Inter-eye Asymmetry in Refractive and Corneal Responses to Orthokeratology for Myopia Control in Rural Adolescents: A Paired-Eye Analysis
Bradley A Nordin

TL;DR
This study finds that orthokeratology leads to similar eye treatment outcomes in both eyes of adolescents, making it a reliable method for controlling myopia.
Contribution
The study provides new evidence on the consistency of orthokeratology effects in both eyes, particularly in rural adolescent populations.
Findings
Orthokeratology results in minimal inter-eye asymmetry in refractive and corneal changes.
Older age and longer treatment duration are linked to slower myopia progression.
Baseline asymmetry and sex do not predict post-treatment asymmetry.
Abstract
Purpose The purpose of this study is to evaluate inter-eye asymmetry in refractive error (spherical equivalent, SE) and corneal curvature (mean keratometry, Km) following orthokeratology (ortho-k) in adolescents, and to identify clinical predictors of asymmetric treatment response using a paired-eye design. Methods A retrospective analysis was conducted in 53 adolescents (106 eyes; ages 8-16 years) treated with orthokeratology for at least 6 months. Absolute inter-eye differences (oculus dexter - oculus sinister (|OD−OS|)) in SE and Km were calculated at baseline and post-treatment. Paired-samples t-tests assessed inter-eye differences, Pearson correlations evaluated bilateral symmetry, and linear regression models examined predictors of post-treatment asymmetry, including baseline asymmetry, age, sex, treatment duration, and interaction terms. Generalized estimating equations were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
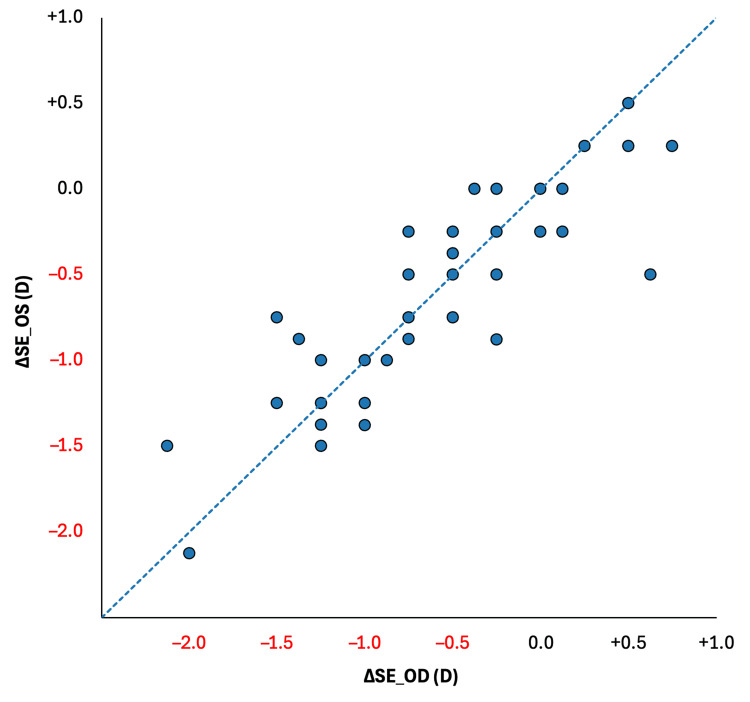 Figure 1
Figure 1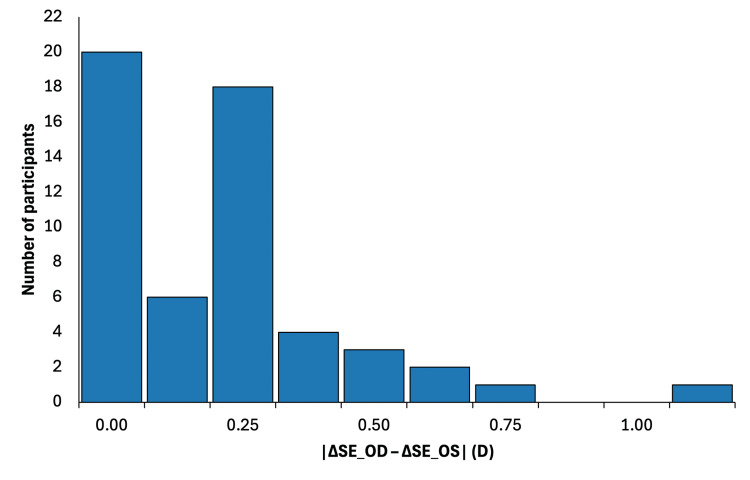 Figure 2
Figure 2| Participants | Number (n=53) | % |
| Male | 27 | 51% |
| Female | 26 | 49% |
| Eyes | 106 | |
| OD | 53 | 50% |
| OS | 53 | 50% |
| Ethnicity | ||
| White, Caucasian | 53 | 100% |
| Clinical parameter | Mean ± SD | Minimum | Maximum |
| Age at baseline, years | 11.2 ± 2.3 | 8 | 16 |
| Treatment duration, months | 56 ± 31 | 6 | 147 |
| Baseline spherical equivalent (SEi)a, D | −2.10 ± 1.12 | –7.5 | –0.75 |
