Improving Emergency Department Throughput in a Community Psychiatric Hospital Using a Structured Quality-Improvement Framework
Ryan Fudale, Anis Djerdjare

TL;DR
This study examines how psychiatric screening processes impact emergency department wait times in a community hospital and finds that these processes account for most of the delays.
Contribution
The study quantifies the impact of mandated psychiatric screening processes on emergency department throughput in a community psychiatric hospital.
Findings
PESS evaluation time accounted for nearly 60% of total emergency department length of stay.
Mean emergency department length of stay was 22.41 hours for encounters requiring PESS evaluation.
Variability in PESS workflow components suggests opportunities for system-level improvements.
Abstract
Background Emergency department (ED) overcrowding and prolonged length of stay (LOS) are pertinent challenges in psychiatric emergency care that have significant implications for patient safety, staff workload, and hospital efficiency. In particular, psychiatric emergency departments experience extended throughput delays due to limited inpatient capacity and external regulatory processes. In New Jersey, the Psychiatric Emergency Screening Services (PESS) is a mandated evaluation process that may contribute substantially to ED LOS, yet its quantitative impact has not been well characterized. This study aimed to quantify the contribution of PESS-related processes to emergency department LOS in a community psychiatric hospital. Methods This retrospective observational quality-improvement study analyzed consecutive psychiatric emergency department encounters at Bergen New Bridge Medical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
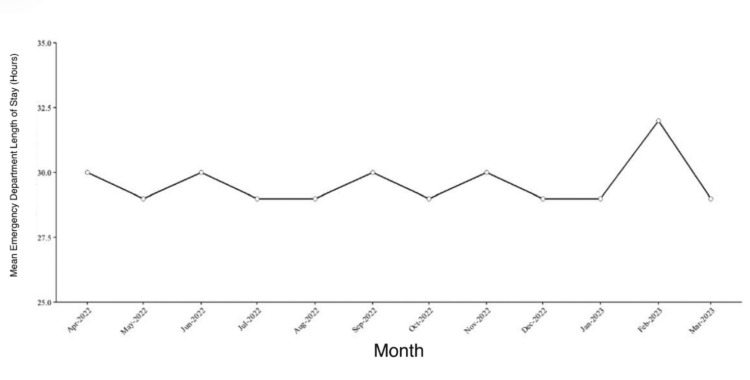 Figure 1
Figure 1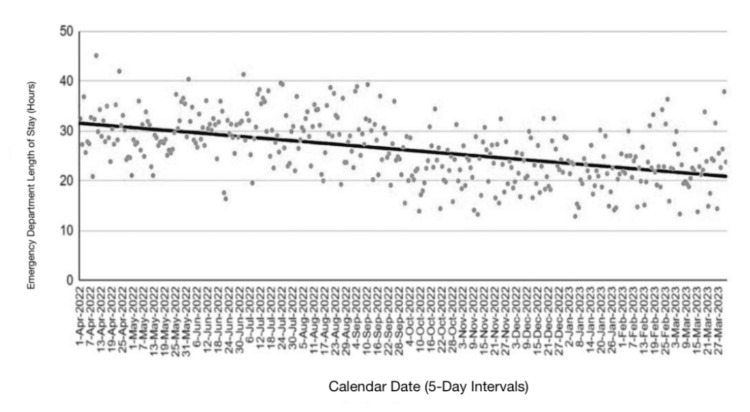 Figure 2
Figure 2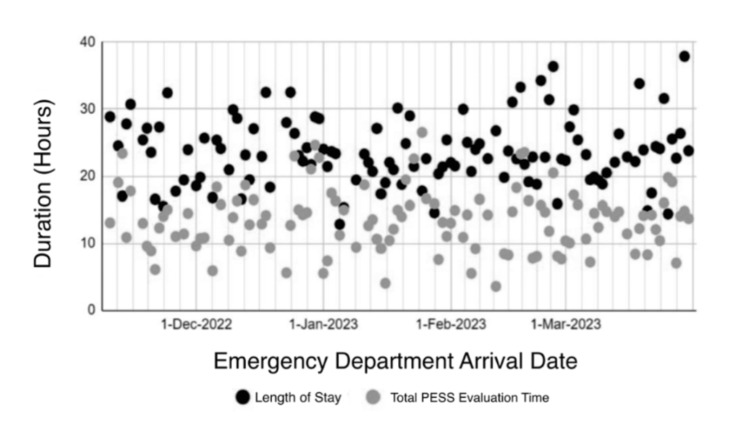 Figure 3
Figure 3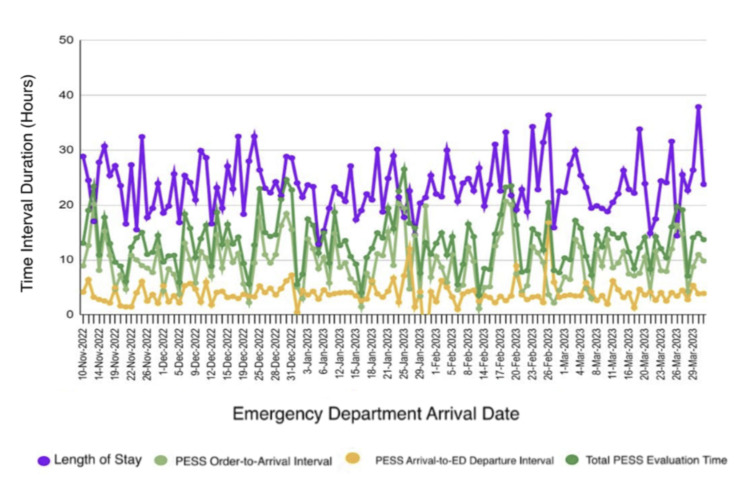 Figure 4
Figure 4| Metric | N (encounters) | Mean (hours) | SD | Median (hours) | IQR (hours) | % of total LOS |
| Total ED LOS | 118 | 22.41 | 4.90 | 22.42 | 19.38–24.94 | 100% |
| PESS evaluation time | 118 | 13.38 | 4.68 | 13.70 | 10.37–15.77 | 59.7% |
| Non-PESS ED time | 118 | 9.03 | 5.85 | 9.51 | 4.97–13.86 | 40.3% |
| PESS workflow component | N (encounters) | Mean (hours) | SD | Median (hours) | IQR (hours) | Min-max (hours) |
| PESS order to arrival | 118 | 9.45 | 4.44 | 9.20 | 5.90–12.01 | 1.12–20.70 |
| PESS arrival to ED departure | 118 | 3.93 | 2.01 | 3.62 | 2.78–4.47 | 0.47–16.81 |
