Prediction of Functional Outcomes at Discharge Using Plasma Concentration of von Willebrand Factor Antigen at Admission in Hospitalized Patients with COVID-19
Masayuki Oki, Daisuke Yamasawa, Shinichi Goto, Hidetaka Yanagi, Saki Manabe, Takako Kobayashi, Ayumi Tsuda, Shota Sato, Seiji Morita, Yoshihide Nakagawa, Tsuyoshi Oguma, Koichiro Asano, Norio Yamamoto, Hideki Ozawa, Shinya Goto

TL;DR
High levels of von Willebrand factor at hospital admission predict poor recovery in hospitalized COVID-19 patients.
Contribution
Shows that von Willebrand factor antigen levels at admission are independently linked to functional outcomes at discharge in COVID-19 patients.
Findings
Elevated VWF:Ag levels at admission are associated with a Clinical Frailty Scale score ≥4 at discharge.
The association remains significant after adjusting for age and sex.
Abstract
Coronavirus disease 2019 (COVID-19) causes endothelial injury through inflammatory and hypoxic stress, leading to vascular dysfunction and immunothrombosis. The plasma level of von Willebrand factor (VWF) could serve as a biomarker of vascular injury. While elevated VWF predicts mortality in severe COVID-19, its relationship with post-discharge functional outcomes remains unclear. This study aimed to determine whether plasma VWF antigen (VWF:Ag) levels at admission predict functional status at discharge in patients hospitalized for COVID-19. This was a single-center prospective cohort study conducted at Tokai University Hospital from July to September 2021. We evaluated the relationship between plasma VWF:Ag levels at admission and a Clinical Frailty Scale (CFS) score ≥4 at discharge using univariable and multivariable logistic regression analyses. A total of 97 patients were enrolled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
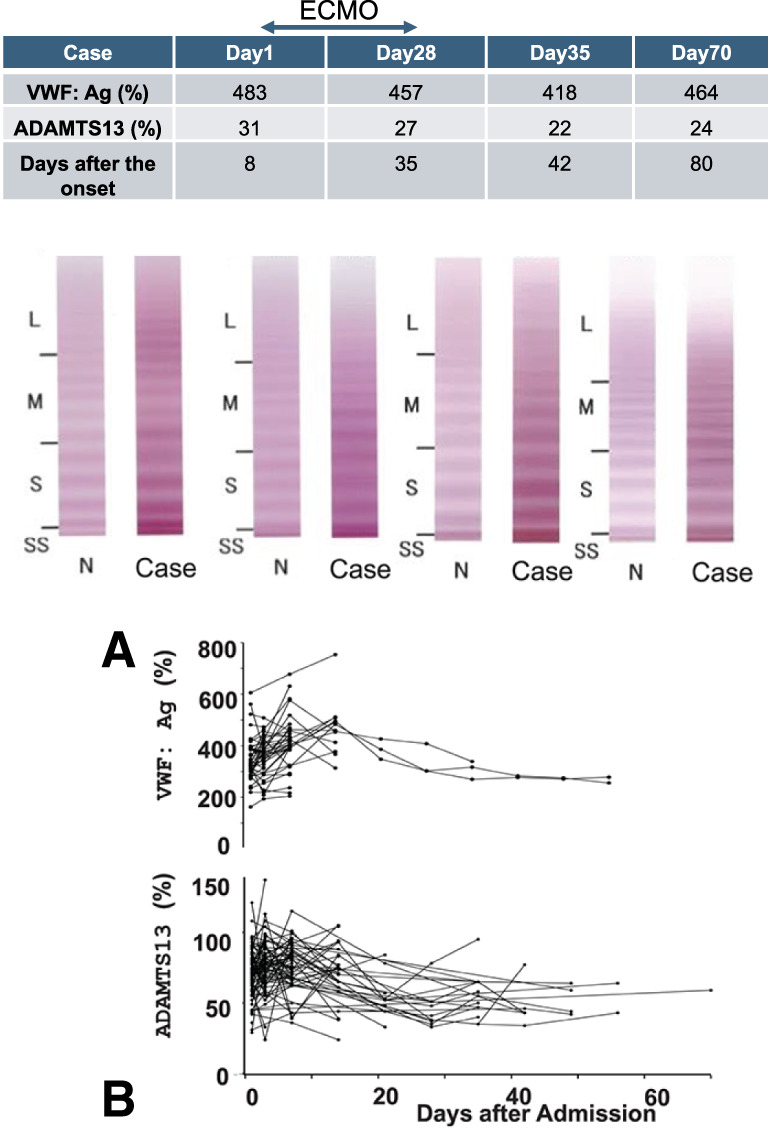 Fig. 1
Fig. 1| Factor | Group | N (%) or median [IQR] |
|---|---|---|
| n | 97 | |
| Age | 56.00 [49.00, 62.00] | |
| Gender | Male | 71 (73.2) |
| Female | 26 (26.8) | |
| Smoking history | Current | 15 (16.1) |
| Former | 21 (22.6) | |
| No | 57 (61.3) | |
| Drinking history | Yes | 34 (37.4) |
| No | 57 (62.6) | |
| Obesity (BMI >30) | Yes | 28 (28.9) |
| No | 69 (71.1) | |
| Hypertension | Yes | 34 (35.4) |
| No | 62 (64.6) | |
| Cardiovascular disease | Yes | 5 (5.2) |
| No | 92 (94.8) | |
| Diabetes mellitus | Yes | 30 (30.9) |
| No | 67 (69.1) | |
| Active cancer | Yes | 3 (3.1) |
