Wildfire-specific fine particulate matter and preterm birth: a US ECHO Cohort analysis
Allison R Sherris, Logan C Dearborn, Dana E Goin, Christine T Loftus, Adam A Szpiro, Joan A Casey, Sindana D Ilango, Jyoti Angal, Deborah H Bennett, Miatta A Buxton, Carlos A Camargo, Kecia N Carroll, Marissa L Childs, Camille Cioffi, Lisa A Croen, Dana Dabelea, Stephanie M Eick

TL;DR
Wildfire smoke exposure during pregnancy is linked to higher odds of preterm birth, especially in the western US and during mid-to-late pregnancy.
Contribution
This study identifies a potential exposure-response relationship between wildfire PM2.5 and preterm birth in a large US cohort.
Findings
Exposure to wildfire PM2.5 was associated with increased odds of preterm birth in the western US.
Higher exposure intensity and duration correlated with greater preterm birth risk.
Mid-to-late pregnancy smoke exposure was linked to preterm birth at the national level.
Abstract
Exposure to PM2·5 from wildfire smoke during pregnancy has been implicated as a risk factor for preterm birth. We investigated this association in the prospective nationwide US Environmental Influences on Child Health Outcomes (ECHO) Cohort, focusing on prenatal wildfire PM2·5 exposure intensity, duration, and timing. In this cohort analysis, we included live singleton births recorded in the ECHO Cohort with available data on gestational age at birth and birthweight and dates of