| Total PESS evaluation time | 118 | 13.38 | 4.68 | 13.70 | 10.37–15.77 | 3.56–26.52 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmergency and Acute Care Studies · Psychiatric care and mental health services · Healthcare Decision-Making and Restraints
Introduction
Emergency department (ED) overcrowding in the United States has intensified over recent decades, negatively impacting patient safety, clinical outcomes, and hospital efficiency [1]. Increasing patient volumes and hospital admissions have placed sustained strain on emergency services, resulting in prolonged wait times and delayed disposition for many patients [2]. These challenges are particularly pronounced in psychiatric emergency care, where patients frequently experience extended lengths of stay (LOS) compared to those in general medicine EDs [3].
Psychiatric emergency departments face many distinct structural and operational constraints that complicate patient flow. Limited availability of inpatient psychiatric beds, heightened safety and monitoring requirements, and complex legal and disposition processes often delay transfer even after clinical stabilization [4]. Psychiatric patients may require continuous observation, specialized staffing, and placement, ultimately reducing flexibility in bed assignment and throughput [5]. As a result, psychiatric EDs are especially vulnerable to overcrowding and prolonged LOS.
In response to ED overcrowding, hospitals have implemented a variety of internal throughput interventions, including staffing model adjustments, triage redesign, and process standardization initiatives [6]. Prior studies have proven that such strategies can mobilize patient flow under certain institutional conditions, particularly when supported by sufficient staffing and infrastructure [7]. However, the effectiveness of these interventions appears to vary in different hospital settings. In psychiatric hospitals, there are also non-clinical restraints, such as regulatory requirements, that may limit the degree to which hospital-level operational changes alone can meaningfully reduce LOS [8].
One underexamined contributor to psychiatric ED throughput delays is the role of state-mandated screening services. In New Jersey, Psychiatric Emergency Screening Services (PESS) are required to evaluate patients for involuntary psychiatric admission and determine appropriate disposition [9]. While PESS plays a critical role in ensuring appropriate and legally compliant psychiatric placement, the timing and availability of these evaluations may introduce substantial delays in ED disposition, particularly when screening resources are limited or demand exceeds capacity [10]. Despite the central role of PESS in psychiatric emergency care, its quantitative contribution to overall ED LOS has not been well characterized.