| Baseline mean keratometry (Kmi), D | 43.21 ± 1.34 | 40.72 | 47.36 |
| Baseline inter-eye SE asymmetryb, D | 0.28 ± 0.34 | 0 | 1.88 |
| Baseline inter-eye Km asymmetryc, D | 0.37 ± 0.29 | 0.05 | 1.34 |
| Parameter | Baseline Asymmetry (|OD−OS|) | Post-Treatment Asymmetry (|OD−OS|) | t value | p-value |
| Spherical equivalent, SE (D) | 0.28 ± 0.34 | 0.22 ± 0.23 | 0.88 | 0.38 |
| Mean keratometry, Km (D) | 0.37 ± 0.29 | 0.15 ± 0.32 | 1.06 | 0.29 |
| Outcome Variable | Pearson r (OD vs OS) | p-value |
| Baseline refractive error (SEi) | 0.91 | < 0.001 |
| Post-treatment refractive error (SEf) | 0.96 | < 0.001 |
| Baseline mean keratometry (Kmi) | 0.87 | < 0.001 |
| Post-treatment mean keratometry (Kmf) | 0.93 | < 0.001 |
| Predictor | β Coefficient | t value | p-value |
| Baseline SE asymmetry | 0.144 | 1.45 | 0.153 |
| Age at initiation | 0.009 | 0.71 | 0.484 |
| Sex | −0.034 | −0.50 | 0.617 |
| Treatment duration | −0.001 | −1.06 | 0.294 |
| Sex × asymmetry interaction | 0.021 | 0.34 | 0.737 |
| Predictor | B (SE) | Wald χ² | 95% CI | p-value |
| Age | −0.037 | 5.33 | −0.068 to −0.006 | 0.021 |
| Treatment duration | −0.005 | 10.78 | −0.008 to −0.002 | 0.001 |
| Baseline SE asymmetry | 0.004 | 0.08 | −0.028 to 0.036 | 0.783 |
| Sex | 0.011 | 0.22 | −0.036 to 0.058 | 0.636 |
| Sex × asymmetry | −0.006 | 0.11 | −0.041 to 0.029 | 0.737 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Impairment Studies · Corneal surgery and disorders · Glaucoma and retinal disorders
Introduction
Myopia is an increasingly prevalent global public health concern, with projections estimating that nearly half of the world’s population will be myopic by 2050 and up to one billion individuals will be at risk for high myopia and its associated sight-threatening complications [1,2]. High myopia is strongly associated with retinal detachment, myopic maculopathy, and glaucoma, underscoring the importance of early intervention during childhood and adolescence [3,4]. Untreated myopia progression during these developmental years commonly averages approximately −0.50 diopters per year (D/y), with faster rates reported in younger children and certain demographic groups [5-7].