| No | 94 (96.9) | |
| Chronic lung disease | Yes | 10 (10.3) |
| No | 87 (89.7) | |
| CKD | Yes | 7 (7.2) |
| No | 90 (92.8) | |
| Immunocompromised hosts | Yes | 4 (4.1) |
| No | 93 (95.9) | |
| Liver cirrhosis | Yes | 1 (1.0) |
| No | 96 (99.0) | |
| VWF-related | ||
| VWF:Ag (%) | 330.0 [273.0, 391.8] | |
| ADAMTS13 activity (%) | 74.0 [64.0, 80.0] | |
| VWF/ADAMTS13 ratio | 4.3 [3.6, 5.8] | |
| Inflamation-related | ||
| CRP (mg/dL) | 8.5 [2.7, 13.5] | |
| WBC (/μL) | 7900.0 [5400.0, 11100.0] | |
| Absolute lymphocyte counts (/μL) | 623.4 [403.5, 844.5] | |
| Thrombosis-related | ||
| D-dimer (μg/mL) | 1.0 [0.6, 1.8] | |
| PAI-1 (ng/mL) | 56.0 [44.8, 76.5] | |
| TM (U/mL) | 22.8 [15.7, 26.3] | |
| Others | ||
| Albumin (g/dL) | 2.9 [2.8, 3.1] | |
| CPK (U/L) | 130.5 [54.0, 228.5] | |
| LD (U/L) | 526.0 [415.0, 654.0] | |
| Creatinine (mg/dL) | 0.8 [0.7, 1.1] | |
| Troponin T (ng/mL) | 6.0 [4.0, 22.0] | |
| Ferritin (ng/mL) | 1251 [604, 2098] |
| Prone position | |
| Yes | 69 (74.2) |
| No | 24 (25.8) |
| High-flow oxygen therapy | |
| Yes | 58 (59.8) |
| No | 39 (40.2) |
| Ventilator | |
| Yes | 24 (24.7) |
| No | 73 (75.3) |
| Vasopressors | |
| Yes | 19 (19.6) |
| No | 78 (80.4) |
| Hemodialysis | |
| Yes | 6 (6.2) |
| No | 91 (93.8) |
| ECMO | |
| Yes | 6 (6.2) |
| No | 91 (93.8) |
| CFS score at discharge | |
| 1 | 2 (2.1) |
| 2 | 24 (24.7) |
| 3 | 34 (35.1) |
| 4 | 6 (6.2) |
| 5 | 7 (7.2) |
| 6 | 10 (10.3) |
| 7 | 14 (14.4) |
| Death during hospitalization | |
| Yes | 8 (8.2) |
| No | 89 (91.8) |
| Discharge destination | |
| Home | 33 (37.1) |
| (If alive at discharge) | |
| Transfer | 56 (62.9) |
| Factor | Group | CFS <4 | CFS ≥4 | p-Value |
|---|---|---|---|---|
| N (%) or median [IQR] | N (%) or median [IQR] | |||
| N = 89 | 60 | 29 | ||
| Age | 56.0 [49.0, 62.3] | 52.0 [49.0, 62.0] | 0.927 | |
| Gender | Female | 11 (18.3) | 12 (41.4) | 0.037 |
| Male | 49 (81.7) | 17 (58.6) | ||
| Smoking history | Current | 11 (18.6) | 4 (15.4) | 0.760 |
| Former | 15 (25.4) | 5 (19.2) | ||
| No | 33 (55.9) | 17 (65.4) | ||
| Drinking history | Yes | 27 (45.8) | 6 (25.0) | 0.090 |
| No | 32 (54.2) | 18 (75.0) | ||
| Obesity (BMI >30) | Yes | 15 (25.0) | 11 (37.9) | 0.224 |
| No | 45 (75.0) | 18 (62.1) | ||
| Hypertension | Yes | 19 (32.2) | 12 (41.4) | 0.478 |
| No | 40 (67.8) | 17 (58.6) | ||
| Cardiovascular disease | Yes | 2 (3.3) | 0 (0.0) | 1 |
| No | 58 (96.7) | 16 (100.0) | ||