Existing studies examining psychiatric ED throughput have largely focused on clinical workflows, staffing models, or inpatient bed availability, with limited attention to the measurable impact of state-mandated screening services [11]. Many analyses aggregate psychiatric and non-psychiatric ED populations, obscuring factors unique to psychiatric emergency care and limiting the applicability of findings to specialized psychiatric settings [12]. There remains a need for institution-specific and data-driven evaluations that isolate system-level contributors to LOS within psychiatric EDs, particularly in community hospitals that function as regional safety-net providers.
The objective of this study is to quantify system-level contributors to ED LOS in a community psychiatric hospital, with particular emphasis on the contribution of New Jersey's PESS to overall throughput delays. Using a retrospective observational quality-improvement framework, this study evaluates trends in psychiatric ED LOS over time and examines the relative impact of internal operational interventions compared with externally mandated screening services. By identifying dominant drivers of prolonged LOS, this analysis aims to inform future quality-improvement efforts and policy discussions focused on improving psychiatric emergency care delivery.
Materials and methods
This study was conducted as a retrospective observational quality-improvement analysis at Bergen New Bridge Medical Center (BNBMC), a community psychiatric hospital and safety-net institution located in Paramus, New Jersey, United States. BNBMC operates a psychiatric emergency department serving a large and diverse patient population and functions as a regional referral center for acute psychiatric care. The study evaluated emergency department throughput as part of a hospital-initiated Emergency Department Throughput Project using a Define-Measure-Analyze-Improve-Control (DMAIC) framework.
Study design and population
The analytic cohort consisted of 118 emergency department encounters involving psychiatric presentations that required PESS evaluation during the April 2022-March 2023 study period. All psychiatric emergency department encounters during the study period were eligible for inclusion, and no encounters were excluded. The analysis focused on system-level throughput metrics rather than individual clinical outcomes.
Data sources and collection
Retrospective operational data were generated from institutional hospital records and provided to the study team in de-identified Microsoft Excel (Microsoft, Redmond, Washington) format for analysis. Data included timestamps related to emergency department arrival, clinical processes, and disposition, as well as time intervals associated with PESS. Data were aggregated at the encounter level and reviewed for completeness prior to analysis. Demographic variables were not collected or analyzed as part of this operational quality-improvement study.
Outcome measure
The primary outcome was emergency department LOS, defined as the interval from emergency department arrival to emergency department departure. LOS was measured in hours and calculated for each encounter.
Process metrics and independent variables
To assess contributors to emergency department LOS, multiple throughput-related process metrics were examined. Door-to-triage time was defined as the interval from emergency department arrival to initial triage assessment. Door-to-doctor time was defined as the interval from arrival to the first documented provider evaluation. Door-to-bed time was defined as the interval from arrival to assignment to an emergency department treatment bed. Admission decision-to-departure time was defined as the interval from the clinical decision to admit or transfer to the patient's physical departure from the emergency department. Psychiatric emergency department LOS was defined as the total interval from emergency department arrival to departure.
Psychiatric Emergency Screening Services (PESS)-related time intervals were analyzed separately. Time from PESS order to PESS arrival was defined as the interval from placement of the PESS consultation order to the physical arrival of the PESS clinician in the emergency department. PESS arrival-to-emergency department departure time was defined as the interval from PESS clinician arrival to the patient's departure from the emergency department for inpatient admission, transfer, or discharge. Total PESS-attributable time was defined as the sum of the PESS order-to-arrival and PESS arrival-to-departure intervals.
These variables were selected based on their relevance to psychiatric emergency department workflows and their alignment with the Define-Measure-Analyze-Improve-Control (DMAIC) framework.
Quality improvement framework
DMAIC methodology guided the evaluation process. During the Define phase, operational bottlenecks affecting psychiatric emergency department throughput were identified through multidisciplinary review. In the Measure phase, baseline throughput metrics were established using collected operational data. The Analyze phase involved examining relationships between LOS and key process metrics to identify drivers of delay. In the Improve phase, targeted operational interventions were implemented, including expansion of psychiatric staffing coverage, triage workflow modifications, and communication standardization across emergency department units. The Control phase focused on monitoring throughput metrics over time to assess the sustainability of observed changes.
