Side-by-side plastic stent insertion for refractory post-endoscopic sphincterotomy bleeding after covered metal stent placement
Takehiko Koga, Naoaki Tsuchiya, Yusuke Ishida, Makoto Fukuyama, Keisuke Matsumoto, Yi-Ling Ko, Fumihito Hirai

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
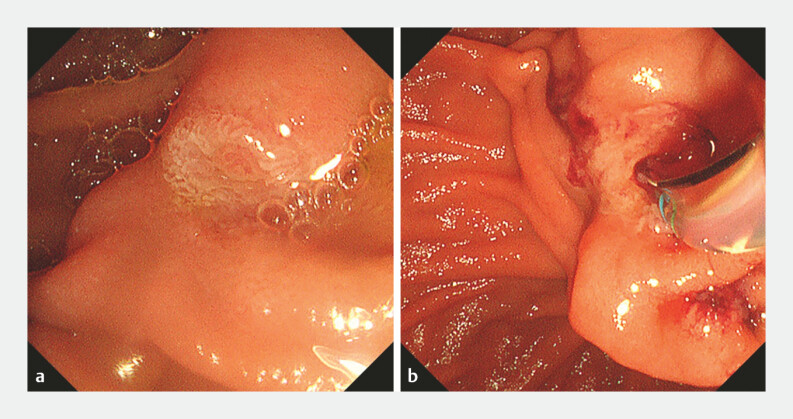 Fig. 1
Fig. 1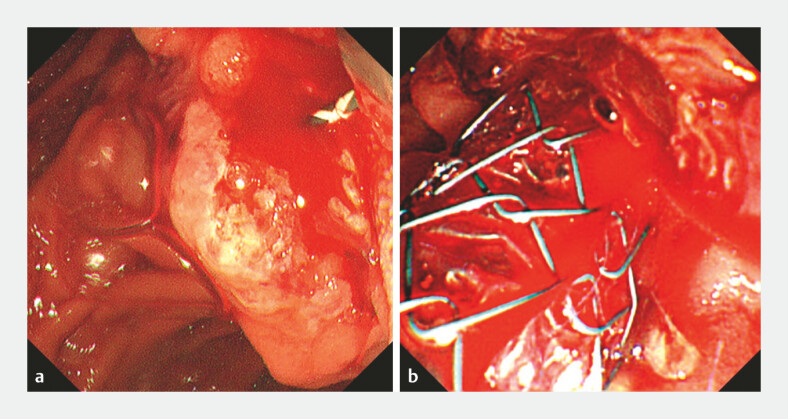 Fig. 2
Fig. 2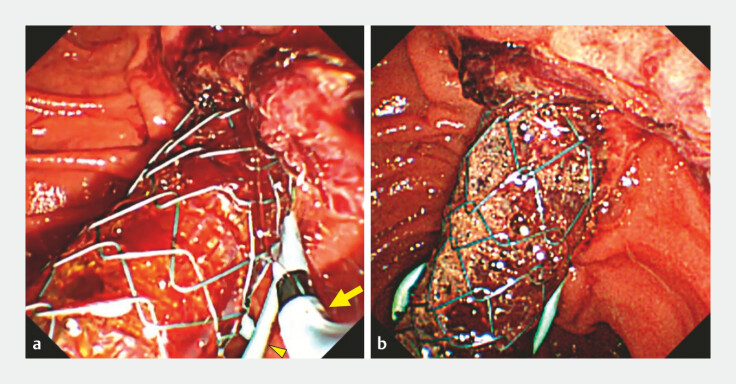 Fig. 3
Fig. 3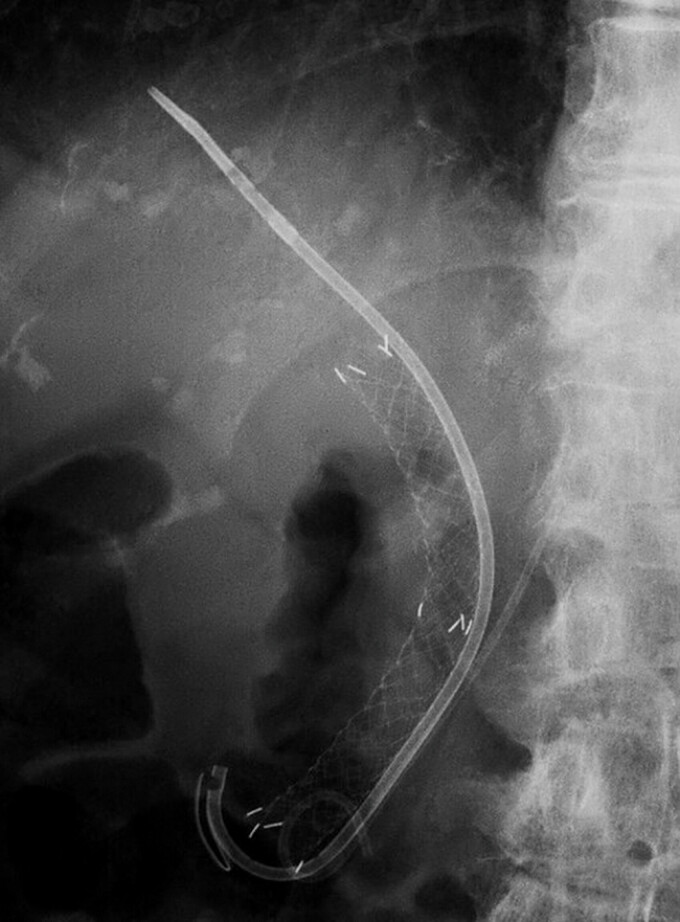 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Gastrointestinal Bleeding Diagnosis and Treatment
Post-endoscopic sphincterotomy (ES) bleeding is a common adverse event following endoscopic retrograde cholangiopancreatography (ERCP 1 ). The placement of a covered self-expandable metal stent (CSEMS) has been reported as an effective rescue hemostatic technique by providing mechanical compression at the duodenal papilla 2 3 . However, bleeding can occasionally persist despite the CSEMS placement 4 5 . Herein, we report a novel rescue hemostatic method for such challenging cases ( Video 1 ).