conception between Jan 1, 2006, and March 20, 2020. Census tract-level estimates of daily mean wildfire-derived PM2·5 for the years 2006–20 from a previous machine learning model were linked to residential address history. We calculated the mean concentration of daily wildfire PM2·5, days with wildfire PM2·5 (>0, ≥2·5, ≥5·0, and ≥10·0 μg/m3; termed smoke days) and consecutive smoke days (2, 3, or ≥4 days;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
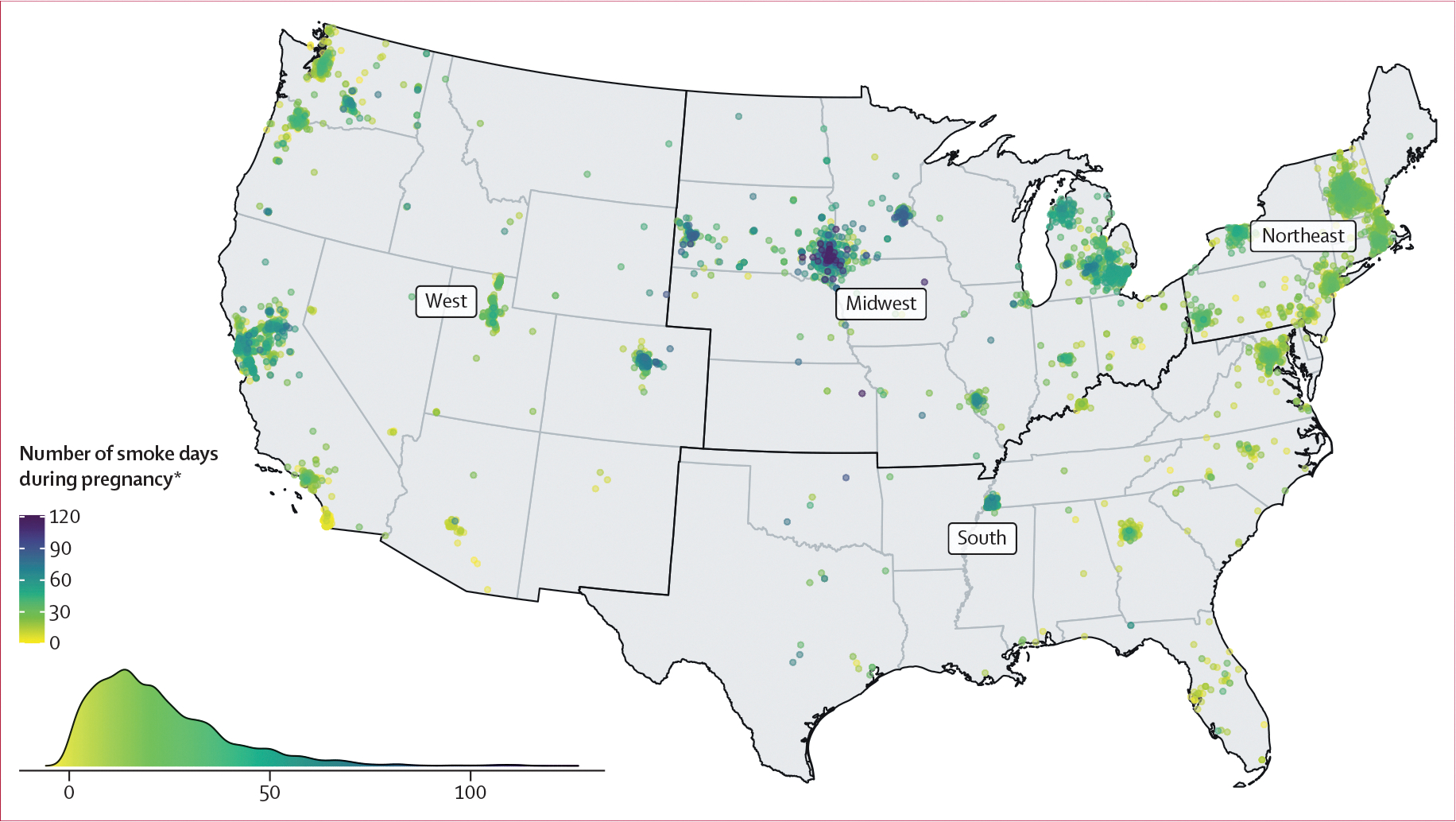 Figure 1
Figure 1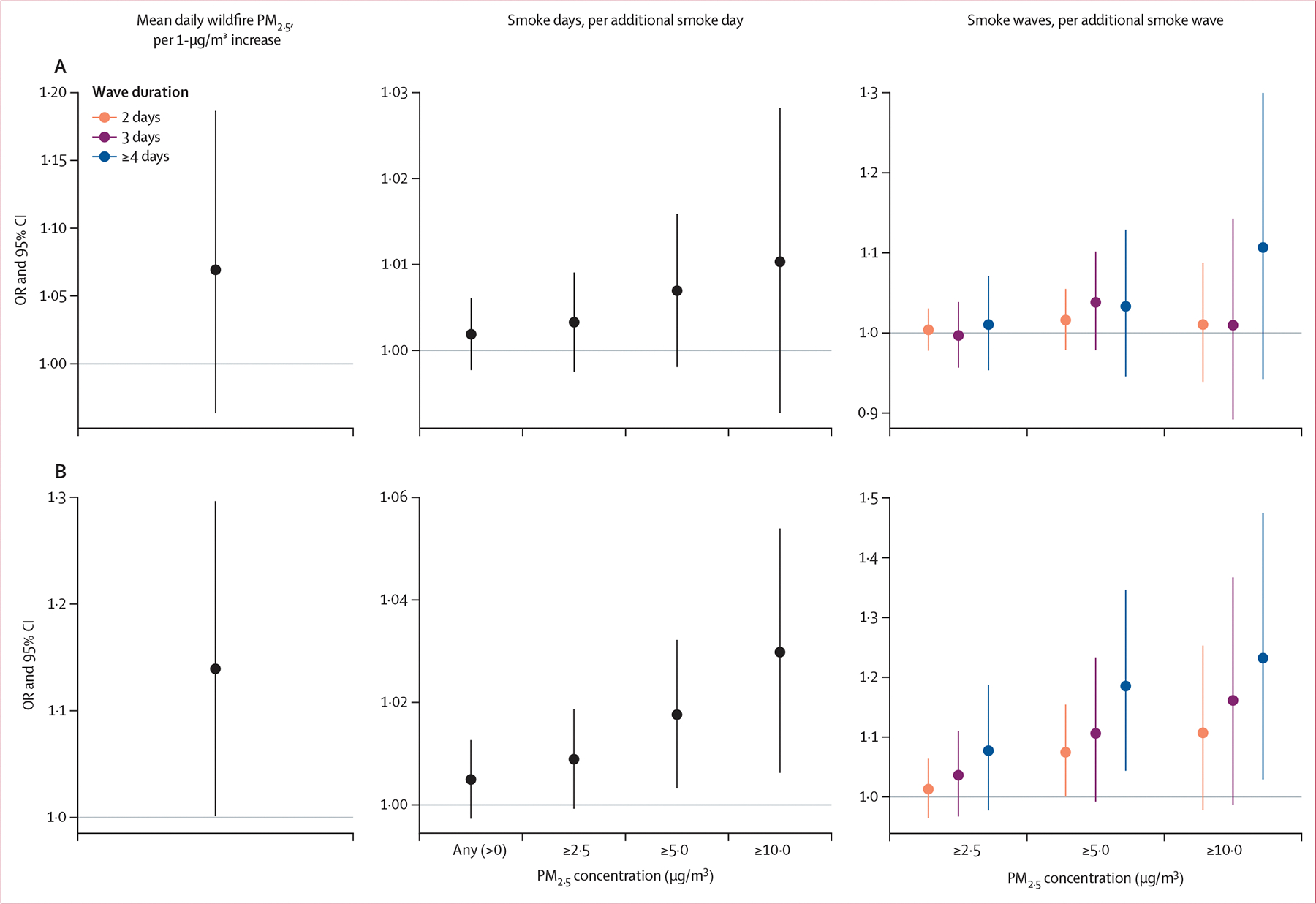 Figure 2
Figure 2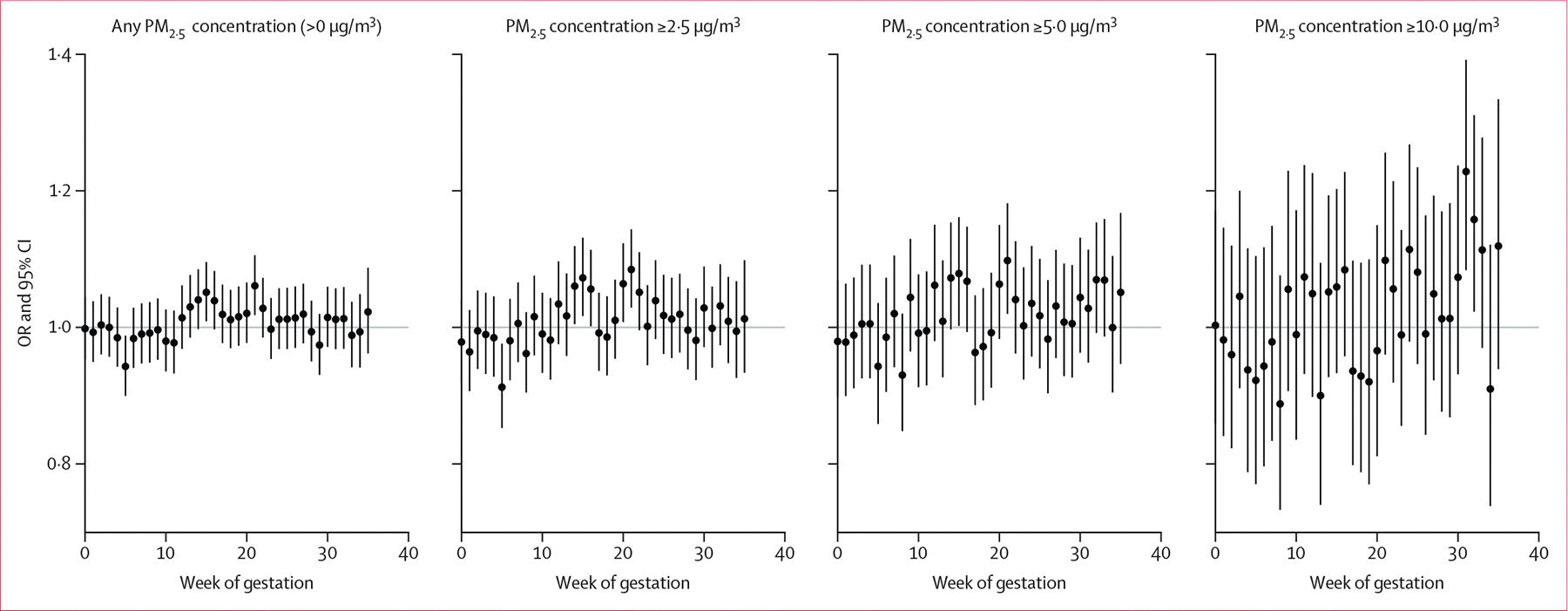 Figure 3
Figure 3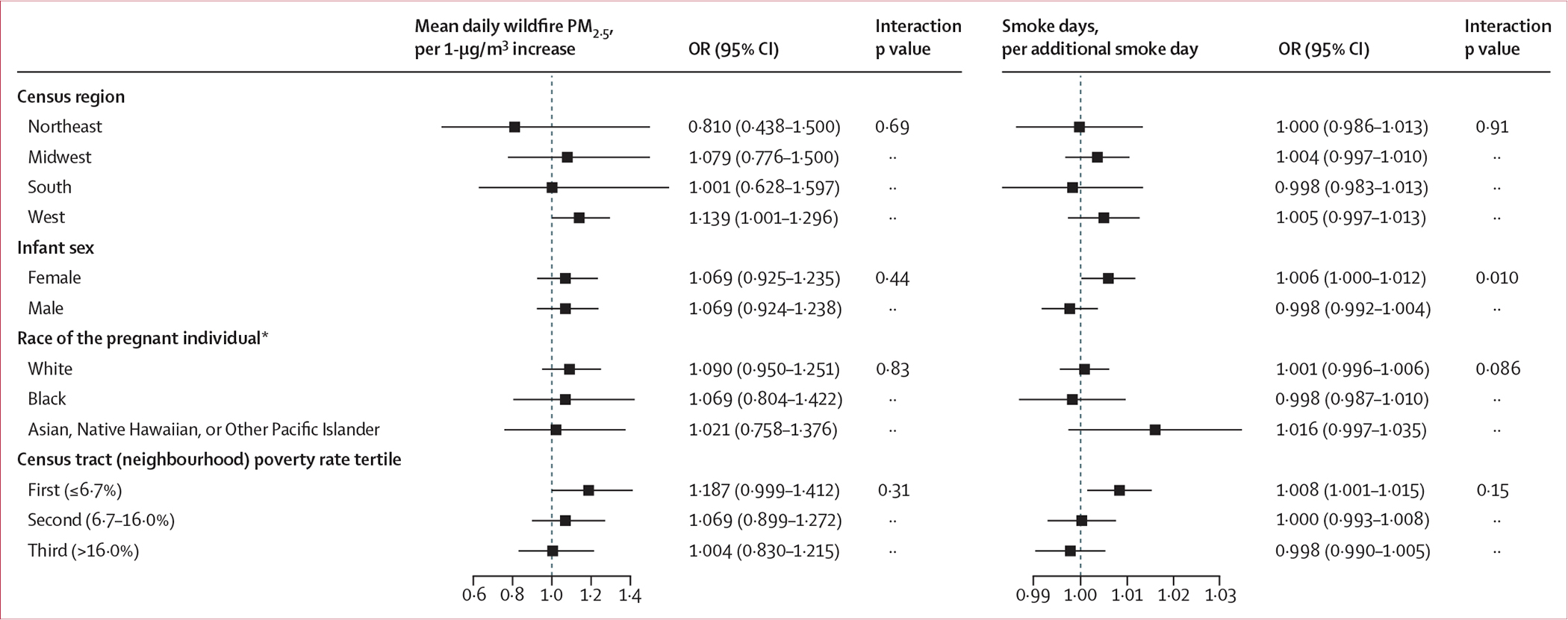 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAir Quality and Health Impacts · Fire effects on ecosystems · Occupational Health and Performance
Introduction
Particulates from wildfire smoke represent a growing contribution to overall ambient PM_2·5_ in the USA.^1^ Research suggests that the toxicity of wildfire PM_2·5_ is elevated relative to that of ambient PM_2·5_ from other sources, due to differences in chemical composition, oxidative potential, and size distribution.^2,3^ Pregnant individuals and the developing fetus might be sensitive to the effects of wildfire-derived PM_2·5_ through pathways including oxidative stress, inflammatory responses, epigenetic programming, and direct effects of particles crossing the placental barrier.