Statistical analysis
Descriptive statistics were used to summarize emergency department LOS and process metrics, including means and standard deviations. Temporal trends in emergency department LOS across the study period were evaluated using linear regression analysis, with calendar time treated as a continuous variable.
Linear regression analysis was also used to evaluate associations between LOS and key throughput variables, including total PESS time, given the continuous nature of these measures and the interest in estimating the strength and direction of linear relationships. Correlation coefficients were reported, and linear trendlines were fitted to visualize temporal patterns. Statistical significance was defined a priori as a two-tailed p-value of less than 0.05. Confidence intervals were not calculated due to limitations of retrospective aggregate operational data.
The proportion of total LOS attributable to PESS was calculated by dividing the mean total PESS duration by the mean total emergency department LOS. Data management was performed using Microsoft Excel, and statistical analyses were conducted using RStudio (R Foundation, Vienna, Austria).
Ethical considerations
This project was conducted as a quality-improvement initiative using de-identified retrospective operational data. It did not involve interaction with human subjects or use of identifiable private information and was therefore deemed exempt from institutional review board review.
Results
A total of 118 consecutive psychiatric emergency department encounters were included in the analysis. Emergency department length of stay (LOS) was evaluated across the 12-month study period from April 2022 through March 2023 to assess temporal trends and system-level contributors to prolonged stays.
Emergency department length of stay trends
The mean emergency department length of stay (LOS) over the study period was 22.41 hours (standard deviation (SD) 4.90 hours), calculated at the patient level across all encounters. Monthly mean LOS values fluctuated between approximately 28 and 32 hours and were calculated as unweighted monthly averages. As a result, months with fewer encounters but longer individual stays contribute equally to months with higher encounter volume. Although short-term variation in LOS was observed, no sustained reduction was evident following implementation of hospital-level throughput interventions. The monthly mean emergency department LOS across the study period is shown in Figure 1.
Monthly mean emergency department length of stay during the study periodEach point represents the mean emergency department length of stay for a given month.
Temporal analysis of emergency department LOS demonstrated substantial day-to-day variability across the study period. When aggregated into five-day intervals, linear regression analysis showed a moderate negative association between calendar time and LOS (r=-0.713, p=1.47 × 10⁻¹²), although considerable dispersion persisted throughout the observation period. Temporal variability in LOS and the associated linear regression trend are illustrated in Figure 2.
Emergency department length of stay aggregated in five-day intervalsEach point represents the mean emergency department length of stay aggregated over five-day intervals across the study period (N=73 intervals). The solid line represents the fitted linear regression trend over calendar time. Linear regression analysis demonstrated a moderate negative association between calendar time and emergency department length of stay (r=-0.713, p=1.47 × 10⁻¹²).
Impact of psychiatric emergency screening services
PESS-related processes accounted for a substantial proportion of total emergency department LOS among encounters requiring PESS evaluation.
Among these encounters, overall emergency department LOS demonstrated moderate variability. Mean LOS was 22.41 hours (SD 4.90), with a median of 22.42 hours (IQR 19.38-24.94). When LOS was examined at an aggregate level, total PESS evaluation time comprised a majority of emergency department LOS, whereas non-PESS emergency department time accounted for the remaining portion.
Aggregate summary statistics describing total emergency department LOS and its decomposition into PESS-related and non-PESS time are presented in Table 1.
Relationship between PESS duration and length of stay
Scatterplot analysis demonstrated a positive association between total PESS evaluation time and overall emergency department LOS, with encounters characterized by longer PESS durations generally exhibiting higher LOS values. The relationship between total PESS evaluation time and emergency department LOS across individual encounters is illustrated in Figure 3.
Relationship between emergency department length of stay and total psychiatric Emergency Screening Services (PESS) durationThe scatterplot shows individual data points for overall emergency department length of stay (LOS; black) and total Psychiatric Emergency Screening Services (PESS) evaluation time (gray), plotted against patient emergency department arrival dates.
To further characterize sources of variability within PESS-related time, individual PESS workflow components were examined separately. Time from PESS order to arrival, time from PESS arrival to emergency department departure, and total PESS evaluation time were analyzed to assess their relative distributions and dispersion across encounters. Descriptive statistics for these PESS workflow components are summarized in Table 2.
