Frantz Tumor (Solid Pseudopapillary Neoplasm) Mimicking an Infected Pancreatic Pseudocyst: A Case Report
Flaviano Junqueira, Murilo Henrique Pedrão Ferreira, Leticia Mancilla Lourenço, Everson Artifon

TL;DR
A rare pancreatic tumor was mistaken for an infected pseudocyst in a young woman, highlighting the need for histopathological confirmation for accurate diagnosis.
Contribution
This case report emphasizes the importance of considering Frantz tumor in the differential diagnosis of cystic pancreatic lesions in young women.
Findings
Frantz tumor can mimic an infected pancreatic pseudocyst in clinical presentation.
Histopathological examination is essential for accurate diagnosis of cystic pancreatic lesions.
Complete surgical resection of Frantz tumor is associated with excellent prognosis.
Abstract
Frantz tumor, or solid pseudopapillary neoplasm (SPN), is a rare pancreatic tumor of low malignant potential that predominantly affects young women. Its clinical presentation is often nonspecific, and the differential diagnosis from other cystic pancreatic lesions, such as pseudocysts, represents a significant challenge. We report the case of a 31-year-old previously healthy woman who presented with abdominal pain, initially diagnosed and treated as an infected pancreatic pseudocyst. Following the initial surgical intervention and antibiotic therapy, the persistence of imaging findings and subsequent histopathological results led to the definitive diagnosis of a Frantz tumor. The patient subsequently underwent a curative-intent pancreatoduodenectomy. This case highlights the difficulty in distinguishing cystic pancreatic lesions. The patient’s initial presentation, with a large fluid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
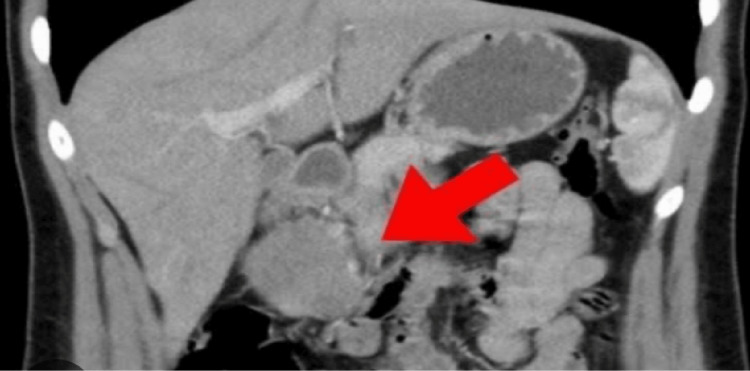 Figure 1
Figure 1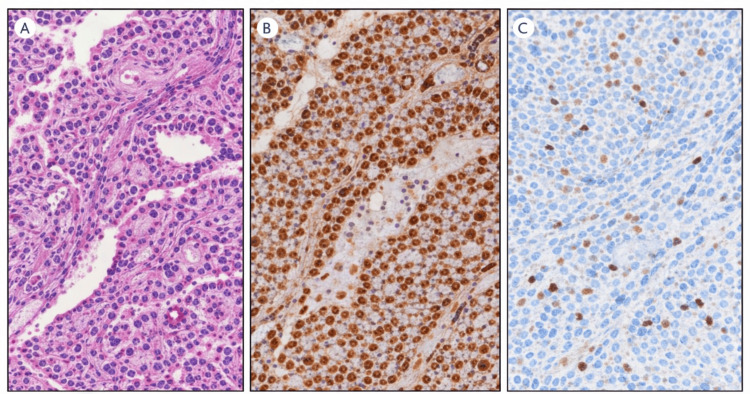 Figure 2
Figure 2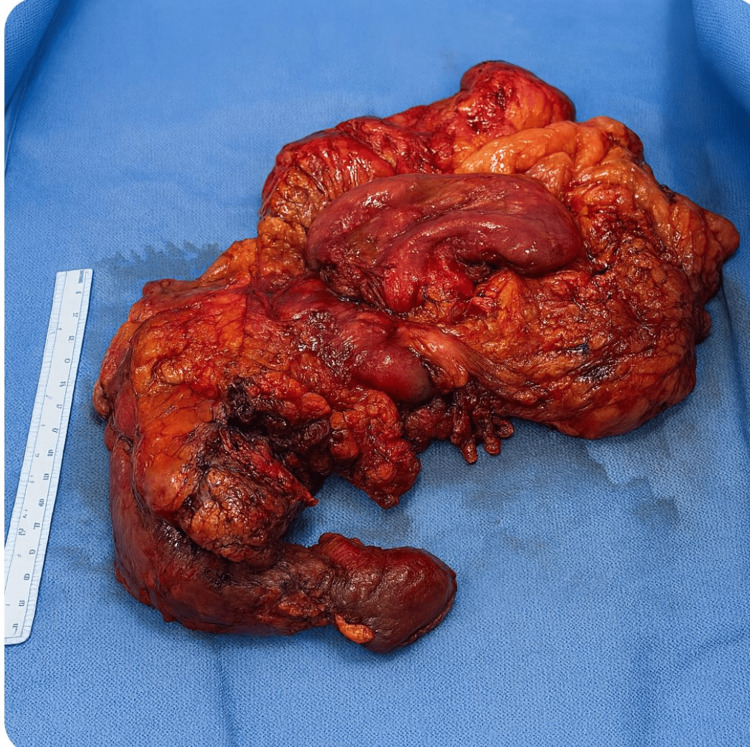 Figure 3
Figure 3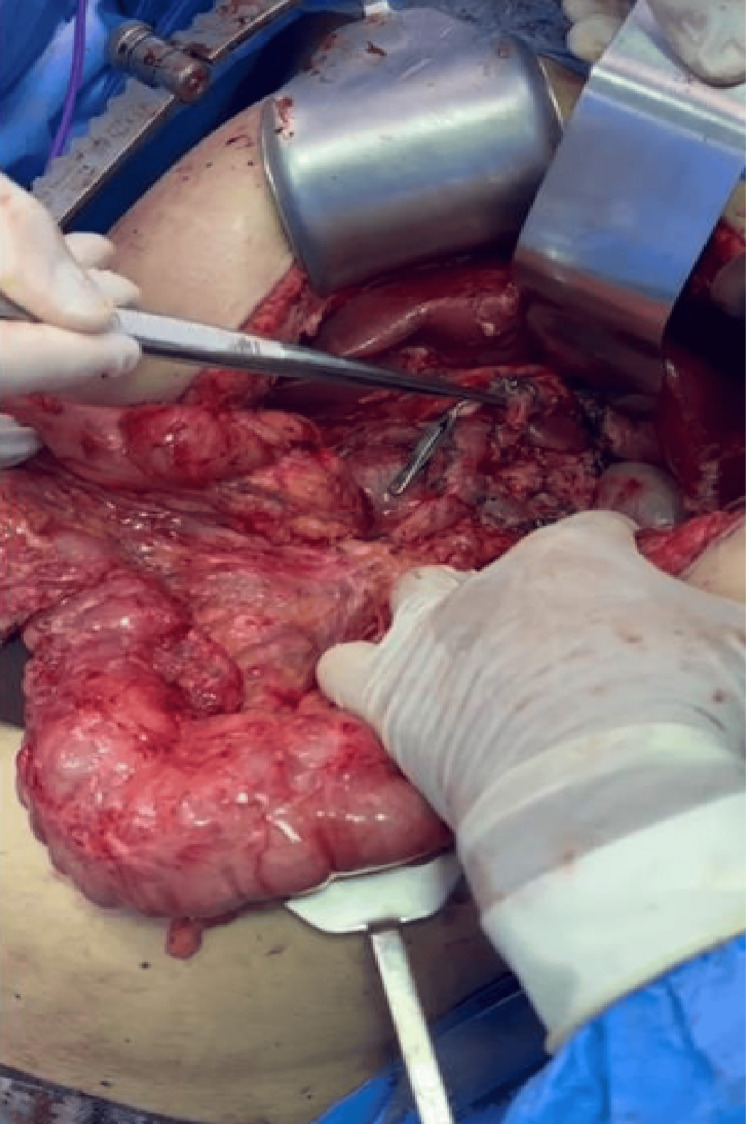 Figure 4
Figure 4| Test | Date 1 | Value 1 | Date 2 | Value 2 | Normal reference values |
| CEA | Day 64 | <0.5 | Day 126 | <0.5 | <3.0 ng/mL |
| CA 19-9 | Day 64 | 22.06 | Day 126 | 23.19 | <37.0 U/mL |