^4^ These biological pathways are implicated in the aetiology of adverse birth outcomes including preterm birth, in which delivery occurs before 37 weeks of gestation.^5^ Indeed, preterm birth has been associated with exposure to non-specific ambientPM_2·5_ and, more recently, to wildfire-derived PM_2·5_.^6–13^ About 10% of livebirths in the USA are preterm, which have a greater risk of adverse neonatal outcomes and respiratory and neurodevelopmental effects throughout the lifecourse.^5,14^
Key questions remain regarding the reproductive health effects of wildfire PM_2·5_ and potentially susceptible regions and subgroups. In the USA, previous studies have primarily focused on specific western states or localities.^7,8,12^ Regional differences in smoke composition, climate, housing quality, and opportunity for protective action during wildfire events might lead to differences in exposure or susceptibility to wildfire PM_2·5_.^15^ There are also well documented racial inequities in preterm birth rates in the USA, and there is some evidence for socioeconomic and racial disparities in the health effects of wildfire PM_2·5_.^16,17^ Finally, given the episodic nature of wildfires relative to other ambient sources of PM_2·5_, the role of exposure intensity, duration, and timing during pregnancy remains unclear.
In the present study, we investigated associations between wildfire-specific PM_2·5_ and preterm birth in the prospective nationwide Environmental Influences on Child Health Outcomes (ECHO) Cohort in the USA. We evaluated the role of wildfire smoke PM_2·5_ exposure intensity, duration, and timing during pregnancy, as well as potential effect modification by infant sex, race of the pregnant individual, geographical region, and neighbourhood poverty rate.
Methods
Study design and population
The ECHO Cohort is a longitudinal prospective study involving cohort study sites across the USA. 69 pregnancy and paediatric cohort study sites contributed harmonised data elements in the first cycle of ECHO (2016–23).^18^ In the present analysis, we included live singleton births recorded in the ECHO Cohort with the following criteria: (1) data on gestational age at birth and birthweight, (2) consent for future sharing of data including residential history, (3) at least one acceptable geocoded residence during pregnancy (that could be matched to point address, street address, or street name), (4) entire pregnancy residential history within the contiguous USA, and (5) date of conception between Jan 1, 2006, and March 20, 2020. Wildfire smoke PM_2·5_ exposure estimates were available up to Dec 31, 2020; we restricted the sample to births conceived at least 41 weeks before this date to ensure that preterm births were not preferentially included at the end of the study period and thus avoid fixed cohort bias. We excluded ECHO study sites with (1) selection on low gestational age or birthweight, (2) greater than 25% missingness of model 1 covariates described herein, or (3) fewer than 100 births meeting inclusion criteria. In secondary analyses, we restricted the sample to births in the 11 states of the contiguous US West census region (Arizona, California, Colorado, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming; as defined by the US Census Bureau) due to higher wildfire smoke exposure in this region than in the other census regions, and to enable comparison with previous studies. Gestational age was determined by the following methods: best obstetrical consensus estimate; neonatal estimate of gestational age at delivery; obstetrical estimate from last menstrual period, first or second trimester ultrasound, or in-vitro fertilisation; administratively recorded estimated date of delivery; or caregiver or self-report (appendix p 3). Given that the unit of analysis in our study was individual births, this meant that individuals with multiple singleton births recorded in the ECHO Cohort during the study period could contribute data to the present analysis for more than one birth.
Study protocols for each cohort study site were reviewed by local institutional review boards and/or the designated single ECHO Program institutional review board; all participants provided written consent for the use of data for future ECHO Program research.
