Severe, Non‐apneic Respiratory Dysfunction and Hypoxia following Generalized Convulsive Seizures
Haley E. Pysick, Rup K. Sainju, Roshni Nair, Deidre N. Dragon, Eduardo Bravo, Laura Vilella, Xiaojin Li, Samden D. Lhatoo, George B. Richerson, Brian K. Gehlbach

TL;DR
This study shows that seizures can cause dangerous breathing and heart issues, even without stopping breathing, which may contribute to sudden deaths in epilepsy patients.
Contribution
The study identifies non-apneic respiratory dysfunction as a novel and significant risk factor for SUDEP.
Findings
Severe non-apneic respiratory dysfunction occurs frequently after generalized convulsive seizures.
Shallow or irregular breathing is linked to severe oxygen drops and slower heart rates.
Breathing and heart issues are closely connected after seizures.
Abstract
Sudden unexpected death in epilepsy (SUDEP) is a devastating consequence of some generalized convulsive seizures (GCS). Recent work has focused on seizure related apnea as a biomarker of SUDEP risk, frequently without characterizing the adequacy of non‐apneic ventilation or identifying other dysfunctional breathing patterns. We hypothesized that GCS frequently induce immediate, severe, non‐apneic respiratory dysfunction that can induce critical hypoxia and bradycardia and sought to characterize breathing patterns after GCS. Adult patients admitted to an epilepsy monitoring unit were studied. The effects of GCS on breathing and heart rate were analyzed using nasal pressure transducers, chest and abdominal respiratory inductance plethysmography, capillary oxygen saturation, transcutaneous CO2, electrocardiogram, electroencephalogram, and expert audiovisual analysis. Correlation analyses,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
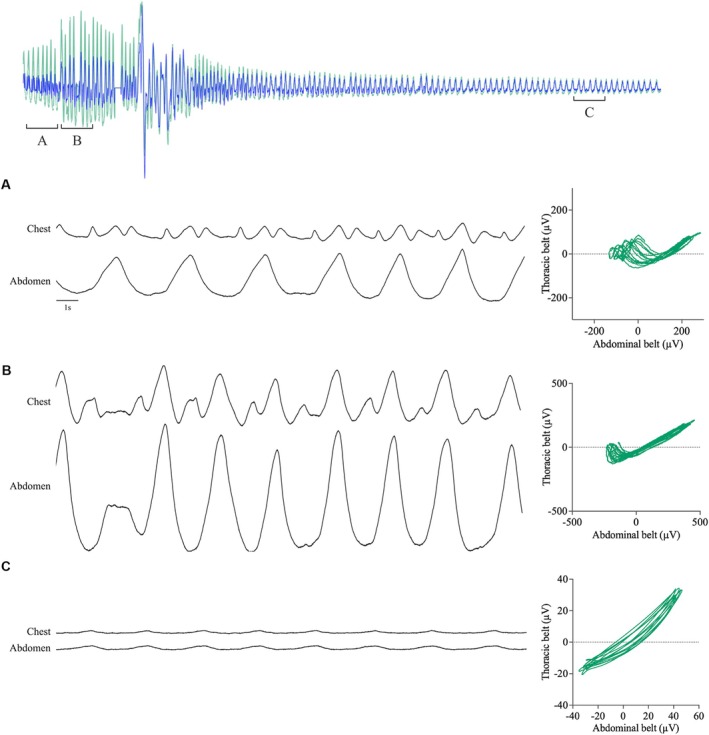 Figure 1
Figure 1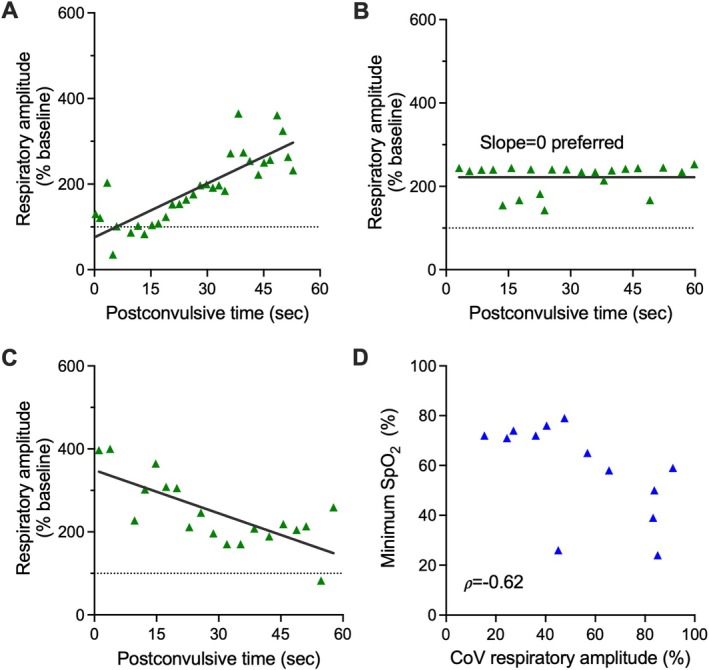 Figure 2
Figure 2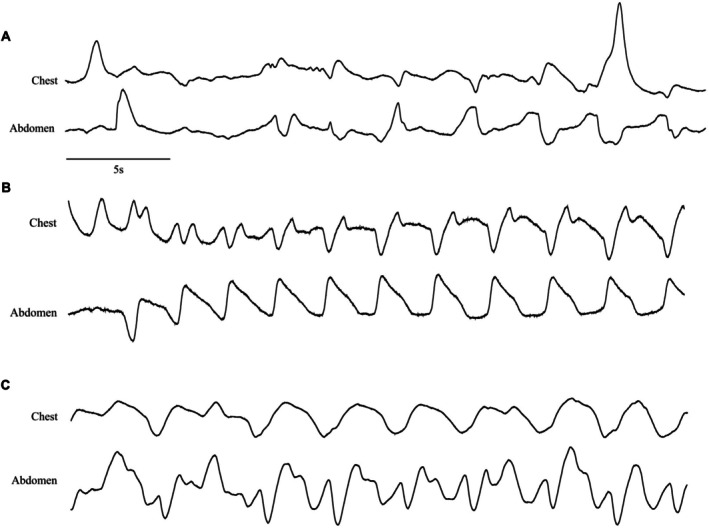 Figure 3
Figure 3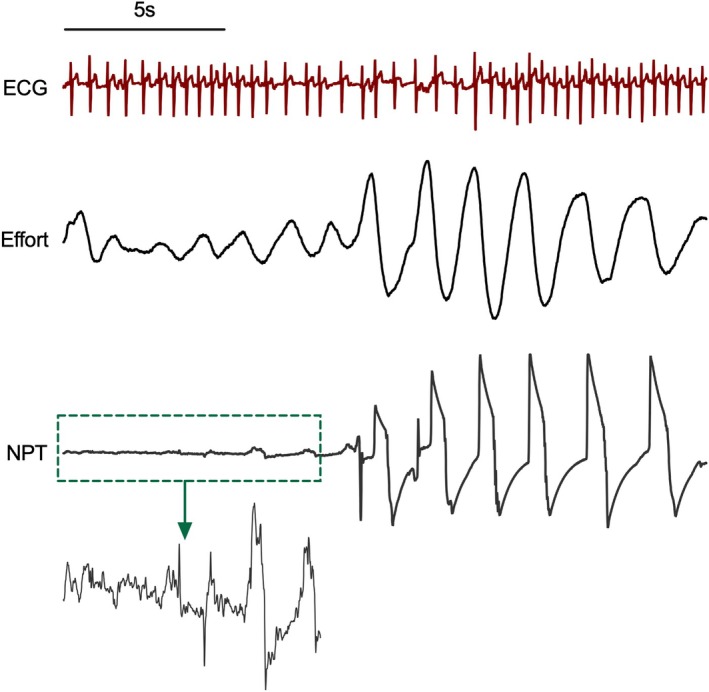 Figure 4
Figure 4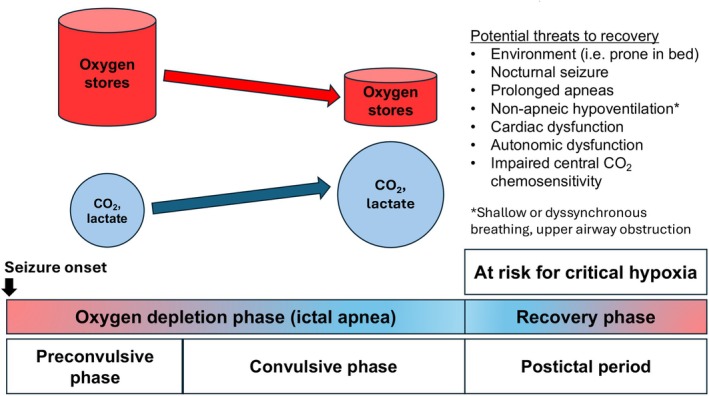 Figure 5
Figure 5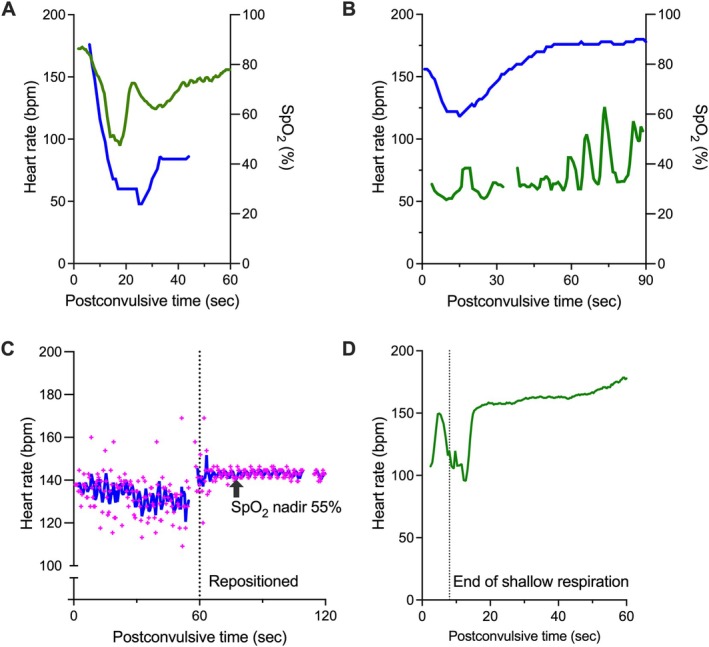 Figure 6
Figure 6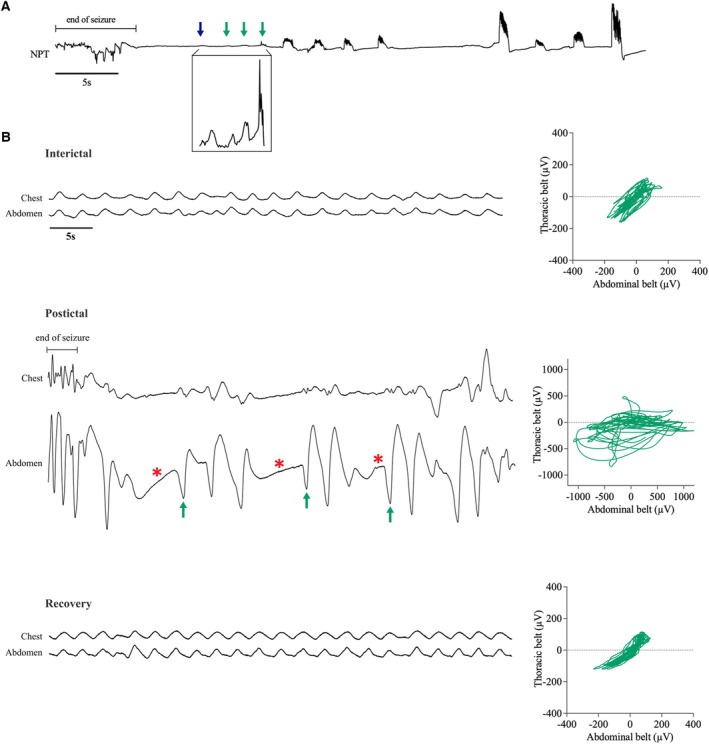 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEpilepsy research and treatment · Obstructive Sleep Apnea Research · Neuroscience of respiration and sleep
Introduction