| CA 125 | Day 64 | 7.2 | Day 126 | 4.4 | <35.0 U/mL |
| Lipase | Day 75 | 19 | Day 158 | 8 | 10-140 U/L |
| Amylase | Day 75 | 18 | Day 159 | 28 | 25-125 U/L |
| CRP | Day 75 | 235.8 | Day 159 | 6.5 | <3.0 mg/L |
| Leukocytes | Day 75 | 22,44 | Day 159 | 8,88 | 4,000-11,000 cells/μL |
| Exam | Date | Relevant result |
| Endoscopic ultrasound | Day of presentation (Day 0) | Solid-cystic lesion in the pancreas. |
| Pathological anatomy (puncture) | Day 1 | Negative for malignancy (scarce material) |
| Abdominal MRI | Day 3 | Cystic formation with air-fluid level and gas (suspected infected pseudocyst) |
| Percutaneous drainage | Day 10 | Culture: |
| Surgery 1 (derivation) | Day 30 | Culture: |
| Pathological Anatomy (Final) | Day 60 | Solid pseudopapillary neoplasm (Frantz tumor) |
| Surgery 2 (Pancreatectomy) | Day 110 | Gastroduodenopancreatectomy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Pancreatitis Pathology and Treatment · Cholangiocarcinoma and Gallbladder Cancer Studies
Introduction
Solid pseudopapillary neoplasm (SPN) of the pancreas, also known as Frantz tumor, is a rare clinicopathological entity, accounting for only 1-2% of all exocrine pancreatic tumors [1,2]. First described by Virginia Frantz in 1959, this neoplasm characteristically affects young women, with an average age at diagnosis between 25 and 35 years, and is extremely rare in men [3].
Although classified by the World Health Organization (WHO) as a neoplasm with low malignant potential, SPN has an excellent prognosis after complete surgical resection, with five-year survival rates exceeding 95% [4]. The clinical presentation is usually insidious, with nonspecific symptoms such as abdominal pain or discomfort, or the palpation of an abdominal mass. In many cases, the diagnosis is incidental during imaging studies performed for unrelated reasons [5].
Radiologically, Frantz tumors typically appear as a well-defined, encapsulated mass with variable proportions of solid and cystic components, which may exhibit areas of hemorrhage or necrosis [1]. This heterogeneity can make the differential diagnosis challenging, including other cystic pancreatic lesions such as serous and mucinous cystadenomas, cystic neuroendocrine tumors, and, notably, pancreatic pseudocysts [6]. Confusion with pseudocysts is particularly relevant, as they are the most common cystic lesions of the pancreas and are generally associated with a history of pancreatitis.