Orthokeratology (ortho-k) has emerged as an effective non-surgical intervention for myopia control, with multiple randomized controlled trials and meta-analyses demonstrating reductions in myopia progression and axial elongation of approximately 30-50% compared with single-vision spectacle correction [8-11]. The primary mechanism of ortho-k is believed to involve overnight corneal reshaping that induces relative peripheral myopic defocus, thereby altering retinal growth signaling and slowing axial elongation [12-14]. Long-term studies have demonstrated sustained efficacy with continued lens wear and an acceptable safety profile when appropriate hygiene and clinical follow-up are maintained [11,15,16].
Despite extensive evidence supporting the efficacy of ortho-k, the symmetry of treatment response between eyes has received comparatively little attention. Inter-eye refractive asymmetry is common in pediatric populations and has been associated with differential progression rates in untreated cohorts [6,17]. Most ortho-k studies analyze eyes independently or report group-level averages, which may obscure clinically relevant inter-eye differences in refractive or corneal response. Understanding whether ortho-k induces asymmetric treatment effects is therefore important for binocular visual development, lens fitting strategies, and long-term clinical management, particularly in children with baseline anisometropia.
This question is especially relevant in rural and underserved populations, where access to subspecialty eye care and frequent follow-up may be limited [18,19]. Appalachian communities, in particular, face persistent barriers related to geographic isolation, socioeconomic disadvantage, and reduced access to pediatric eye care services [20]. In a prior retrospective study, our group demonstrated that ortho-k significantly reduced myopia progression rates in adolescents from a rural Appalachian population compared with published untreated norms [21]. However, that analysis did not evaluate inter-eye asymmetry in refractive or corneal outcomes.
Accordingly, the purpose of the present study was to evaluate inter-eye asymmetry in refractive and corneal curvature responses following orthokeratology treatment in adolescents using a paired-eye design. The study aimed to quantify baseline and post-treatment asymmetry in spherical equivalent and mean keratometry, assess the magnitude and distribution of asymmetry, and identify clinical predictors of asymmetric response. It was hypothesized that orthokeratology would produce largely symmetric bilateral effects, even in the presence of baseline inter-eye differences.
Materials and methods
Study design and population
This retrospective paired-eye study included adolescents treated with orthokeratology at a single rural clinical practice serving Appalachian communities [22,23]. Eligible participants were required to meet the following inclusion criteria: (1) age 8-16 years at the time of orthokeratology initiation; (2) bilateral orthokeratology lens wear; (3) a minimum treatment duration of six months; and (4) availability of complete refractive (spherical equivalent) and corneal topography (mean keratometry) data for both eyes at baseline and follow-up.
Exclusion criteria included the presence of ocular pathology other than refractive error (e.g., keratoconus, corneal dystrophy, active ocular surface disease), prior ocular surgery, history of amblyopia or strabismus requiring treatment, incomplete bilateral clinical data, or inconsistent orthokeratology lens wear that precluded reliable assessment of treatment response.
Fifty-three adolescents (106 eyes) met all inclusion criteria and were included in the final analysis. All participants were of White/Caucasian descent and resided in rural Appalachian communities. Demographic characteristics are summarized in Table 1.
Orthokeratology Treatment
All patients were fitted with Boston XO reverse-geometry rigid gas-permeable ortho-k lenses (Bausch + Lomb, Quebec, Canada) according to standard clinical protocols [9-11,15]. Lenses were worn overnight and removed upon waking. Follow-up visits included refraction and corneal topography assessments.