Rescue hemostasis with side-by-side plastic stent insertion for post-endoscopic sphincterotomy bleeding refractory to covered metal stent placement.Video 1
An 86-year-old woman with a history of Billroth I reconstruction underwent ERCP for distal biliary obstruction. After cholangiography, ES was performed ( Fig. 1 ), and continuous bleeding from the duodenal papilla occurred thereafter ( Fig. 2 a ). Initial endoscopic hemostasis using a balloon tamponade and hemostatic gel failed. A 5-Fr pancreatic plastic stent was placed to prevent post-ERCP pancreatitis, followed by deployment of a CSEMS (HANAROSTENT, 10 mm × 10 cm; M.I. Tech Co., Seoul, Korea). However, profuse bleeding persisted, and the source was unclear ( Fig. 2 b ). Subsequently, a 7-Fr plastic stent (ADFlap Stent, 14 cm; SILUX, Saitama, Japan) was inserted side-by-side with the CSEMS, providing additional compression to the duodenal papilla and achieving hemostasis ( Fig. 3 ). No rebleeding or adverse events occurred.
Endoscopic images before endoscopic sphincterotomy. a The duodenal papilla before endoscopic sphincterotomy. b Sphincterotome positioned at the papillary orifice just before incision.
Endoscopic images after endoscopic sphincterotomy. a Active bleeding from the duodenal papilla after endoscopic sphincterotomy. b Persistent bleeding despite the placement of a covered self-expandable metal stent.
Endoscopic images after additional plastic stent placement. a An endoscopic view showing the side-by-side placement of a plastic stent (arrow) beside the covered self-expandable metal stent, following the placement of a pancreatic plastic stent (arrowhead). b Hemostasis achieved after additional plastic stent placement.
In this case, the additional plastic stent was positioned on the anal side of the CSEMS, opposite to the sphincterotomy incision ( Fig. 4 ). This likely altered the angle and tension of the CSEMS, enhancing direct mechanical compression at the bleeding site. This simple modification may serve as a practical rescue technique when the CSEMS placement alone is insufficient, expanding its hemostatic potential in challenging post-ES bleeding.
A fluoroscopic image after the procedure. A fluoroscopic view showing the side-by-side placement of covered self-expandable metal and plastic stents.
Endoscopy_UCTN_Code_CPL_1AK_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Kapral C Aabakken LERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20205212714910.1055/a-1075-408031863440 · doi ↗ · pubmed ↗
- 2Shah JN Marson F Binmoeller KF Temporary self-expandable metal stent placement for treatment of post-sphincterotomy bleeding Gastrointest Endosc 2010721274127810.1016/j.gie.2010.08.01220951987 · doi ↗ · pubmed ↗
- 3Itoi T Yasuda I Doi S Endoscopic hemostasis using covered metallic stent placement for uncontrolled post-endoscopic sphincterotomy bleeding Endoscopy 20114336937210.1055/s-0030-125612621360425 · doi ↗ · pubmed ↗
- 4Saeed A Yousuf S Gangwani MK Efficacy and safety of fully covered self-expandable metal stents in the management of postsphincterotomy bleeding: systematic review and meta-analysis Gastrointest Endosc 202510111101.117E 639716535 10.1016/j.gie.2024.12.023 · doi ↗ · pubmed ↗
- 5Yoshida M Inoue T Naitoh I Practical Experiences of Unsuccessful Hemostasis with Covered Self-Expandable Metal Stent Placement for Post-Endoscopic Sphincterotomy Bleeding Clin Endosc 20225515015533207403 10.5946/ce.2020.217PMC 8831398 · doi ↗ · pubmed ↗