This report describes a challenging case of a 31-year-old female patient whose initial diagnosis was that of an infected pancreatic pseudocyst, treated with drainage and antibiotic therapy, but whose subsequent investigation revealed a Frantz tumor. The purpose of this work is to emphasize the importance of including SPN in the differential diagnosis of complex cystic pancreatic lesions in young women, even in the absence of a typical clinical or radiological presentation.
Case presentation
A 31-year-old previously healthy female patient sought medical care on the day of presentation with complaints of abdominal pain. Initial investigation with endoscopic ultrasound revealed a solid-cystic lesion in the pancreas. Fine-needle aspiration biopsy was negative for malignancy, although with scarce material. The clinical picture evolved with worsening pain, nausea, and vomiting, prompting hospitalization on day 3. Imaging studies (CT and MRI) demonstrated a large pancreatic collection with an air-fluid level and gaseous foci, suggestive of an infected pseudocyst. The patient was treated with broad-spectrum antibiotic therapy (ceftriaxone and metronidazole) and subsequently underwent percutaneous drainage on day 10, with culture of the material revealing Streptococcus anginosus. The antimicrobial regimen was adjusted to teicoplanin and later to ciprofloxacin. Despite initial clinical improvement and reduction in collection volume on follow-up imaging, the patient underwent gastric derivation of the pseudocyst with cholecystectomy on day 30, due to the complexity of the case. Culture of the surgical material identified Staphylococcus epidermidis, and histopathological analysis of the cyst wall and adjacent pancreas showed fibrosis and acute-on-chronic inflammation (acute cholecystitis in the gallbladder). Surprisingly, the definitive histopathological analysis of the surgical specimen, whose result was released on day 60, diagnosed SPN (Frantz tumor).
