsHepatitis viral324.28 (7.75, 76.04)24.28 (7.79, 75.68)Infections and infestationsPneumococcal sepsis320.12 (6.44, 62.9)20.11 (6.45, 62.68)Infections and infestationsHaemophilus infection419.84 (7.39, 53.24)19.83 (7.44, 52.84)Infections and infestationsCampylobacter gastroenteritis319.29 (6.17, 60.3)19.29 (6.19, 60.12)Infections and infestationsMeningitis enteroviral3501.91 (149.11, 1689.45)501.69 (148.83, 1691.18)Infections and infestationsSuperinfection bacterial346.69 (14.94, 145.94)46.67 (14.97, 145.46)Infections and infestationsEnterocolitis infectious341.83 (13.39, 130.63)41.81 (13.41, 130.31)Infections and infestationsCytomegalovirus infection3527.8 (19.91, 38.8)27.66 (19.82, 38.6)Infections and infestationsPneumonia cytomegaloviral325.94 (8.33, 80.8)25.93 (8.32, 80.82)Infections and infestationsCytomegalovirus colitis422.77 (8.51, 60.88)22.75 (8.54, 60.62)Neoplasms benign, malignant and unspecified (incl cysts and polyps)Lymphoma transformation10134.23 (70.15, 256.86)134.1 (70.23, 256.05)4191.23 (69.8, 523.93)191.12 (70.34, 519.31)Neoplasms benign, malignant and unspecified (incl cysts and polyps)Follicular lymphoma21121.44 (77.73, 189.73)121.18 (77.21, 190.2)19352.06 (219.32, 565.13)351.09 (219.34, 561.97)Neoplasms benign, malignant and unspecified (incl cysts and polyps)Chronic lymphocytic leukaemia recurrent14115.44 (66.92, 199.13)115.28 (66.59, 199.57)5170.77 (69.5, 419.57)170.64 (69.27, 420.38)Neoplasms benign, malignant and unspecified (incl cysts and polyps)B-cell lymphoma recurrent433.74 (12.51, 90.97)33.72 (12.41, 91.62)5160.91 (65.58, 394.87)160.8 (65.27, 396.14)Neoplasms benign, malignant and unspecified (incl cysts and polyps)Richter's syndrome1141.57 (22.81, 75.74)41.52 (22.61, 76.23)474.78 (27.75, 201.49)74.74 (27.51, 203.08)Neoplasms benign, malignant and unspecified (incl cysts and polyps)Tumor flare324.42 (7.8, 76.49)24.42 (7.84, 76.11)Neoplasms benign, malignant and unspecified (incl cysts and polyps)Metastatic squamous cell carcinoma322.36 (7.14, 69.95)22.35 (7.17, 69.66)InvestigationsCytomegalovirus test positive1229.99 (16.93, 53.15)29.96 (16.97, 52.89)539.38 (16.3, 95.12)39.35 (16.29, 95.06)InvestigationsProcalcitonin increased516.38 (6.78, 39.56)16.37 (6.78, 39.55)327.13 (8.71, 84.53)27.12 (8.7, 84.53)InvestigationsHuman rhinovirus test positive333.53 (10.67, 105.4)33.52 (10.75, 104.47)InvestigationsBlood immunoglobulin g decreased720.25 (9.6, 42.72)20.24 (9.61, 42.63)InvestigationsLymphocyte count decreased5517.52 (13.42, 22.88)17.43 (13.25, 22.93)InvestigationsCd4 lymphocytes decreased968.97 (35.63, 133.5)68.88 (35.37, 134.12)Immune system disordersHypogammaglobulinaemia2117.35 (11.28, 26.69)17.31(11.25, 26.64)1529.04 (17.46, 48.31)28.98 (17.41, 48.24)Immune system disordersSecondary immunodeficiency423.48 (8.74, 63.07)23.47 (8.81, 62.53)Immune system disordersCytokine release syndrome3628.03 (20.18, 38.95)27.89 (19.99, 38.92)Respiratory, thoracic and mediastinal disordersObliterative bronchiolitis872.2 (35.83, 145.52)72.12 (35.61, 146.05)Respiratory, thoracic and mediastinal disordersOrganising pneumonia1022.51 (12.08, 41.94)22.48 (12.01, 42.09)Metabolism and nutrition disordersTumor lysis syndrome9543.37 (35.32, 53.24)42.95 (35.31, 52.25)4481.37 (60.28, 109.84)80.86 (60.26, 108.5)Metabolism and nutrition disordersHyperphosphataemia818.15 (9.04, 36.47)18.14 (8.96, 36.73)General disorders and administration site conditionsVaccination failure527.21 (11.28, 65.63)27.19 (11.26, 65.68)General disorders and administration site conditionsHyperpyrexia1024.88 (13.35, 46.37)24.85 (13.27, 46.53)Vascular disordersHyperaemia619.57 (8.74, 43.81)19.56 (8.76, 43.69)Skin and subcutaneous tissue disordersPrurigo345.22 (14.47, 141.31)45.2 (14.5, 140.88)Injury, poisoning and procedural complicationsInfusion related reaction26633.05 (29.22, 37.38)32.18 (28.61, 36.2)20427.11 (23.57, 31.18)26.34 (22.96, 30.21)