| Active cancer | Yes | 3 (5.0) | 0 (0.0) | 0.548 |
| No | 57 (95.0) | 16 (100.0) | ||
| Chronic lung disease | Yes | 7 (11.7) | 3 (10.3) | 1 |
| No | 53 (88.3) | 26 (89.7) | ||
| CKD | Yes | 3 (5.0) | 1 (3.4) | 1 |
| No | 57 (95.0) | 28 (96.6) | ||
| Diabetes mellitus | Yes | 16 (26.7) | 9 (31.0) | 0.802 |
| No | 44 (73.3) | 20 (69.0) | ||
| Immunocompromised hosts | Yes | 3 (5.0) | 1 (3.4) | 1 |
| No | 57 (95.0) | 28 (96.6) | ||
| Liver cirrhosis | Yes | 13 (22.4) | 0 (0.0) | 0.326 |
| No | 45 (77.6) | 16 (100.0) | ||
| Prone position | Yes | 53 (74.6) | 17 (65.4) | 0.760 |
| No | 18 (25.4) | 9 (34.6) | ||
| WBC (/μL) | 7550.00 [4725.00, 9725.00] | 7900.00 [5600.00, 12300.00] | 0.261 | |
| Albumin (g/dL) | 3.00 [2.85, 3.30] | 2.90 [2.70, 3.10] | 0.02 | |
| Creatinine (mg/dL) | 0.79 [0.66, 0.95] | 0.84 [0.68, 1.20] | 0.338 | |
| CRP (mg/dL) | 7.34 [2.77, 15.04] | 4.33 [1.95,12.61] | 0.549 | |
| D-dimer (μg/mL) | 0.70 [0.50,1.10] | 1.50 [0.90, 2.70] | <0.001 | |
| Ferritin (ng/mL) | 3.00 [1.00, 6.00] | 2.00 [2.00, 4.00] | 0.873 | |
| IL-6 (pg/mL) | 23.40 [7.83, 54.85] | 66.75 [34.77, 229.25] | 0.006 | |
| LD (U/L) | 473.00 [359.25, 583.50] | 567.00 [485.00, 777.00] | 0.005 | |
| Procalcitonin (ng/mL) | 0.12 [0.06, 0.24] | 0.22 [0.08, 0.45] | 0.12 | |
| VWF:Ag (%) | 301.00 [244.00, 362.00] | 391.00 [326.00, 412.00] | <0.001 | |
| ADAMTS13 activity (%) | 73.50 [66.75, 80.00] | 71.00 [62.00, 81.00] | 0.566 | |
| VWF/ADAMTS13 | 4.10 [3.21, 4.98] | 5.08 [4.32, 6.59] | 0.001 | |
| PAI-1 (ng/mL) | 53.00 [43.50, 68.25] | 61.00 [46.25, 103.50] | 0.07 | |
| TM (U/mL) | 18.15 [14.80, 24.35] | 20.90 [17.50, 27.10] | 0.078 |
| Variable | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| VWF:Ag (%) | 1.010 | 1.000–1.010 | 0.005 |
| ADAMTS13 (%) | 0.989 | 0.963–1.020 | 0.435 |
| VWF/ADAMTS13 ratio | 1.360 | 1.070–1.730 | 0.013 |
| TM (U/mL) | 1.030 | 0.990–1.070 | 0.142 |
- —Ministry of Education, Culture, Sports, Science and Technology
- —Agency for Cultural Affairs, Government of Japan
- —Cross-ministerial Strategic Innovation Promotion Program
- —Integrated Health Care System
- —Fukuda Memorial Foundation
- —Japan Agency for Medical Research and Development
- —Nakatani Foundation for Advancement of Measuring Technologies in Biomedical Engineering
- —Suzuken Memorial Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Platelet Disorders and Treatments · Complement system in diseases