This coronal CT image (Figure 1) highlights an SPN of the pancreas, indicated by the arrow, located in the pancreatic head. The radiological appearance demonstrates a well-defined mass with mixed solid-cystic components, a pattern frequently described in this low-grade malignant tumor that predominantly affects young women. This figure serves as a visual reference for the lesion’s typical anatomical position and structural characteristics within the pancreatic region.
Solid pseudopapillary neoplasm of the pancreatic head on the coronal CT scan
With the oncological diagnosis established, the patient was staged. Tumor markers (CA 19-9, CEA) were normal. After surgical risk assessment, she underwent gastroduodenopancreatectomy with retroperitoneal lymphadenectomy and Roux-en-Y reconstruction on Day 110, a procedure that occurred without complications.
Postoperative histopathological and immunohistochemical findings
Histopathological examination of the surgical specimen revealed an SPN characterized by pseudopapillary architecture, uniform neoplastic cells with eosinophilic cytoplasm, oval nuclei with nuclear grooves, and areas of hemorrhage and cystic degeneration. Surgical margins were free of tumor, and no lymph node metastasis was identified.
Immunohistochemical analysis demonstrated nuclear positivity for β-catenin and cyclin D1, with positivity for progesterone receptor and cytokeratin AE1/AE3. The Ki-67 proliferation index was low (<1%). Neuroendocrine markers, including chromogranin A and synaptophysin, were negative. This immunophenotypic profile is consistent with an SPN of the pancreas.
As shown in Figure 2, we observe the complete anatomical specimen obtained during the gastroduodenopancreatectomy procedure, which demonstrates the characteristic gross pathological features of an SPN. The resected tissue displays the typical heterogeneous appearance with both solid and cystic components, along with areas of hemorrhage and necrosis that are commonly observed in this type of pancreatic tumor.
Histopathological and immunohistochemical features of solid pseudopapillary neoplasm of the pancreas.(A) Hematoxylin and eosin staining showing pseudopapillary architecture with uniform tumor cells. (B) Nuclear accumulation of β-catenin on immunohistochemistry. (C) Low proliferative activity demonstrated by the Ki-67 labeling index.
The anatomical specimen was removed during gastroduodenopancreatectomy on day 110 (Figure 3).
Anatomical specimen removed during gastroduodenopancreatectomySource: Authors' own elaboration
As depicted in Figure 4, the intraoperative view during the pancreaticoduodenectomy reveals the complex anatomical relationships and the surgical technique employed for tumor resection. The procedure involved careful dissection of the pancreatic head, demonstrating the proximity of the lesion to vital structures, including the gastroduodenal artery and hepatic vessels. This intraoperative documentation illustrates the surgical approach and the technical considerations necessary for complete tumor removal.
Intraoperative view showing pancreatic head of approximately 4 cm and clipped gastroduodenal artery and hepatic arterySource: Authors' own elaboration
The diagnostic course, summarized in Tables 1-2, was prolonged and marked by an initial misinterpretation of the pancreatic lesion as an infected pseudocyst. Despite early imaging and endoscopic evaluation, the overlap between inflammatory findings and cystic degeneration delayed the recognition of an underlying neoplasm. Definitive diagnosis was achieved only after surgical intervention, underscoring the limitations of minimally invasive sampling in complex cystic pancreatic lesions.
Laboratory findings supported this diagnostic challenge. As shown in Table 1, conventional tumor markers remained within normal limits throughout the disease course, while inflammatory markers were markedly elevated during the infectious phase. This dissociation between inflammatory activity and stable pancreatic enzymes reinforced the atypical presentation of an SPN in this patient.
The chronological sequence of diagnostic procedures and therapeutic interventions is summarized in Table 2, which illustrates the evolution from initial presentation to definitive diagnosis and treatment.
Discussion
A Frantz tumor is a rare neoplasm that presents a diagnostic challenge due to its variable presentation. In the reported case, the initial manifestation as a complex cystic collection, with clinical and radiological signs of infection, led to a presumptive diagnosis of infected pancreatic pseudocyst. This atypical presentation is one of the diagnostic pitfalls described in the literature. What differentiates the present case is the presence of a clinically and radiologically confirmed infected pancreatic collection, with intralesional gas and positive microbiological cultures, mimicking an infected pseudocyst. The documented superimposed infection, associated with a negative initial endoscopic biopsy and the need for multiple therapeutic interventions, masked the underlying neoplasm and delayed the definitive diagnosis until postoperative histopathological examination.