Outcome Measures
Primary outcomes included spherical equivalent refraction (SE), defined as the sphere power plus one-half of the cylindrical correction, consistent with standard refractive reporting [24], and mean keratometry (Km), defined as the average of the principal corneal curvature values (K1 and K2) representing overall central corneal curvature. Absolute inter-eye asymmetry was calculated as the absolute difference between the right (OD) and left (OS) eyes (|OD−OS|) for each variable at baseline and post-treatment. Annualized refractive progression rates were calculated when longitudinal data were available. For subject-level analyses, bilateral measurements were averaged within individuals to avoid pseudo-replication, consistent with best practices for paired-eye ophthalmic studies [25,26].
Statistical Analysis
Paired t-tests were used to compare OD and OS measurements at baseline and follow-up. Pearson correlation coefficients were used to assess bilateral symmetry. Linear regression models were used to evaluate predictors of post-treatment asymmetry, including baseline asymmetry, age, sex, treatment duration, and sex × asymmetry interaction. Generalized estimating equations (GEE) with an exchangeable correlation structure were used to model predictors of annualized refractive progression while accounting for inter-eye correlation [27].
Statistical analyses were performed using IBM SPSS Statistics (version 30.0; IBM Corp, Armonk, NY, US). A p-value < 0.05 was considered statistically significant.
Results
Baseline characteristics
The mean age at treatment initiation was 11.2 ± 2.3 years (range: 8-16 years), with a mean orthokeratology treatment duration of 56 ± 31 months (range: 6-147 months). At baseline, the mean absolute inter-eye asymmetry was 0.28 ± 0.34 D for spherical equivalent and 0.37 ± 0.29 D for mean keratometry, consistent with previously reported ranges of inter-eye refractive variability in pediatric cohorts [6,17]. Baseline clinical parameters for study participants are summarized in Table 2.
Inter-eye symmetry of refractive and corneal outcomes
No statistically significant differences were observed between right (OD) and left (OS) eyes for spherical equivalent or mean keratometry at baseline or following orthokeratology treatment (paired t-tests, all p > 0.05; Table 3). Bilateral correlations between eyes were strong for all refractive and corneal measures at both time points (Pearson ρ = 0.87-0.96, all p < 0.001; Table 4), consistent with prior reports of symmetric response to orthokeratology [14,28], and indicating a high degree of bilateral concordance in treatment response.
A scatter plot comparing right-eye and left-eye changes in spherical equivalent (ΔSE) visually reinforces this bilateral concordance (Figure 1). Individual data points clustered closely along the line of identity, demonstrating that refractive changes induced by orthokeratology were highly symmetric between eyes across participants.
Comparing changes in spherical equivalent refraction (ΔSE) between right (OD) and left (OS) eyes following orthokeratologyEach point represents one participant (n = 53). The diagonal line represents the line of identity (y = x), indicating equal refractive change between eyes. The close clustering of points along the identity line demonstrates strong bilateral symmetry in refractive response to treatment.D: diopters
Inter-eye asymmetry magnitude and distribution
Post-treatment asymmetry in refractive and corneal outcomes was minimal. The mean absolute asymmetry in refractive change (|(ΔSE_OD − ΔSE_OS)|) was 0.22 ± 0.23 D, while the mean absolute asymmetry in corneal curvature change was 0.15 ± 0.32 D (Table 3).
Although most participants demonstrated low inter-eye asymmetry, a subset exhibited higher asymmetry exceeding commonly used clinical thresholds for refractive asymmetry. Depending on the threshold applied (0.5-0.8 D), 11-23% of participants met criteria for higher asymmetry, thresholds commonly cited in anisometropia and refractive literature [6,29]. The distribution of absolute inter-eye asymmetry in refractive change is shown in Figure 2, which demonstrates that the majority of participants clustered at low asymmetry values, with relatively few outliers.