Sudden unexpected death in epilepsy (SUDEP) is the leading category of premature death in people with epilepsy (PWE).^1^ The MORTEMUS study documented changes in electrocardiograms (ECG) and respiratory rates in patients who died of SUDEP in epilepsy monitoring units (EMUs).^2^ In 9 of the 11 SUDEP patients in whom both heart rate and respiratory rate could be measured, terminal apnea preceded terminal asystole, and all deaths occurred shortly after a generalized convulsive seizure (GCS). This sequence has since been replicated in multiple animal models of seizure-induced death.^3–5^
MORTEMUS was important in identifying respiratory dysfunction as the primary cause of death in some cases of SUDEP. Still, controversy remains regarding some of its findings. For example, it is sometimes noted^6, 7^ that cardiac changes, principally bradycardia and transient asystole, occurred before apnea in a subset of individuals, suggesting that cardiovascular dysfunction may have been the initiating event in those cases. This interpretation does not account for certain limitations in MORTEMUS, in which breathing was not directly measured but was retrospectively assessed through the analysis of video recordings and breathing artifacts on electroencephalography (EEG). While the authors suggested that hypoventilation may have also occurred in the absence of apnea, and in some cases described findings consistent with dysfunctional breathing, the design of the study precluded detailed characterization of non-apneic breathing patterns. Consequently, formal analyses of respiration focused on changes in the respiratory rate and the identification of 10-second central apneas. Since measurements of CO_2_ or O_2_ were not made, and non-apneic breathing patterns were not quantified, the possibility remains that some patients developed severe respiratory dysfunction and hypoxia that may have secondarily caused the observed cardiac changes.^4^
This possibility is critical to investigate, because while the ability of seizures to induce severe hypoxia is well established^8–10^, the optimal treatment of patients with bradycardia and/or hypoxia would depend on the cause of both the bradycardia (primary cardiac versus respiratory) and the hypoxemia. For instance, a patient with hypoxemia from upper airway obstruction would be expected in most cases to improve with repositioning, while a patient with central apnea would not. Similarly, while electrically pacing the heart would ameliorate postictal bradycardia, it would not improve ventilation or oxygenation.