Discussion
Obinutuzumab is a type II glycoengineered anti-CD20 monoclonal antibody initially developed to overcome resistance to rituximab in B-cell malignancies. Studies have shown that it is superior to rituximab in the treatment of hematologic malignancies, such as B-cell lymphoma.17 Obinutuzumab is primarily administered via intravenous infusion, where it specifically binds to the CD20 antigen on the surface of B-cells and kills target cells through multiple mechanisms, such as Antibody-Dependent Cell-Mediated Cytotoxicity (ADCC) and Antibody-Dependent Cellular Phagocytosis (ADCP).18^,^19 Unlike type I anti-CD20 antibodies (such as Rituximab), Obinutuzumab effectively induces direct cell death but does not target the antigen-antibody complex to lipid rafts, resulting in lower Complement-Dependent Cytotoxicity (CDC).18 Additionally, due to the afucosylation of its Fc region and the optimized conformation of its hinge region, Obinutuzumab enhances direct cell death induction and ADCC activity.18^,^20 In a previous randomized phase II clinical trial (GAGE), the efficacy of monotherapy with Obinutuzumab in treating Chronic Lymphocytic Leukemia (CLL) patients and the dose optimization were investigated. The results demonstrated significant efficacy for Obinutuzumab in untreated CLL patients.21 A more recent clinical trial found that combination therapy with Obinutuzumab showed better treatment outcomes in patients with relapsed/refractory chronic lymphocytic leukemia.22 Overall, the efficacy of Obinutuzumab in treating B-cell-related malignancies has been well-established. Furthermore, in recent years, the therapeutic effects of Obinutuzumab in autoimmune-related diseases, such as lupus, rheumatoid arthritis, and primary membranous nephropathy, have also gained increasing recognition.23^,^24 Clinically, the most common adverse reactions to this drug include Infusion-Related Reactions (IRRs) and neutropenia, which are typically associated with severe toxicity.8^,^25 The use of Obinutuzumab is also expanding, with applications in conditions like lupus nephritis, antiphospholipid syndrome, and ANCA-associated vasculitis.26, 27, 28 However, there is still limited understanding of the adverse reactions associated with Obinutuzumab. With the increasing diversity of its applications, monitoring its real-world usage and adverse events to ensure its safety and efficacy is crucial. This study systematically evaluated the adverse reactions related to Obinutuzumab by deeply mining the FAERS database from the fourth quarter of 2013 to the fourth quarter of 2024, providing valuable safety information and revealing new potential risks. This data supports medical practice and the rational use of the drug.
This study observed that reports of adverse events related to Obinutuzumab were more common in male patients than in female patients. It is noteworthy that in blood and lymphatic system disorders, the ROR value (8.62, 95% CI: 7.99‒9.29) and PRR value (7.77, 95% CI: 7.33‒8.24) for female patients were significantly higher than the ROR value (5.31, 95% CI: 4.97‒5.68) and PRR value (4.89, 95% CI: 4.61‒5.19) for male patients, indicating that females may face a higher risk when using Obinutuzumab. Since the majority of adverse event reports (67.99%) were submitted by physicians, the credibility of the results presented is high.