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus attacks both airway epithelial cells and vascular endothelial cells.^1–3)^ Damage to airway epithelial cells leads to severe lung injury,^4)^ while damage to vascular endothelial cells results in extensive vascular disorders.^4)^ The prognosis is affected by the severity of both types of injuries. Plasma biomarkers of endothelial injury can provide insights into the extent of vascular damage at the time of admission.^5,6)^
Von Willebrand factor (VWF) is primarily released from damaged vascular endothelial cells.^7)^ Plasma VWF serves as a biomarker of endothelial dysfunction in cardiovascular diseases.^8–10)^ In coronavirus disease 2019 (COVID-19), SARS-CoV-2 infects endothelial cells via the angiotensin-converting enzyme (ACE2) receptor,^4,11)^ triggering immunothrombosis—a key pathophysiologic mechanism.^12)^ While elevated plasma VWF antigen (VWF:Ag) levels predict in-hospital mortality in severe COVID-19,^13,14)^ their ability to predict functional recovery and discharge status remains unclear. Given that endothelial injury may influence the post-acute phase of functional capacity, we hypothesized that VWF:Ag levels at admission predict impaired functional status at discharge. This study aimed to investigate whether plasma VWF:Ag levels measured at hospital admission predict functional outcomes at discharge in hospitalized COVID-19 patients.
Materials and Methods
Study population
All consecutive patients admitted to Tokai University Hospital for SARS-CoV-2 infection between July and September 2021 were recruited for this study. The Institutional Review Board approved the study (21R058), and written informed consent was obtained from all participants.
Clinical outcome of interest
The primary outcome measured was impaired functional status at discharge, which was defined as a Clinical Frailty Scale (CFS) score of 4 or higher.^15,16)^ We used the 7-point CFS scale (scores 1–7).^17)^ In the original 7-point CFS, score 7 encompasses both “severely frail” patients and those who are “terminally ill” or approaching death.^15)^ For the purpose of this analysis, we focused exclusively on patients who were discharged alive, as the CFS is designed primarily to assess functional status. Therefore, the 8 patients who died during hospitalization were excluded from the primary analysis comparing CFS score ≥4 versus CFS score <4. The in-hospital mortality rate (8.2%) is reported separately as a clinical outcome.