We hypothesized that some seizures induce immediate, severe respiratory dysfunction and hypoxia and sought to characterize breathing patterns after GCS. We further hypothesized that respiratory dysfunction would modulate the heart rate and predispose to bradycardia. To test these hypotheses, we retrospectively analyzed all available respiratory data from a cohort of patients who underwent video-EEG and comprehensive cardiorespiratory monitoring in our EMU. Here we describe a variety of severe respiratory abnormalities in the immediate postictal period following nonfatal GCS that could have been missed in MORTEMUS by focusing on central apneas and would worsen the accrual of an oxygen debt that likely developed during the seizures.
Methods
Study design and participants
This study utilized data from prospectively enrolled patients admitted to the University of Iowa EMU between June 2015 and July 2023. Data from some participants have been reported previously as part of the multicenter Center for SUDEP Research or related studies.^11–22^ Participants were 18 years or older and had one or more GCS recorded during their inpatient EMU stay. Exclusion criteria included a history of stroke, active cardiac or pulmonary disease, space-occupying brain lesions, and known or potential pregnancy. Approval was obtained through the University of Iowa Institutional Review Board. All participants provided written consent.
Demographic and clinical variables were obtained via written questionnaire and query of the electronic medical record (see Supplement). This report adheres to all elements of the Strobe checklist for observational studies (www.strobe-statement.org/checklists/).
Video-electroencephalographic and cardiorespiratory monitoring
All patients underwent continuous video-EEG monitoring and peri-ictal care as directed by the clinical service. Scalp EEG electrodes were placed according to the international 10–20 system with the addition of T1 and T2 electrodes. Multimodal polygraphy included 3-lead electrocardiography (ECG), peripheral capillary oxygen saturation (SpO_2_), and transcutaneous CO_2_ (tcCO_2_) measurement. Thoracic and abdominal excursions were recorded using respiratory inductance plethysmography (RIP) and airflow was assessed using a nasal pressure transducer (NPT) and oronasal thermistor (see Supplement).