As a monoclonal antibody, the most common adverse event associated with Obinutuzumab is Infusion-Related Reactions (IRRs), which are linked to the drug's high affinity for FcγRIII. Obinutuzumab tightly binds to CD20, triggering FcγR activation, leading to the recruitment of effector cells and a strong release of cytokines, resulting in clinical symptoms.25 Neutropenia and tumor lysis syndrome are also common adverse reactions.29^,^30 At the PT level, in addition to myelosuppression and febrile neutropenia, this study also identified pure red cell aplasia, which is not mentioned in the drug labeling. Although there were only 5 female patients, the ROR value reached 23.67 (95% CI: 9.82‒57.06) and the PRR value reached 23.65 (95% CI: 9.79‒57.13), indicating the need for further attention and investigation. Additionally, PTs such as post-acute COVID-19 syndrome, cytomegalovirus chorioretinitis, cytomegalovirus enterocolitis, COVID-19 pneumonia, and enteroviral meningitis also showed high signal strength, especially enteroviral meningitis, which had the highest ROR and PRR values, with ROR at 501.91 (95% CI: 149.11‒1689.45) and PRR at 501.69 (95% CI: 148.83‒1691.18), and it occurred exclusively in female patients. A recent case report mentioned two female patients receiving Obinutuzumab treatment who developed disseminated enteroviral infections. One patient tested positive for enterovirus in the cerebrospinal fluid through PCR, and both patients' symptoms improved rapidly after discontinuing Obinutuzumab and administering 0.8 g/kg of intravenous immunoglobulin.31 Furthermore, a phase 3 randomized controlled trial found that infections associated with COVID-19 were more severe in the Obinutuzumab group.10 A recent report also mentioned the occurrence of cytomegalovirus enterocolitis after Obinutuzumab combined with bendamustine treatment.32 These findings are consistent with our conclusions.
This study found that pure red cell aplasia and enteroviral meningitis related to Obinutuzumab occurred exclusively in female patients. The occurrence of pure red cell aplasia in female patients may involve complex interactions between different gender-related immune system regulation, erythropoiesis regulation mechanisms, or cytokine release patterns. Although there is currently insufficient evidence to suggest that Obinutuzumab treatment is more likely to cause pure red cell aplasia in female patients, these findings warrant further clinical research and data analysis to reveal the potential impact of gender differences on drug-related adverse reactions. During Obinutuzumab treatment, a recent case report confirmed the detection of enterovirus in the cerebrospinal fluid of some female patients, and their clinical condition rapidly improved after discontinuing Obinutuzumab and administering IVIg.31 Generally, females tend to have stronger immune responses than males, especially in viral infections. Estrogen is believed to promote B-cell activation and antibody production,33 which helps combat viruses and other pathogens.34^,^35 This suggests that the gender differences in the occurrence of enteroviral meningitis may be related to differences in immune responses, hormone levels, and reactions to immunosuppression between females and males. It indicates the potential existence of a gender-specific immune response mechanism, which warrants further investigation. Further research into this phenomenon may help clarify the mechanism behind Obinutuzumab-induced enteroviral infections and provide insights for personalized treatment and immune monitoring. Considering gender differences, developing gender-specific monitoring protocols will help improve treatment efficacy and the precision of personalized management.
It is important to emphasize that the above discussion regarding the adverse reactions of Obinutuzumab and their potential mechanisms remains speculative. The specific causal relationships need to be further verified through research. The occurrence of adverse reactions is influenced by various factors, including drug characteristics, individual differences, and underlying conditions. Therefore, more in-depth experimental and clinical studies are required to better understand the mechanisms behind these reactions. In addition, adverse events such as pure red cell aplasia and enteroviral meningitis, as identified in the study, are relatively rare. Given the rarity of these events, the authors recommend that these signals be further validated in independent cohorts or confirmed through targeted studies. This validation is crucial for determining the causal relationship between these adverse reactions and Obinutuzumab. Meanwhile, clinicians should continue to closely monitor adverse reactions during Obinutuzumab treatment and implement timely intervention measures.
Although this study provides scientific evidence for the safety assessment of Obinutuzumab, there are still some limitations. As the FAERS database is a spontaneous reporting system, its inherent characteristics, such as underreporting and incomplete case information, may affect the results, particularly regarding gender differences. Despite these limitations, the identification and detection of adverse reaction signals for Obinutuzumab in the FAERS database still provide valuable insights for further research and clinical treatment plans. Additionally, the efficacy and safety of Obinutuzumab for different diseases still require ongoing monitoring.