Although most SPNs present as well-defined masses with solid and cystic components, extensive cystic degeneration, hemorrhage, and necrosis may lead to a purely cystic appearance, mimicking pseudocysts or cystadenomas [7,8]. The superimposition of an infection, as evidenced by the growth of Streptococcus anginosus and Staphylococcus epidermidis and by imaging findings, further complicated the differential diagnosis. The presence of gas within a pancreatic lesion is a strong indicator of infection, usually associated with infected pseudocysts or abscesses, but rarely described in uncomplicated SPNs. It is believed that the rapid growth rate of the tumor may exceed its blood supply, leading to central necrosis and, occasionally, communication with the pancreatic duct or gastrointestinal tract, which could facilitate secondary infection [9]. The gold standard treatment for Frantz tumor, regardless of size or presence of metastases, is complete surgical resection with negative margins [4]. The type of resection depends on the location and extent of the tumor, ranging from enucleation for small lesions to more radical procedures such as distal pancreatectomy or gastroduodenopancreatectomy, as performed in our patient. The prognosis after resection is excellent, even in cases with local invasion or metastases, which are rare at the time of diagnosis (approximately 10-15%) [3,10]. This case highlights the importance of histopathological confirmation for the definitive diagnosis of pancreatic cystic lesions. The initial fine needle aspiration was inconclusive, a common problem due to the heterogeneous nature of the tumor and the possibility of sampling necrotic or cystic areas. The final diagnosis was only possible after analysis of the surgical specimen, reinforcing the role of surgery not only as a therapeutic, but also as a definitive diagnostic tool in ambiguous cases.
Conclusions
This case report of a Frantz tumor mimicking an infected pancreatic pseudocyst highlights a significant diagnostic challenge. SPN should be maintained in the differential diagnosis of young women presenting with complex cystic lesions in the pancreas, even when signs and symptoms strongly suggest an infectious process. Complete surgical resection is the treatment of choice and offers a favorable prognosis, with histopathological confirmation being essential for adequate therapeutic planning.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Solid pseudopapillary tumor the pancreas Eurasian J Med Gursan N Yildirgan MI Atamanalp SS Sahin O Gursan MS 129132412009 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4261478/25610084 PMC 4261478 · pubmed ↗
- 2Frantz tumor: the tumor of young women. Radiologic-pathological correlation of two cases on tomography: literature review [Article in Spanish]Rev Med Tafur Anzola A Suarez Jiménez D 707712017
- 3Solid pseudopapillary tumors of the pancreas: review of 718 patients reported in English literature J Am Coll Surg Papavramidis T Papavramidis S 96597220020051592221210.1016/j.jamcollsurg.2005.02.011 · doi ↗ · pubmed ↗
- 4Solid pseudopapillary tumor of pancreas: a case report and review of literature Indian J Med Paediatr Oncol Sandlas G Tiwari C 207209382017 https://pmc.ncbi.nlm.nih.gov/articles/PMC 5582560/2890033110.4103/ijmpo.ijmpo_59_16PMC 5582560 · doi ↗ · pubmed ↗
- 5Frantz tumor: a case report of solid pseudopapillary tumor of pancreas Cureus Stefanova N Kalinov T Kolev N Kalchev E 0152023 https://pmc.ncbi.nlm.nih.gov/articles/PMC 10413994/
- 6Solid pseudopapillary neoplasm of the pancreas mimicking a pseudocyst of pancreas Med J Armed Forces India Jha BM Shah P Agarwal A 07712015
- 7Frantz's tumour of the pancreas presenting as a post-traumatic pancreatic pseudocyst Acta Chir Belg Hansson B Hubens G Hagendorens M Deprettere A Colpaert C Eyskens E 828499199910352738 · pubmed ↗
- 8Solid pseudopapillary tumor of the pancreas in male patients: report of 16 cases World J Gastroenterol Cai YQ Xie SM Ran X Wang X Mai G Liu XB 693969452020142494448610.3748/wjg.v 20.i 22.6939 PMC 4051935 · doi ↗ · pubmed ↗