All seizures were reviewed by three investigators (HEP, RKS, and BKG) including a board-certified epileptologist (RKS) and board-certified pulmonary and critical care physician (BKG). Only seizures with evaluable O_2_/CO_2_ data from oximetry and/or tcCO_2_ data plus respiratory pattern data from appropriately positioned RIP belts and/or NPT were included. CO_2_/O_2_ data were analyzed as previously described (see Supplement).^19^ Duration of postictal generalized EEG suppression (PGES) was determined using an automated and validated tool^21, 23^ and supplemented by visual analysis when necessary. GCS ictal semiology was characterized as per Alexandre et al.^24^ Audio and video analysis was used to assess body position, upper airway sounds, accessory muscle use, and movement of the chest and abdomen; to confirm maintenance of stable positioning of the monitoring devices; and to identify artifact from muscle activity and nursing interventions.
Cardiorespiratory analyses
Postconvulsive breathing was analyzed in two stages. We first identified four breathing patterns through a comprehensive and iterative review of all audiovisual and signal data. Visual analysis of RIP belt waveforms was used to assess rate and regularity of breaths and to identify instances of thoracoabdominal asynchrony, defined as nonparallel movement of the thoracic and abdominal compartments. Konno-Mead plots were constructed to better visualize synchrony of thoracoabdominal wall motion.^25^ Instances of postconvulsive central apnea (PCCA) were defined as one or more missed breaths without any other explanation (i.e. movement or intervention), and of at least 5 seconds duration if occurring immediately after the end of the convulsive period.^16^ RIP belts were also used to qualitatively assess depth of respiration, which included the identification of grossly ineffective respiratory efforts, or “shallow breaths.” The NPT waveform was used to detect airflow limitation in the inspiratory and expiratory phases^26^ and to help identify instances of shallow breathing and/or irregularity.
Next, we quantified disordered rhythmicity and shallow breathing during the first 60 seconds of the postconvulsive period (see Supplement). For disordered rhythmicity we used a previously published method^11^ to analyze respiratory variability, which was expressed as the coefficient of variation of the inter-breath interval (CoV-IBI). To quantify the occurrence of shallow breathing we determined the amplitude of each breath, expressed as a percentage of baseline amplitude. Seizures associated with two or more breaths smaller than baseline were considered to exhibit shallow breathing. Changes in respiratory amplitude over time were modeled using linear regression.
The association between postconvulsive respiratory dysfunction and heart rate was analyzed after calculating R-R intervals (RRI) from the same period (see Supplement). Instantaneous heart rates were calculated as 1/RRI × 60 beats per minute (bpm). To identify potentially clinically relevant instances of bradycardia we determined the minimum heart rate for each postconvulsive period using a 4-beat moving average, with bradycardia defined as a heart rate < 60 beats per minute. Transient relative bradycardia was defined as an acute fall in heart rate by at least 40 bpm to a value below 100 bpm with rapid recovery to over 100 bpm.
Statistical analysis
Our statistical analysis plan had two major components. The first was to characterize the observed respiratory patterns and relate them to the development of critical hypoxia. For this reason, we focused on SpO_2_ nadir as our primary outcome of interest. Secondary outcomes included the associations between breathing patterns and duration of hypoxemia and the development of postictal hypercapnia. The second major component of our analysis was to analyze the association between the observed postconvulsive breathing patterns and heart rate.
Some patients had more than one evaluable GCS. All seizures were pooled for descriptions of seizure characteristics. For inferential statistical analyses, however, only the first evaluable GCS for each patient was used. Data were summarized as mean (SD) or median (IQR) depending on their distribution. Spearman’s ρ or Pearson’s r was used to examine the relationships between tcCO_2_ and SpO_2_ and selected clinical variables. An unpaired t-test or Mann-Whitney test was used to analyze differences between independent groups. The Wilcoxon matched-pairs signed rank test was used to analyze differences between baseline and postconvulsive CoV-IBI and heart rate. All tests were two-sided and p≤0.05 was considered statistically significant. Correction for multiple comparisons was not performed due to the exploratory nature of the study.
Results
Patient and seizure characteristics
A total of 270 patients were enrolled, of whom 59 had 106 GCS. No seizures were fatal. Twenty-two patients had 33 seizures with both (a) oximetry (n=28) and/or tcCO_2_ data (n=26) and (b) evaluable RIP belt (n=31) and/or NPT (n=15) data. One of these seizures (with SpO_2_, tcCO_2_, and RIP belt data) was subsequently excluded because the patient received extensive bag-mask ventilation during the convulsive and postconvulsive periods.
Patient and seizure characteristics are shown in Table 1. All (32/32, 100%) seizures were associated with some form of nursing intervention including suctioning (27/32, 84.4%) and/or repositioning (21/32 (65.6%). In nine seizures oxygen was administered; in the six seizures with an evaluable SpO_2_ this was performed 13.5 (−3.5–28.3) seconds after (and no sooner than seven seconds prior to) the time of occurrence of the SpO_2_ nadir.
The respiratory rate in the first minute following GCS ranged from 5 to 40 breaths per minute with a median of 21.5 (19.3–24.8). All seizures (n=32/32, 100%) demonstrated eventual tidal volume recruitment through a combination of increased inspiratory capacity (deeper inspiration) and active expiration, with video and RIP belt evidence of abdominal muscle activation below the interictal relaxation volume. Despite the modest increase in respiratory rate, hypercapnia was common after GCS, with a mean peak postictal tcCO_2_ of 57.2 ± 9.9 mm Hg in 21 GCS. Oxygen desaturation was also common and frequently severe, with SpO_2_ nadir <70% occurring in over half (13/22, 59.1%) of all evaluable seizures. The median time to SpO_2_ nadir (n=22) and peak tcCO_2_ (n=21) following the end of the convulsive period was 8.0 (0.8, 19.5) and 143.5 (100.3–194.3) seconds, respectively.