Exposure assessment
We used data from a machine learning model of daily wildfire-specific PM_2·5_ across the contiguous USA for the years 2006–20 that has been described previously.^19^ Briefly, satellite imagery and simulated air trajectories from fires were used to identify days with wildfire-related smoke and infer daily mean wildfire PM_2·5_ concentrations at ground-based US Environmental Protection Agency (EPA) monitors. A machine learning model was then developed to predict wildfire PM_2·5_ concentrations using spatiotemporal inputs at a 10 km grid resolution and produce population-weighted census tract means. This model performed well on out-of-sample data from both EPA monitors and PurpleAir monitors (coefficient of determination, R^2^: 0·67–0·70) over the entire range of wildfire PM_2·5_ exposure, improving on previous models that tended to underestimate high wildfire PM_2·5_ concentrations.^19^
We retrospectively linked wildfire PM_2·5_ estimates to pregnant individuals by date and census tract of residence (ie, census tract on each day of pregnancy) to estimate daily wildfire PM_2·5_ exposure during pregnancy. Our metrics of overall wildfire smoke PM_2·5_ exposure were (1) the mean concentration of daily wildfire PM_2·5_ during the exposure period and (2) the number of smoke days, defined as days with exposure to wildfire PM_2·5_ greater than 0 μg/m^3^ (based on modelled estimates of daily mean values^19^) during the exposure period. To evaluate the role of exposure intensity, we calculated the number of smoke days when wildfire PM_2·5_ exceeded prespecified thresholds (≥2·5, ≥5·0, and ≥10·0 μg/m^3^) during the exposure period. These thresholds were selected a priori based on the distribution of wildfire PM_2·5_ concentrations on smoke days, corresponding to approximately the 50th, 75th, and 90th percentiles (appendix p 3). To evaluate the role of exposure duration, we calculated the number of smoke waves, defined as consecutive smoke days (2, 3, or ≥4 days) exceeding the specified thresholds.
Statistical analysis
In descriptive statistics, we calculated mean daily wildfire PM_2·5_ concentrations and the number of smoke days and smoke waves from conception to delivery. We evaluated mean daily wildfire PM_2·5_, mean smoke days, and rates of preterm birth in the overall population and in different categories of demographic characteristics as potential effect modifiers. We also evaluated Pearson’s correlation coefficients between each metric of exposure, and between smoke days in different weeks of gestation.
We investigated preterm birth (delivery before 37 weeks of gestation) as the primary outcome and continuous gestational age at delivery as the secondary outcome. We used pooled logistic regression, a method applicable to interval-censored time-to-event data, to estimate conditional odds ratios (ORs) for preterm birth associated with wildfire smoke PM_2·5_ exposure.^20^ The analytical dataset included time-updated metrics of exposure by gestational week: the cumulative mean daily wildfire PM_2·5_ and the cumulative number of smoke days, defined from conception to the start of each gestational week. Given that preterm births in the study population occurred from 22–36 weeks’ gestation, we calculated these time-updated metrics from gestational week 22 through to delivery for each birth; term births (≥37 weeks’ gestation) were censored at 36 weeks. Models evaluated the outcome of preterm birth status at each gestational week, incorporating an indicator fixed effect for gestational week, ensuring that cumulative pregnancy exposure for a preterm birth was compared to cumulative exposure up to the same gestational week for births at risk for preterm birth. The estimates for all gestational weeks were pooled to yield the odds of preterm birth associated with a one-unit increase in cumulative exposure, conditional on the pregnancy continuing to the start of the previous gestational week.
All models were implemented as mixed-effect models with use of the lme4 package in R (version 4.4.0) with random intercepts for cohort study site. Associations were interpreted based on 95% CIs for effect estimates and whether these crossed the null. Site-specific multiple imputation by chained equations was used to impute missing covariate data using the mice and miceadds packages in R. Potential confounders and precision variables were identified a priori based on a hypothesised directed acyclic graph (appendix p 15).