Measured parameters
The following plasma parameters were measured at admission and serial intervals: VWF:Ag levels, VWF cleavage protease ADAMTS13 (a disintegrin and metalloproteinase with thrombospondin type 1 motifs member) levels, and other parameters, including blood cell counts, inflammation markers, and thrombosis markers.
Primary hypothesis and statistical analysis
We hypothesized that plasma VWF:Ag levels at admission could predict an individual’s functional status at discharge. To investigate the association between VWF:Ag levels at admission and a CFS score of 4 or higher at discharge, we used both univariable and multivariable logistic regression analyses, adjusting for age and sex. A 2-sided p-value of less than 0.05 was considered statistically significant. Patients who died during hospitalization (n = 8) were excluded from the logistic regression analysis, as the CFS scale is designed to assess functional status in living patients rather than mortality outcomes.
Results
Baseline characteristics
A total of 97 patients were recruited for the study. Eight patients (8.2%) died during hospitalization and were excluded from the primary analysis of functional outcomes at discharge. The remaining 89 patients who were discharged alive were included in the analysis comparing CFS scores <4 (n = 60) versus ≥4 (n = 29). Many of the patients were male, accounting for 73.2% of the cohort, and the median age was 56 years, with an interquartile range (IQR) of 49–62 years. The risk factor profile among the patients was generally low. A limited smoking history was noted, with 22.6% classified as former smokers and 16.1% as current smokers. The prevalence of obesity was low at 28.9%, along with a history of hypertension (35.4%), cardiovascular diseases (5.2%), diabetes mellitus (30.9%), active cancer (3.1%), and chronic lung diseases (10.3%) (Table 1).
Plasma markers at admission
Patients exhibited significant inflammation, as evidenced by an elevated C-reactive protein (CRP) level with a median of 8.5 mg/dL (95% confidence interval [CI]: 2.7–13.5). White blood cell (WBC) counts were nearly normal, averaging 7900/μL (95% CI: 5400–11100). Additionally, D-dimer levels were elevated at 1.0 μg/mL (95% CI: 0.6–1.8). The VWF:Ag level was notably high at 330.0% (95% CI: 273.0–391.8), while the ADAMTS13 level was lower, recorded at 74.0% (95% CI: 64.0–80.0) (Table 1).
Clinical course
High-flow oxygen therapy was utilized in 59.8% of cases, while 24.7% of patients required mechanical ventilation. Hemodialysis and extracorporeal membrane oxygenation (ECMO) were necessary for 6.2% of the patients each. During hospitalization, 8 patients (8.2%) passed away. Of those who were discharged, 37.1% returned home, while 62.9% were transferred to secondary hospitals or nursing homes (Table 2).
A representative Western blot analysis of VWF multimers indicates elevated levels of VWF:Ag. However, there are no significant differences in the distribution of multimers when compared to standard plasma (Fig. 1A). Furthermore, the changes in VWF:Ag and ADAMTS13 levels during the admission period reveal consistently low levels of ADAMTS13 alongside high levels of VWF:Ag (Fig. 1B).
(A) A representative Western blot analysis of VWF multimers. It indicates that VWF levels are elevated, yet there are no significant differences in the distribution of multimers when compared to standard plasma. (B) The changes in VWF and ADAMTS13 levels over the course of admission, showing consistently low levels of ADAMTS13 alongside high levels of VWF. VWF:Ag: von Willebrand factor:antigen; ECMO: extracorporeal membrane oxygenation; ADAMTS13: a disintegrin and metalloproteinase with thrombospondin type 1 motifs member
Functional status at discharge
Among the 89 patients who were discharged alive, 29 had a CFS score of 4 or higher. At baseline, no clinical characteristics were significantly associated with a CFS score of 4 or higher, except for gender (p = 0.037) (Table 3). Several plasma markers showed a correlation with a CFS of 4 or higher (Table 3): lower albumin levels (p = 0.02), higher D-dimer levels (p < 0.001), elevated interleukin-6 (IL-6) levels (p = 0.006), increased lactate dehydrogenase (LD) (p = 0.005), higher VWF:Ag levels (p = 0.001), and a higher VWF/ADAMTS13 ratio (p = 0.001).