In analyses restricted to the first evaluable GCS from each patient, respiratory rate was unrelated to tcCO_2_ peak (n=17), magnitude of postictal increase in tcCO_2_ (n=17), or duration of increased tcCO_2_ (n=18; all p>0.17). Severity of oxygen desaturation as expressed by SpO_2_ nadir was similarly not associated with respiratory rate (r=0.035, p=0.91, n=13) or any of these tcCO_2_ variables (all p>0.34). In contrast, SpO_2_ nadir was negatively associated with duration of oxygen desaturation (r=−0.78, p=0.008, n=10), while the latter was also positively associated with duration of tcCO_2_ elevation (r=0.58, p=0.039, n=13). There was no relationship between SpO_2_ nadir and either vigilance state at seizure onset or duration of PGES (both p>0.66), see Supplement).
Of 32 seizures analyzed, 31 (96.9%) had evidence of one or more obviously or possibly dysfunctional breathing patterns. These patterns were classified into four categories: disordered rhythmicity, shallow breathing, thoracoabdominal asynchrony, and upper airway obstruction (UAO).
Disordered rhythmicity
PCCA occurred in 3 of 32 seizures (9.4%; Fig. 1A). In addition, many patients exhibited respirations that did not meet criteria for PCCA, but which were irregular and/or chaotic (Fig. 1A, 1B). Overall, respiratory variability (CoV-IBI) increased from baseline during the first 60 seconds of the postconvulsive period, from a median of 10.8 (6.3–18.0) % to 26.5 (19.3–41.3) %, p<0.0001, n=22. In 2 of 32 seizures (6.3%), there was one or more higher amplitude breaths immediately following the convulsive period before breathing transitioned to a more rapid, irregular pattern. Two seizures (6.3%) not scored as PCCA exhibited a pattern of “interrupted” expiration, which consisted of an apnea interposed between passive and active expiration (Fig. 1B).
Postconvulsive CoV-IBI was not significantly associated with SpO_2_ nadir (ρ=−0.52, p=0.073, n=13). There was also no relationship between postconvulsive CoV-IBI and either peak postictal CO_2_ (ρ=−0.24, p=0.35, n=17) or duration of hypercapnia (ρ= −0.23, p=0.37, n=18).
Shallow breathing
Overall respiratory amplitude increased during the first 60 seconds of the postconvulsive period to 273.2 (196.1, 448.3) % of baseline (n=30 GCS). Linear regression was used to map temporal trends in respiratory amplitude. Using this approach, the best-fit model of respiratory amplitude vs time had a positive slope in 12 seizures, a slope of zero in 12 seizures, and a negative slope in 4 seizures (Fig. 2A–C). Thus most, but not all, seizures were characterized by either an immediate increase in tidal volume that was maintained during the first minute of the postconvulsive period or by continued tidal volume recruitment throughout this period. Still, 12/32 (37.5%) seizures were characterized by two or more grossly ineffective respiratory efforts (amplitude less than interictal baseline despite high metabolic demand), termed “shallow breaths”. In two seizures from one patient, shallow breathing occurred between the end of the generalized convulsive period and the end of the electrographic seizure. In one of these cases, many of the shallow breaths recorded from RIP belts coincided with focal clonic activity of the supraclavicular muscle (an accessory muscle of respiration) as the EEG transitioned to predominantly involve the right frontal lobe. It is not clear whether this represented a causal relationship. Shallow breathing was also frequently irregular even when not accompanied by PCCA (Fig. 1A, 1B).
When present, shallow respiration usually occurred in the immediate postconvulsive period, in close temporal proximity to the development of critical oxygen desaturation. We therefore analyzed this relationship to assess the appropriateness of respiratory motor output during a vulnerable period. Seizures with at least two postconvulsive breaths shallower than baseline (n=7) were associated with a lower SpO_2_ nadir 58 (26–65) % vs 72 (65.8–76.8) %, p=0.047 than seizures without this finding(n=6). While overall respiratory amplitude during the first minute was unrelated to SpO_2_ nadir (ρ=0.22, p=0.47, n=13), the CoV of respiratory amplitude was negatively related to SpO_2_ nadir (ρ=−0.62, p=0.027, n=13, Fig. 2D).
Thoracoabdominal asynchrony
All seizures in patients with data available from both RIP belts (30/30, 100%) demonstrated in-phase (parallel) movements of the chest and abdomen during baseline, interictal breathing. In the postconvulsive period, a phenomenon was observed with 25 seizures (24/30, 80.0%) in which movement of the thorax and abdomen were out of phase with one another. There were two variations of this pattern.
Paradoxical breathing pattern in a 1:1 chest-abdomen ratio:
In these cases, the chest and abdomen moved in opposite directions but maintained a 1:1 ratio for the duration of the respiratory cycle. Fifteen seizures (15/30, 50.0%) had evidence of transient or sustained paradoxical breathing during the immediate postconvulsive period (Fig. 3A, 3B). In three of these seizures (3/15, 20.0%), paradoxical breathing was noted to substantially improve after re-positioning, consistent with alleviation of UAO.
Paradoxical breathing tended to persist for longer than shallow breathing, suggesting it may contribute to both the development of hypercapnia and prolonged hypoxemia. However, when compared with in-phase movement of the chest and abdomen we found no significant relationships between paradoxical breathing and either adequacy of ventilation (tcCO_2_ variables) or severity of oxygen desaturation (SpO_2_ nadir and duration of hypoxemia), although these analyses were limited by small sample sizes (see Supplement).