To further characterize variability in these workflow components across individual encounters, temporal patterns in emergency department length of stay and PESS-related time intervals were examined over the study period. Temporal trends in these workflow components are illustrated in Figure 4.
Emergency department length of stay and Psychiatric Emergency Screening Services (PESS) time intervals by arrival dateTime series plot showing emergency department length of stay (LOS) and Psychiatric Emergency Screening Services (PESS)-related time intervals for individual encounters plotted by emergency department arrival date. Displayed measures include total LOS, PESS order-to-arrival interval, PESS arrival-to-emergency department departure interval, and total PESS evaluation time, all reported in hours. Across encounters, total LOS ranged from 12.85 to 36.37 hours, PESS order-to-arrival time ranged from 1.12 to 20.70 hours, PESS arrival-to-departure time ranged from 0.47 to 16.81 hours, and total PESS evaluation time ranged from 3.56 to 26.52 hours.
Summary of key findings
Despite the implementation of multiple hospital-level operational interventions, including expanded psychiatric staffing coverage, triage workflow adjustments, and process standardization, improvements in emergency department LOS were modest and held substantial variability. In contrast, PESS-related processes consistently accounted for a large proportion of total LOS, with delays in screening availability and timing emerging as the dominant contributors to prolonged emergency department stays.
Discussion
Interpretation of key findings
In this retrospective quality-improvement analysis, externally mandated psychiatric screening processes accounted for a substantial proportion of emergency department length of stay in a community psychiatric hospital. Despite the implementation of multiple hospital-level throughput interventions, overall reductions in LOS were modest and held substantial variability over the study period. In contrast, PESS consistently represented a dominant component of prolonged LOS, accounting for approximately 59.7% of total emergency department time.
Prior studies have consistently shown that psychiatric patients experience longer emergency department lengths of stay than nonpsychiatric populations, largely due to boarding and disposition-related delays [3,4,11]. The present findings are consistent with this literature, demonstrating prolonged LOS despite the implementation of multiple hospital-level throughput interventions. This analysis extends prior work by quantifying the contribution of a state-mandated psychiatric screening process to overall LOS within a community psychiatric hospital setting. Unlike studies that focus primarily on inpatient bed availability or internal emergency department workflows, the present study highlights screening-related processes as a substantial system-level contributor to throughput delays.
The analysis quantifies the relative contribution of screening-related processes to overall throughput but does not imply that PESS is unnecessary or inappropriate. Rather, the results indicate that the timing and availability of mandated screening evaluations are operationally significant and may meaningfully influence emergency department flow in psychiatric settings.
Hospital-level interventions and system constraints
During the study period, several hospital-level operational interventions were implemented as part of ongoing quality-improvement efforts. These included adjustments to psychiatric staffing coverage intended to improve availability during periods of higher demand, modifications to triage workflows to facilitate earlier identification and prioritization of psychiatric patients, and standardization of communication and handoff processes across emergency department and psychiatric services.
Following implementation of these interventions, emergency department LOS demonstrated modest temporal improvement accompanied by substantial variability over time, rather than a consistent or sustained reduction. This pattern suggests that while internal operational changes may influence throughput under certain conditions, their impact may be limited when key components of patient flow depend on externally mandated processes and system-level constraints.
Importantly, this observation does not diminish the value of hospital-based quality-improvement initiatives. Rather, it highlights the practical challenges of achieving durable reductions in psychiatric emergency department LOS in settings where disposition and placement are influenced by regulatory requirements, availability of external screening services, and broader system capacity.
Role of psychiatric emergency screening services in throughput
Psychiatric Emergency Screening Services serve a critical function in ensuring that psychiatric admissions are legally compliant and clinically appropriate [9]. The present analysis does not question the necessity of these services. Rather, it demonstrates that delays occurring prior to screening arrival and variability in screening availability were closely associated with prolonged emergency department LOS.
The observation that screening-related time intervals constituted a large proportion of total LOS underscores the importance of viewing psychiatric emergency throughput as a shared responsibility across multiple system actors. From an operational standpoint, delays related to screening availability may represent a bottleneck that limits the effectiveness of otherwise optimized internal workflows. Quantifying this contribution provides a clearer understanding of where delays occur without attributing fault or intent.