We specified two models: model 1 (primary model) included infant sex, the pregnant individual’s age at delivery (spline with 3 degrees of freedom), self-reported race (American Indian or Alaska Native; Asian, Native Hawaiian, or Other Pacific Islander; Black; White; more than one race; or Other), self-reported Hispanic ethnicity, and residential census tract poverty rate (continuous; as a neighbourhood-level measure, defined as the percentage of all residents below the annual US federal poverty level by census tract for the census year most proximal to the year of birth), season of conception, infant birth year (spline with 4 degrees of freedom), and spatial thin plate regression splines (10 degrees of freedom) to control for geographical confounding. Model 2 (extended model) included additional adjustment for precision variables and those variables with higher missingness: parity (0, 1, or ≥2), prepregnancy BMI, any self-reported tobacco use during pregnancy, any self-reported alcohol consumption during pregnancy, method of determining gestational age, and education (high school degree or equivalent or less; some college [university] education, associate’s degree, or trade school; bachelor’s degree; or postgraduate degree). Education of the pregnant individual was measured at different stages of their child’s life at different sites (pregnancy: 73%, early childhood [ages 1 to <5 years]: 8%, middle childhood [ages 5 to <12 years]: 19%); we therefore included an interaction term between the reported education level and the life stage at which data were collected. Extended models excluded sites with greater than 50% missingness in any covariate. As a sensitivity analysis, we also fit models with the model 1 adjustments in this restricted sample that excluded sites with greater than 50% missingness. We evaluated associations for preterm birth separately in the nationwide sample and the US West census region.
To investigate the role of exposure timing, we implemented separate logistic regression models with adjustment for model 1 covariates to evaluate associations between smoke days in gestational weeks 0–35 and preterm birth in the nationwide sample.
We used mixed-effects linear regression with adjustment for model 1 covariates for the secondary outcome of gestational age at delivery in the nationwide sample, in which exposure was calculated from conception up to 32 weeks’ gestation to ensure a fixed exposure window and to include 99% of births; births occurring before 32 weeks’ gestational age at delivery (ie, extremely or very preterm; n=210) were excluded from these analyses.
For the exposure metrics of cumulative mean daily wildfire PM_2·5_ and smoke days, we explored effect modification of the primary outcome in the nationwide sample in stratified analyses and with interaction terms evaluated to a significance level of 0·05, adjusted for model 1 covariates. The analysed effect modifiers were infant sex, the four US census regions (West, Midwest, Northeast, and South), race of the pregnant individual, and census tract poverty rate tertiles. Self-reported race was included as a proxy for downstream effects of systemic and multilevel racism including disparities in exposures, outcomes, and opportunities for self-protective action during wildfire events.^15,17^
We also conducted the following sensitivity analyses of the primary outcome at the nationwide level: (1) evaluation of trimester-specific wildfire PM_2·5_ exposure instead of weekly exposure; (2) adjustment for pregnancy-average daily mean ambient temperature and daily mean ambient PM_2·5_;^21,22^ (3) use of fixed effects (instead of random intercepts) for cohort study site and adjustment for the nine US census divisions (New England, Middle Atlantic, East North Central, West North Central, South Atlantic, East South Central, West South Central, Mountain, and Pacific) to control for spatial confounding; (4) use of random intercepts and random effects for cohort study site in mixed models; and (5) complete case analysis instead of multiple imputation of missing covariate data.
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
There were 37 371 births from 49 ECHO sites in the study period, of which 22 656 from 47 sites were singleton births with exposure and outcome data (appendix p 16). We excluded those from sites recruiting for low gestational age or birthweight (n=1490), with fewer than 100 eligible births (n=441), or with greater than 25% missingness of primary covariates (n=691), which gave a final primary study sample of 20 034 singleton births from 30 sites (appendix p 4). In this final sample, the first recorded residences during pregnancy were across all 48 contiguous US states and the District of Columbia, and thus represented all US census regions (West, n=5807 [29·0%]; Midwest, n=3570 [17·8%]; Northeast, n=6379 [31·8%]; and South, n=4278 [21·4%]; figure 1). The extended models excluded an additional 3807 births, resulting in a restricted sample of 16 227 singleton births from 18 sites. Similar to the primary sample, the first recorded residences during pregnancy in the restricted sample represented all US Census regions (47 contiguous states and the District of Columbia; appendix pp 5, 16). In the primary sample, pregnant individuals’ mean age at delivery was 30·6 years (SD 5·6; table 1). Among the 20 034 births, 12 482 (62·3%) of the pregnant individuals identified as White, 2553 (12·7%) as Black, 1342 (6·7%) as Asian, Native Hawaiian, or Other Pacific Islander, 400 (2·0%) as American Indian or Alaska Native, and 1876 (9·4%) as more than one race or Other race; 1381 (6·9%) were missing data on race. 4417 (22·0%) of the individuals identified as Hispanic.