Paradoxical breathing pattern with biphasic or triphasic movement of the chest or abdomen:
In 16 seizures (16/30, 53.3%) the chest and abdomen moved at different rates for unclear reasons. Of these cases, 13 seizures (13/16, 81.3%) exhibited two inspiratory peaks in the chest belts compared to a single inspiratory peak in the abdominal belt (Fig. 3B). In 1 of 16 seizures (6.3%) we observed a 3:1 chest to abdomen ratio that decreased to 2:1 and then eventually 1:1, which may also be a manifestation of disordered rhythmicity. (Fig. 4).
In contrast, 5 of 30 seizures (16.7%) demonstrated biphasic abdominal movement during inspiration compared to a single chest movement (Fig. 3C). One seizure (1/30, 3.3%) first exhibited biphasic inspiratory peaks of the chest belt with a single abdominal excursion, but then transitioned to biphasic inspiratory peaks of the abdominal belt with a single inspiratory peak of the chest belt.
Upper airway obstruction
UAO was ascertained through a composite analysis of NPT tracings, the identification of 1:1 paradoxical breathing on RIP belts, and noisy upper airway sounds captured on audio-video recordings, with or without accessory muscle use. Nearly all seizures (30/32, 93.8%) exhibited at least 1 finding consistent with UAO. Even after excluding noisy upper airway sounds as a criterion, evidence of UAO was present in 26/32 (81.3%) GCS. As discussed above, 1:1 paradoxical breathing consistent with inspiratory UAO was observed to varying degrees in 15 of 30 seizures (50.0%; Fig. 3A, 3B). In 27 of 32 seizures (84.4%) patients exhibited noisy upper airway sounds, both inspiratory (21/32, 65.6%) and expiratory (27/32, 84.4%), the latter associated with grunting or lip fluttering. We also examined the NPT signal for flow limitation compatible with UAO. In 15 of 15 (100%) seizures with interpretable NPT data, waveforms exhibited inspiratory peak flattening consistent with inspiratory flow limitation (Fig. 5). In 6 of these cases (6/15, 40.0%), high-frequency inspiratory (5/15, 33.3%) and/or expiratory (5/15, 33.3%) oscillations were present on NPT tracings, consistent with variable upper airway resistance (Fig. 5). In some cases, UAO improved with repositioning, although the effects of this intervention were difficult to separate from the effects of co-interventions (i.e. stimulation and suctioning).
Cardiorespiratory relationships
In 29 GCS the median instantaneous heart rate during the first minute after the convulsive period ranged from 60.0 to 162.2 beats per minute (bpm) with a median of 134.8 (123.7–143.8) bpm. Using a four-point moving average the median heart rate nadir was 95.6 (81.9–113.4) bpm. Bradycardia occurred in two seizures and transient relative bradycardia in six (see Supplement).
Median heart rate increased from 72 (60.6–78) bpm interictal to 130.4 (120.1–143.8) bpm postconvulsive period, p<0.0001, n=21. Patients with absolute (2/21 [9.5%]) or transient relative (6/21 [20.7%]) bradycardia exhibited greater variability in respiratory amplitude than non-bradycardic patients (CoV respiratory amplitude 74.4 [53.9–89.7] % [n=8] vs 35.7 [22.9–56.1] % [n=14], p=0.0197). Bradycardic patients also exhibited longer duration of oxygen desaturation (209 [134.8–233.8] s, n=4 vs 94.5 [50.8–137.8] s, n=10, p=0.024 and a nonsignificantly lower SpO_2_ nadir (58.0 [31.5–62.0] %, n=5 vs 72 [55.3–75.5] %, n=8, p=0.059). There were no significant differences between these two groups in median CoV-IBI or respiratory amplitude (p≥0.21, see Supplement). In some cases, acute changes in heart rate occurred in close temporal proximity to changes in respiratory status (Fig. 6A–6C).
Long-term follow-up
Approximately 40 months after EMU admission a male > 30 years of age with generalized drug-resistant epilepsy since childhood and frequent nocturnal GCS died unexpectedly following a witnessed GCS at home. He initially recovered to the point of communicating with emergency medical services. During the subsequent ambulance ride he became anxious, short of breath, and hypoxemic prior to becoming unresponsive and experiencing a cardiac arrest. An autopsy revealed bilateral proximal pulmonary thromboembolism. The seizure reported in this study was characterized by perioral cyanosis and shallow breathing during the immediate postictal period, as well as by high respiratory amplitude variability, UAO, and relative bradycardia (Fig. 6D). See Fig. 6 and Supplemental Results for further details. All other patients were living at the time of this report.