Table 3: Baseline characteristics and laboratory parameters by discharge functional status (CFS <4 vs. CFS ≥4)
Prediction of functional outcome
The univariable analysis indicated that both VWF:Ag levels and the VWF/ADAMTS13 ratio were significantly associated with a CFS score of 4 or higher. This significance remained after adjusting for age and sex (Table 4). The adjusted odds ratio (OR) for VWF:Ag levels was 1.010 (95% CI: 1.000–1.010, p = 0.005), while the adjusted OR for the VWF/ADAMTS13 ratio was 1.360 (95% CI: 1.070–1.730, p = 0.013).
Discussion
Our single-center study confirmed that plasma levels of VWF:Ag were significantly elevated at admission, which predicted poor functional outcomes at discharge represented by CFS. This suggests that the extent of vascular damage has prognostic value. Larger VWF multimers are cleaved by ADAMTS13,^18)^ and decreased levels of ADAMTS13 at admission indicate its consumption during the cleavage of VWF from virus-stimulated endothelial cells.^19)^ The VWF/ADAMTS13 ratio, a marker of the balance between thrombosis and bleeding,^20)^ was elevated and predicted poor outcomes.
CFS is widely used to determine the need for admission to a decision unit or intensive care unit (ICU) globally.^17)^ National Institute for Health and Care Excellence guidelines for critical care also recommend the use of CFS for selecting patients suitable for ICU admission.^21)^ In Japan, CFS was used also for “download transfer” of recovered patients from high-intensity hospitals to the lower-grade ones. Thus, the CFS is one of the most widely used scales for evaluating the recovery status of patients admitted to high-intensity hospitals such as Tokai University Hospital. Obviously, the CFS scale is influenced largely by time course, especially in patients with infectious diseases, including COVID-19. However, during the COVID-19 pandemic, the Japanese government guided the prompt “download transfer” of severe COVID-19 patients from high-intensity hospitals to lower-intensity hospitals after recovery. Thus, it was practically difficult to measure CFS with a fixed period. Given the importance of time as an influencing factor for CFS, measuring CFS at discharge may pose a significant limitation. Moreover, the CFS is a rather general parameter that reflects the functional state of the target patients.^22)^ It reflects the severity of thrombosis or bleeding, as well as the simple damage caused by viral infection. Our study provides prognostic value for VWF:Ag level at admission. However, the causal link between increased VWF:Ag at admission and the poor CFS at discharge is still to be elucidated.
Regarding our choice of scale, we utilized the 7-point CFS (scores 1–7) rather than the 9-point version. When this study was planned in 2021, the 7-point scale was familiar to our team and was the standard tool in our institution. In the original 7-point scale, score 7 encompasses both severely frail patients and those approaching death, acknowledging that these states are often indistinguishable in acute illness.^15)^ During the download transfer process, we faced significant challenges differentiating between severe frailty and impending mortality in the long-term phase of COVID-19. Patients often exhibited profound functional impairment that made it impossible to reliably predict short-term mortality at the time of transfer decisions.
The 7-point scale was therefore pragmatically suited to our clinical context. Because the CFS is fundamentally a tool for assessing functional status rather than predicting mortality, we excluded the 8 patients who died from the functional analysis. This ensures that the relationship between VWF:Ag and recovery of functional capacity is assessed clearly among survivors.