Distribution of absolute inter-eye asymmetry in refractive change following orthokeratology.Histogram showing the absolute difference between right-eye and left-eye changes in spherical equivalent (|ΔSE_OD − ΔSE_OS|). Most participants demonstrated minimal asymmetry, with relatively few exceeding commonly used clinical thresholds.D: diopters
Predictors of post-treatment asymmetry
Linear regression analyses revealed no significant predictors of post-treatment inter-eye asymmetry in refractive outcomes. Baseline SE asymmetry, age at treatment initiation, sex, treatment duration, and the sex × asymmetry interaction term were all non-significant predictors (all p > 0.15), with low explanatory power across models (R² < 0.07; Table 5). The absence of identifiable predictors of post-treatment asymmetry is consistent with prior work suggesting limited predictability of inter-eye refractive divergence over time [17].
Myopia progression
Generalized estimating equation (GEE) analysis of annualized refractive progression demonstrated that increasing age at treatment initiation (B = −0.037, p = 0.021) and longer orthokeratology treatment duration (B = −0.005, p = 0.001) were significantly associated with slower myopia progression (Table 6). In contrast, baseline inter-eye asymmetry, sex, and interaction terms were not associated with progression rate (all p > 0.6).
Discussion
The present paired-eye analysis demonstrates that orthokeratology produces highly symmetric bilateral refractive and corneal responses in adolescents, even in the presence of baseline inter-eye differences. Strong correlations between the right and left eyes and minimal absolute asymmetry following treatment suggest that ortho-k induces consistent optical and biomechanical effects within individuals. These findings extend prior evidence supporting ortho-k efficacy by showing that its myopia control benefits are not only effective but also predictably bilateral.
Previous studies have established the effectiveness of ortho-k in slowing myopia progression and axial elongation in children and adolescents [8-11,15,16]. However, most investigations have analyzed eyes independently or focused on population-level averages, which may obscure clinically meaningful inter-eye differences. By employing a paired-eye design, the present study directly addresses this gap and provides visual confirmation of bilateral concordance through scatter analysis of refractive change (Figure 1). The close clustering of points along the line of identity reinforces the statistical findings and supports the conclusion that treatment responses between eyes are closely matched.
Inter-eye asymmetry in refractive error is relatively common in pediatric populations and has been associated with differential progression rates in untreated cohorts [6,17]. Such asymmetry can raise clinical concerns regarding binocular vision development, lens-fitting strategies, and long-term refractive balance. In the current study, although a subset of participants exhibited asymmetry exceeding commonly cited clinical thresholds, the overall distribution of asymmetry was skewed toward low values (Figure 2), and higher asymmetry was not associated with poorer outcomes or accelerated progression. This pattern suggests that observed variability likely reflects normal biological heterogeneity rather than inconsistent treatment effects.
The absence of identifiable predictors of post-treatment asymmetry further supports the robustness of ortho-k treatment. Neither baseline refractive imbalance, age, sex, nor treatment duration significantly predicted asymmetric response. These findings are consistent with emerging biomechanical evidence indicating that ortho-k induces relatively uniform corneal epithelial redistribution and curvature changes across eyes, even when baseline corneal geometry differs modestly [14,22,23]. This uniformity likely reflects the dominant role of peripheral retinal defocus in modulating ocular growth rather than localized baseline refractive differences [12,13].
Importantly, generalized estimating equation analysis demonstrated that older age at treatment initiation and longer treatment duration were associated with slower myopia progression, while baseline inter-eye asymmetry was not. These results align with prior longitudinal studies showing that younger age is a key risk factor for faster progression and that sustained ortho-k wear is necessary to maintain treatment efficacy [15,16,24]. The lack of association between asymmetry and progression further suggests that clinicians need not alter treatment strategies solely based on baseline inter-eye differences.
From a clinical perspective, the demonstrated bilateral consistency of ortho-k is particularly relevant for rural and underserved populations. In settings where access to subspecialty care and advanced imaging may be limited, treatment modalities that offer predictable and symmetric outcomes can simplify clinical management and patient counseling [18-20]. This is especially important in pediatric patients, for whom long-term adherence and continuity of care are critical. Our findings build upon prior work showing effective myopia control in rural Appalachian adolescents treated with ortho-k and further support its use as a reliable strategy in such populations [21].