Discussion
This study has several novel findings: (1) GCS frequently induce immediate, severe, non-apneic respiratory dysfunction and hypoxia. Nearly all GCS were characterized by one or more of the following patterns: disordered rhythmicity, shallow breathing, thoracoabdominal asynchrony, or UAO. (2) Postconvulsive breathing that is either shallow or irregular in amplitude is associated with more severe oxygen desaturation. (3) The occurrence of transient or relative bradycardia was associated with greater variability in the amplitude of postictal respiration. Overall, our findings in nonfatal GCS demonstrate that seizures frequently induce respiratory dysfunction severe enough to cause bradyarrhythmias^4^ of the kind witnessed immediately after fatal seizures in MORTEMUS.^2^
Until relatively recently, studies of SUDEP pathogenesis were primarily focused on cardiac etiologies.^27^ There is now accumulating evidence pointing to a primary respiratory defect in many cases of SUDEP.^28^ The current study “connects the dots” between seizure-induced respiratory and cardiac dysfunction while also showing the former is not limited to apnea. This is important, because in a recent multicenter study showing increased risk of SUDEP in patients with peri-ictal apnea, ictal and postictal central apnea were only observed in 36% and 43%, respectively, of all SUDEP/near-SUDEP cases.^29^ This means that the absence of peri-ictal apnea is not necessarily reassuring, and that there is an urgent need to develop more predictive biomarkers of SUDEP risk. We speculate that increased variability in the timing and amplitude of postconvulsive respiration identifies a tendency to seizure-induced instability of the respiratory network that, in certain contexts, could increase the risk of SUDEP. Of note, prior studies support the potential utility of interictal respiratory variability in predicting severity of postictal oxygen desaturation^11^ and, when measured during non-rapid eye movement sleep, SUDEP risk.^30^
This study is novel in its comprehensive multi-modal assessment of postictal respiration, involving analysis of audiovisual material and tcCO_2_, SpO_2_, airflow, and chest and abdominal RIP signal data by investigators with expertise in respiratory failure. This approach allowed us to characterize respiratory patterns that would have otherwise not been detected by conventional metrics such as respiratory rate. In fact, many of the patterns described above would be classified as having a “normal” respiratory rate but are markedly abnormal in the context of severe hypoxia and/or hypercapnia. As such, this study demonstrates a variety of respiratory abnormalities in the postictal period, both subtle and overt, that may themselves cause severely decreased ventilation and oxygenation. These findings are therefore consistent with those of MORTEMUS,^2^ whose authors described several different patterns of dysfunctional breathing but, because respiration was not directly monitored, were unable to comprehensively characterize them or relate them to oxygenation, ventilation, or the heart rate.
The metabolic effects of GCS are central to the interpretation of our findings. The forceful muscle contractions of GCS result in an acute CO_2_ load and lactic acidosis.^31^ In a different context, these stimuli would prompt central CO_2_ chemoreceptors to vigorously stimulate ventilation^32^ to restore homeostasis. Adequate ventilation is particularly important in the immediate postictal period because respiratory efforts during the tonic and clonic phases are frequently absent or ineffective, which together with the high metabolic demand from GCS causes oxygen stores to be depleted and predisposes the patient to critical hypoxia. Indeed, the SpO_2_ nadir in our study occurred a median of only eight seconds after the convulsive period ended, consistent with ictal apnea being the primary contributor to hypoxemia during the immediate postictal state (Fig. 7) and providing an additional stimulus to increase ventilation. In our study, however, breathing was frequently shallow, erratic, and less effective during the first minute postictally despite severe hypercapnia, consistent with the occurrence of seizure-induced depression of central CO_2_ chemoreceptors in some individuals.^13 33^ A failure to adequately respond to hypoxemia and hypercapnia may make patients vulnerable to harsh downstream effects: a cascade of failures that may present simply as bradycardia^4^ but may also cause a critical reduction in cardiac contractility^34,35^ and hypoperfusion of the brainstem and respiratory muscles. In this sequence, what began primarily as respiratory dysfunction and critical hypoxia leads ultimately to secondary cardiac dysfunction, terminal apnea, and cardiac arrest.
One patient in our study later died after a GCS, with the autopsy revealing bilateral proximal pulmonary thromboembolism. This death could be classified as SUDEP Plus, given that death “may have been due to the combined effect of both conditions”.^36^ Still, because the chain of events leading to death is not known, it is unclear whether the features of this patient’s peri-ictal physiology described in this report (Fig. 6) are relevant to his death.
UAO was a common finding in our cohort, affecting approximately 90% of all seizures. Postictal UAO is a well-known complication of GCS and has been highlighted by other investigators.^4, 16^ Our definition of UAO was composite and included examination of the NPT and RIP belt signal data and audiovisual review. Expiratory UAO in the form of grunting or lip fluttering was common, and its clinical significance is unclear. Inspiratory UAO is likely of greater importance, given that it causes hypoxemia and sometimes hypercapnia in otherwise normal patients with OSA. Upper airway dilator muscles receive tonic and phasic drive from the respiratory network, and this output is reduced during sleep and when consciousness is diminished, such as during conscious sedation and anesthesia. Audiovisual evidence of UAO is also apparent on our review of a recently published report of a patient who died of SUDEP while undergoing home video-EEG monitoring.^37^ Upper airway tone is partly mediated by motor output enhanced by serotonergic neurons involved in arousal.^38, 39^ Thus, the co-occurrence of UAO and hypoventilation are linked mechanistically. It is important to consider UAO clinically as supplemental oxygen may not be sufficient, and the patient may instead require repositioning, insertion of a nasopharyngeal airway, or intubation.
Similar to Vilella et al,^16^ we did not observe laryngospasm in our cohort. Laryngospasm has been reported during a focal seizure^40^ and after GCS,^41^ and animal models suggest it may be a cause of some SUDEP cases.^42^ However, the UAO in this study’s nonfatal seizures tended to rapidly improve, including sometimes by stimulation and repositioning, features more commonly associated with reduced upper airway tone than laryngospasm. Furthermore, the upper airway sounds in this study tended to be low and coarse, unlike the higher-pitch inspiratory stridor more characteristic of laryngospasm.
Nonparallel movement of the chest and abdomen is most commonly observed when the upper airway is obstructed, as in OSA. It is therefore likely that the cases of 1:1 paradoxical breathing we observed were due to UAO. However, we also observed other forms of thoracoabdominal asynchrony, including instances in which the abdomen and chest appeared to move at different rates. The etiology of these patterns is not clear. In such cases the work of breathing frequently appeared elevated, suggesting some of these instances of thoracoabdominal asynchrony represented adaptive responses to loaded breathing^43, 44^ from acidosis. Acute hypercapnia also reduces diaphragm contractility and endurance time, and we cannot rule out the possibility of diaphragmatic fatigue if this muscle was tonically contracted during the GCS.^5, 45^ Thus, some instances of thoracoabdominal asynchrony may reflect a strength-load imbalance between the diaphragm and the metabolic load from the GCS. In other cases, the asynchrony may represent dysfunction of respiratory rhythm generation by the brainstem.