Our study involved a relatively young population, approximately 10% of whom experienced mortality. Previous reports indicate that hospitalized deaths occur mainly in older patients^23)^ with cardiovascular disease and a history of chronic kidney disease (CKD).^24)^ Additionally, high-flow oxygen therapy or noninvasive ventilation (World Health Organization [WHO] scale 4) increases the risk of mortality.^25)^ Our findings are consistent with the published literature. Deceased patients showed lower lymphocyte counts^26)^ and serum albumin,^27)^ while exhibiting elevated D-dimer,^28)^ lactate dehydrogenase (LD),^29)^ interleukin-6 (IL-6),^30)^ and thrombomodulin (TM).^31)^ These results confirm that undernutrition indicated by lower albumin levels and extensive endothelial damage indicated by increased D-dimer, (LD), (IL-6), and TM are associated with worse outcomes.
Baseline levels of VWF:Ag and the VWF/ADAMTS13 ratio can predict functional outcomes at discharge. VWF is secreted from endothelial cells, megakaryocytes, or platelets.^32)^ Endothelial injuries during SARS-CoV-2 infection are highlighted as an indirect consequence caused by inflammatory signaling and hypoxic stress from infected epithelial cells, which leads to vascular dysfunction and immunothrombosis.^2)^ Platelet adhesion triggers the degranulation of α-granules, leading to VWF release.^33)^ Activated platelet-derived VWF contributes approximately 20% of total plasma VWF; both endothelial and platelet-derived VWF are responsible for elevated levels seen in SARS-CoV-2 infections. High VWF:Ag levels indicate significant endothelial damage, which aligns with clinical understanding.
Limitations
This single-center registry may limit the generalizability. However, the similarity in baseline characteristics and blood markers to previous reports suggests that our population did not differ substantially.
Conclusion
Levels of VWF:Ag and VWF/ADAMTS13 measured upon admission may help predict the functional status of hospitalized COVID-19 patients at discharge.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lamers MM, Haagmans BL. SARS-Co V-2 pathogenesis. Nat Rev Microbiol 2022; 20: 270–84.35354968 10.1038/s 41579-022-00713-0 · doi ↗ · pubmed ↗
- 2Won T, Wood MK, Hughes DM, et al. Endothelial thrombomodulin downregulation caused by hypoxia contributes to severe infiltration and coagulopathy in COVID-19 patient lungs. E Bio Medicine 2022; 75: 103812.35033854 10.1016/j.ebiom.2022.103812 PMC 8756077 · doi ↗ · pubmed ↗
- 3Wang P, Luo R, Zhang M, et al. A cross-talk between epithelium and endothelium mediates human alveolar-capillary injury during SARS-Co V-2 infection. Cell Death Dis 2020; 11: 1042.33293527 10.1038/s 41419-020-03252-9PMC 7721862 · doi ↗ · pubmed ↗
- 4Pons S, Fodil S, Azoulay E, et al. The vascular endothelium: the cornerstone of organ dysfunction in severe SARS-Co V-2 infection. Crit Care 2020; 24: 353.32546188 10.1186/s 13054-020-03062-7PMC 7296907 · doi ↗ · pubmed ↗
- 5Xu S-W, Ilyas I, Weng J-P. Endothelial dysfunction in COVID-19: an overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacol Sin 2023; 44: 695–709.36253560 10.1038/s 41401-022-00998-0PMC 9574180 · doi ↗ · pubmed ↗
- 6Bonaventura A, Vecchié A, Dagna L, et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat Rev Immunol 2021; 21: 319–29.33824483 10.1038/s 41577-021-00536-9PMC 8023349 · doi ↗ · pubmed ↗
- 7Mannucci PM. von Willebrand factor: a marker of endothelial damage? Arterioscler Thromb Vasc Biol 1998; 18: 1359–62.9743222 10.1161/01.atv.18.9.1359 · doi ↗ · pubmed ↗
- 8Sakai H, Goto S, Kim JY, et al. Plasma concentration of von Willebrand factor in acute myocardial infarction. Thromb Haemost 2000; 84: 204–9.10959690 · pubmed ↗