Limitations
Several limitations of this study should be acknowledged. First, the retrospective design introduces inherent constraints, including potential selection bias and reliance on the completeness and accuracy of existing clinical records. Although all eligible patients meeting predefined inclusion criteria were included, data availability limited analyses to refractive and keratometric outcomes routinely collected in clinical practice. Axial length measurements and detailed corneal biomechanical parameters were not consistently available and therefore could not be evaluated.
Second, data extraction was restricted to visits with complete bilateral measurements for both spherical equivalent and mean keratometry; records lacking paired-eye data, incomplete follow-up, or inconsistent orthokeratology lens wear were excluded to ensure analytic validity. While this approach strengthens internal consistency, it may limit generalizability to broader clinical populations. Finally, the study cohort was demographically homogeneous and derived from a single rural clinical practice, which may further limit external applicability. Despite these limitations, the paired-eye design, extended treatment duration, and use of statistical methods accounting for inter-eye correlation support the robustness of the findings.
Conclusions
In conclusion, this paired-eye analysis demonstrates that orthokeratology produces highly consistent and symmetric bilateral refractive and corneal curvature responses in adolescents, even in the presence of baseline inter-eye differences. Absolute inter-eye asymmetry in spherical equivalent and mean keratometry remained low following treatment, and no clinically meaningful differences were observed between right and left eyes. Importantly, commonly considered patient and treatment factors, including age at initiation, sex, treatment duration, and baseline asymmetry, did not predict asymmetric outcomes, indicating that treatment effects were robust and uniform across individuals. These findings suggest that orthokeratology exerts predictable bilateral effects on both refractive error and corneal shape, supporting its reliability as a myopia-control strategy in pediatric populations. From a clinical perspective, the demonstrated symmetry of treatment response may simplify lens fitting, monitoring, and patient counseling, particularly in rural or underserved settings where access to frequent subspecialty follow-up may be limited. Overall, the results reinforce orthokeratology as a dependable and consistent intervention for myopia management in adolescents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050 Ophthalmology Holden BA Fricke TR Wilson DA 1036104212320162687500710.1016/j.ophtha.2016.01.006 · doi ↗ · pubmed ↗
- 2Nearly 1 billion myopes at risk of myopia-related sight-threatening conditions by 2050 - time to act now Clin Exp Optom Holden BA Jong M Davis S Wilson D Fricke T Resnikoff S 4914939820152676917510.1111/cxo.12339 · doi ↗ · pubmed ↗
- 3Myopia Lancet Morgan IG Ohno-Matsui K Saw SM 1739174837920122255990010.1016/S 0140-6736(12)60272-4 · doi ↗ · pubmed ↗
- 4Myopia control: why each diopter matters Optom Vis Sci Bullimore MA Brennan NA 4634659620193111616510.1097/OPX.0000000000001367 · doi ↗ · pubmed ↗
- 5Myopia progression rates in urban children wearing single-vision spectacles Optom Vis Sci Donovan L Sankaridurg P Ho A Naduvilath T Smith EL 3rd Holden BA 27328920122198312010.1097/OPX.0b 013e 3182357 f 79PMC 3249020 · doi ↗ · pubmed ↗
- 6Myopia progression as a function of sex, age, and ethnicity Invest Ophthalmol Vis Sci Jones-Jordan LA Sinnott LT Chu RH 3662202110.1167/iovs.62.10.36PMC 841186634463720 · doi ↗ · pubmed ↗
- 7Progression of myopia in school-aged children after COVID-19 home confinement JAMA Ophthalmol Wang J Li Y Musch DC 29330013920213344354210.1001/jamaophthalmol.2020.6239 PMC 7809617 · doi ↗ · pubmed ↗
- 8Orthokeratology for myopia control: a meta-analysis Optom Vis Sci Si JK Tang K Bi HS Guo DD Guo JG Wang XR 2522579220152559933810.1097/OPX.0000000000000505 · doi ↗ · pubmed ↗