Clinical and operational implications
Prolonged psychiatric emergency department LOS has important implications for patient safety, staff workload, and resource utilization. Extended stays frequently require continuous observation and specialized staffing, which may further constrain emergency department capacity and contribute to crowding. From a clinical perspective, prolonged boarding in emergency settings may delay access to definitive psychiatric treatment and increase patient distress.
The findings of this study suggest that efforts to reduce psychiatric emergency department LOS may benefit from approaches that extend beyond hospital-based workflow optimization to include broader system-level coordination. In settings where screening availability and disposition pathways are governed by external processes, internal operational changes alone may be insufficient to achieve durable improvements. Future investigations that examine alternative screening coordination models, integrate patient-level outcomes, or evaluate throughput across different regulatory environments may help clarify strategies for improving psychiatric emergency care delivery while preserving legal and clinical safeguards.
Limitations and scope of inference
This study has several limitations that should be considered when interpreting the findings. First, the analysis was conducted at a single community psychiatric hospital, which may limit generalizability to other institutions or regulatory environments. Second, the retrospective design and use of aggregate operational data precluded adjustment for patient-level clinical characteristics, acuity, or case mix. Third, the study focused exclusively on throughput metrics and did not assess clinical outcomes or patient experience measures.
Despite these limitations, the study has several strengths. The analysis included consecutive psychiatric emergency department encounters over a 12-month period, reducing the influence of short-term variation. The use of routinely collected, time-stamped operational data enabled objective characterization of emergency department length of stay and screening-related workflow components in a real-world clinical setting.
Additionally, while temporal associations between screening-related delays and LOS were observed, causal relationships cannot be inferred. The results should therefore be interpreted as an operational characterization of throughput patterns rather than an evaluation of screening effectiveness or policy appropriateness.
Conclusions
In this retrospective quality-improvement study, PESS accounted for a substantial proportion of emergency department length of stay in a community psychiatric hospital, while hospital-level throughput interventions were associated with only modest and variable changes. These findings describe system-level patterns of emergency department flow and should not be interpreted as causal or evaluative of screening effectiveness. Further study is needed to examine how mandated screening processes interact with hospital operations across diverse psychiatric emergency care settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Emergency department crowding: a systematic review of causes, consequences and solutions P Lo S One Morley C Unwin M Peterson GM Stankovich J Kinsman L 013201810.1371/journal.pone.0203316 PMC 611706030161242 · doi ↗ · pubmed ↗
- 2Modeling emergency department crowding: Restoring the balance between demand for and supply of emergency medicine P Lo S One Ansah JP Ahmad S Lee LH Shen Y Ong ME Matchar DB Schoenenberger L 016202110.1371/journal.pone.0244097 PMC 780297533434228 · doi ↗ · pubmed ↗
- 3Emergency department length-of-stay for psychiatric visits was significantly longer than for nonpsychiatric visits, 2002-2011 Health Aff (Millwood) Zhu JM Singhal A Hsia RY 169817063520162760565310.1377/hlthaff.2016.0344 · doi ↗ · pubmed ↗
- 4Boarding of mentally ill patients in emergency departments: American Psychiatric Association Resource document West J Emerg Med Nordstrom K Berlin JS Nash SS Shah SB Schmelzer NA Worley LL 6906952020193153932410.5811/westjem.2019.6.42422 PMC 6754202 · doi ↗ · pubmed ↗
- 5A quality measurement framework for emergency department care of psychiatric emergencies Ann Emerg Med Im DD Scott KW Venkatesh AK 5926058120233640262910.1016/j.annemergmed.2022.09.007 · doi ↗ · pubmed ↗
- 6Does rapid assessment shorten the amount of time patients spend in the emergency department?Br J Hosp Med (Lond) Jarvis P Davies T Mitchell K Taylor I Baker M 6486517520142538343710.12968/hmed.2014.75.11.648 · doi ↗ · pubmed ↗
- 7A conceptual model of emergency department crowding Ann Emerg Med Asplin BR Magid DJ Rhodes KV Solberg LI Lurie N Camargo CA Jr 1731804220031288350410.1067/mem.2003.302 · doi ↗ · pubmed ↗
- 8The impact of court-ordered psychiatric treatment on hospital length of stay: balancing legal and clinical concerns J Korean Acad Psychiatr Ment Health Nurs Shin J San Gabriel MC Ho-Periola A Ramer S Kwon Y Bang H 1811913120223589163110.12934/jkpmhn.2022.31.2.181PMC 9311333 · doi ↗ · pubmed ↗