Conclusion
Obinutuzumab is associated with significant adverse event risks, notably higher in females, highlighting the need for enhanced safety monitoring and further exploration of gender-specific mechanisms in adverse event development.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Not applicable.
Authors’ contributions
Conceptualization, J.C., Y.L., and Z.B.; methodology, J.C., Z.B., H.L., and R.Z.; validation, J.C., Y.L., and H.L.; writing-original draft preparation, J.C.; data curation, Y.L., H.L., R.Z., M.D., and W.P. All the authors have read and agreed with the published version of the manuscript.
Funding
This research was funded by the 10.13039/501100001809National Natural Science Foundation of China (grant n° 82260106), the College Students’ Innovation Training Program under project numbers 2024106610965. Qianxinan Prefecture Science and Technology Project (ZHOU KE HE YI XUE 2025-1).
Data availability statement
The dataset generated and analyzed during and during the current study is available from the corresponding author on reasonable request.
Declaration of competing interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amudala N.A.Boukhlal S.Sheridan B.Langford C.A.Geara A.Merkel P.A.Obinutuzumab as treatment for ANCA-associated vasculitis Rheumatology (Oxford)6192022381438173495834310.1093/rheumatology/keab 916 · doi ↗ · pubmed ↗
- 2Al-Sawaf O.Robrecht S.Zhang C.Olivieri S.Chang Y.M.Fink A.M.Venetoclax-Obinutuzumab for previously untreated chronic lymphocytic leukemia: 6-year results of the randomized phase 3 CLL 14 study Blood 144182024192419353908266810.1182/blood.2024024631 PMC 11551846 · doi ↗ · pubmed ↗
- 3Gurumurthi A.Chin C.K.Feng L.Fowler N.H.Strati P.Hagemeister F.B.Safety and activity of lenalidomide in combination with obinutuzumab in patients with relapsed indolent non-Hodgkin lymphoma: a single group, open-label, phase 1/2 trial E Clinical Medicine 74202410274710.1016/j.eclinm.2024.102747 PMC 1133279539161543 · doi ↗ · pubmed ↗
- 4Al-Sawaf O.Zhang C.Tandon M.Sinha A.Fink A.M.Robrecht S.Venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab for previously untreated chronic lymphocytic leukaemia (CLL 14): follow-up results from a multicentre, open-label, randomised, phase 3 trial Lancet Oncol 2192020118812003288845210.1016/S 1470-2045(20)30443-5 · doi ↗ · pubmed ↗
- 5Sharman J.P.Egyed M.Jurczak W.Skarbnik A.Pagel J.M.Flinn I.W.Efficacy and safety in a 4-year follow-up of the ELEVATE-TN study comparing acalabrutinib with or without obinutuzumab versus obinutuzumab plus chlorambucil in treatment-naïve chronic lymphocytic leukemia Leukemia 3642022117111753497452610.1038/s 41375-021-01485-x PMC 8979808 · doi ↗ · pubmed ↗
- 6Le Gouill S.Morschhauser F.Chiron D.Bouabdallah K.Cartron G.Casasnovas O.Ibrutinib, obinutuzumab, and venetoclax in relapsed and untreated patients with mantle cell lymphoma: a phase 1/2 trial Blood 137720218778873318183210.1182/blood.2020008727 · doi ↗ · pubmed ↗
- 7Flowers C.R.Matasar M.J.Herrera A.F.Hertzberg M.Assouline S.Demeter J.Polatuzumab vedotin plus bendamustine and rituximab or obinutuzumab in relapsed/refractory follicular lymphoma: a phase Ib/II study Haematologica 10942024119412053776755010.3324/haematol.2023.283557 PMC 10985435 · doi ↗ · pubmed ↗
- 8Sharman J.P.Egyed M.Jurczak W.Skarbnik A.Pagel J.M.Flinn I.W.Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzmab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial Lancet 395102322020127812913230509310.1016/S 0140-6736(20)30262-2PMC 8151619 · doi ↗ · pubmed ↗