Disordered rhythmicity occurred at some point during most seizures. Two seizures exhibited a pattern of “interrupted expiration” (Fig. 1B) that, to our knowledge, has not been described previously in this population. Similar findings, along with marked variability in breathing, have been reported in the immediate period after birth in humans.^46, 47^
The ratio of Type 1 to Type 3 GCS was lower in our study than has been reported elsewhere,^24^ possibly because of inter-rater variability in assessment or the relatively small sample size. We also reported a lower rate of PCCA in our study than was reported by Ochoa-Urrea et al.^15^ This may also reflect sampling differences or inter-rater variability in the identification of very low amplitude breaths (vs apnea).
Limitations and strengths
Our study has some limitations. First, many sensors were removed by patients or became dislodged or malpositioned during GCS. To ensure high-fidelity measurements, we carefully reviewed the signal data and position of all devices and restricted our analyses to only high-quality recordings. This decreased the power of our study and limited our ability to conduct some analyses. Second, our analyses of RIP data do not permit us to precisely quantify tidal volume and should be considered semiquantitative. Third, while it is likely that various nursing interventions improved the cardiorespiratory status of some patients (Fig. 6C),^48^ our study was not powered to formally assess this effect. Fourth, because the seizures in this study were nonfatal, we were unable to directly observe cardiorespiratory changes leading to death. Finally, because this was an exploratory study we did not adjust our analyses for multiple comparisons^49^. This approach increases the risk of a false discovery. Thus, the inferences made from our statistical tests should be considered hypothesis-generating, albeit in many cases highly plausible biologically, and should be replicated in a larger cohort.
There are also strengths to this study, including our comprehensive approach to analyzing respiration using metrics not routinely measured in other studies. In every case, video and signal data from the postictal period were reviewed multiple times by the investigators to analyze and integrate multiple sources of complex data. This approach allowed us to characterize the adequacy of ventilation in our patients more comprehensively than prior studies that relied solely on measurements of respiratory rate and oxygen saturation and the visual identification of central apneas. It also permitted the association between dysfunctional breathing and heart rate to be analyzed, highlighting the interdependence of cardiac and respiratory function in the postictal state^22^.
Conclusions
The results of this study show that GCS frequently cause immediate and severe respiratory dysfunction and hypoxia in the absence of frank apnea, and that this respiratory dysfunction is closely associated with changes in heart rate. This suggests some of the immediately postictal bradyarrhythmias observed in MORTEMUS may have been caused by critical hypoxia that occurred before any significant respiratory dysfunction was detected using visual observation and EEG analysis. These data will also guide the identification of high-risk patients who might require different approaches to the prevention of SUDEP. Defining the sequence of events leading from seizures to death will require direct measurements of all relevant pathological variables, including CO_2_, O_2_, efficacy of alveolar ventilation, and electrocardiogram.
Supplementary Material
Supp Text
Supp F1Supplemental Figure 1. Upper airway obstruction evident on NPT tracing. Flattening of the inspiratory peak and high-frequency oscillations in both inspiratory and expiratory phases is demonstrated. NPT = nasal pressure transducer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thurman DJ, Hesdorffer DC, French JA. Sudden unexpected death in epilepsy: Assessing the public health burden. Epilepsia. 2014;55(10):1479–85.24903551 10.1111/epi.12666 · doi ↗ · pubmed ↗
- 2Ryvlin P, Nashef L, Lhatoo SD, Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): a retrospective study. Lancet Neurol. 2013;12(10):966–77.24012372 10.1016/S 1474-4422(13)70214-X · doi ↗ · pubmed ↗
- 3Buchanan GF, Murray NM, Hajek MA, Richerson GB. Serotonin neurones have anti-convulsant effects and reduce seizure-induced mortality. J Physiol. 2014;592(19):4395–410.25107926 10.1113/jphysiol.2014.277574 PMC 4215784 · doi ↗ · pubmed ↗
- 4Kim Y, Bravo E, Thirnbeck CK, Severe peri-ictal respiratory dysfunction is common in Dravet syndrome. J Clin Invest. 2018;128(3):1141–53.29329111 10.1172/JCI 94999 PMC 5824857 · doi ↗ · pubmed ↗
- 5Wenker IC, Teran FA, Wengert ER, Postictal death is associated with tonic phase apnea in a mouse model of sudden unexpected death in epilepsy. Ann Neurol. 2021;89(5):1023–35.33604927 10.1002/ana.26053 PMC 8411945 · doi ↗ · pubmed ↗
- 6Bagnall RD, Crompton DE, Semsarian C. Genetic Basis of Sudden Unexpected Death in Epilepsy. Front Neurol. 2017;8:348.28775708 10.3389/fneur.2017.00348 PMC 5517398 · doi ↗ · pubmed ↗
- 7Farrenburg M, Rali A, Grodzinsky A, Landazuri P. Cardiology perspective on seizure-related bradyarrhythmias and SUDEP: A survey study. Epilepsy Behav. 2021 Sep;122:108188.34252834 10.1016/j.yebeh.2021.108188 · doi ↗ · pubmed ↗
- 8Nashef L, Walker F, Allen P, Sander JW, Shorvon SD, Fish DR. Apnoea and bradycardia during epileptic seizures: relation to sudden death in epilepsy. J Neurol Neurosurg Psychiatry. 1996 Mar;60(3):297–300.8609507 10.1136/jnnp.60.3.297PMC 1073853 · doi ↗ · pubmed ↗