In the primary sample, 1687 (8·4%) of the 20 034 infants were preterm, including 210 (1·0%) extremely or very preterm infants (<32 weeks’ gestation), 189 (0·9%) moderately preterm infants (32–33 weeks’ gestation), and 1288 (6·4%) late preterm infants (34–36 weeks’ gestation). The prevalence of preterm birth was higher among pregnant individuals identifying as Black (299 [11·7%] of 2553) or American Indian or Alaska Native (54 [13·5%] of 400) than among those identifying as White (953 [7·6%] of 12 482) or Asian, Native Hawaiian, or Other Pacific Islander (107 [8·0%] of 1342; table 2). Preterm infants were also slightly more likely to be in the highest tertile of neighbourhood poverty (table 2).
In most of the sample (19 872 [99·2%] of 20 034), pregnant individuals were exposed to at least one smoke day with wildfire PM_2·5_ concentration greater than 0 μg/m^3^ between conception and delivery. The mean daily wildfire PM_2·5_ concentration during pregnancy was 0·36 μg/m^3^ (SD 0·46; table 2). Pregnant individuals were exposed to a mean of 22·2 smoke days (SD 16·6) of any wildfire PM_2·5_ concentration (>0 μg/m^3^), and 1·8 smoke days (3·1) with a wildfire PM_2·5_ concentration of 10·0 μg/m^3^ or greater during pregnancy (table 2). 16 140 (80·6%) individuals were exposed to at least one smoke wave of 2 consecutive smoke days with wildfire PM_2·5_ concentration of 2·5 μg/m^3^ or greater, whereas only 1210 (6·0%) were exposed to at least one 4-day duration smoke wave of higher intensity (≥10·0 μg/m^3^; table 3). The highest mean number of smoke days during pregnancy occurred in the US Midwest region (figure 1, table 2), but the highest mean concentration of wildfire PM_2·5_ on smoke days and the highest mean number of smoke days with wildfire PM_2·5_ concentration of 10·0 μg/m^3^ or greater occurred in the US West region (appendix p 3, table 2). Mean daily wildfire PM_2·5_ exposure was higher among individuals identifying as Asian, Native Hawaiian, or Other Pacific Islander, or American Indian or Alaska Native, than among those identifying as White or Black (table 2). Wildfire PM_2·5_ exposure metrics across pregnancy were weakly to highly correlated (Pearson’s r: 0·31–0·92; appendix p 17). When assessing exposure to smoke days by week of gestation, exposures within a 1–3 week-period were moderately correlated (r: 0·41 to 0·62), while less proximal exposures were negligibly or weakly correlated (r: −0·13 to 0·39; appendix p 18).
In pooled logistic regression analyses with primary model adjustment (model 1), we observed a non-significant association between cumulative mean daily wildfire PM_2·5_ concentrations in pregnancy and preterm birth, with a conditional OR of 1·069 per 1-μg/m^3^ increase (95% CI 0·964–1·187; figure 2, appendix p 6). The association between cumulative smoke days (wildfire PM_2·5_ >0 μg/m^3^) during pregnancy and preterm birth was also in the positive direction (OR 1·002 per additional smoke day [0·998–1·006]), and point estimates increased with increasing intensity of smoke days (ie, wildfire PM_2·5_ ≥2·5, ≥5·0, and ≥10·0 μg/m^3^), although the 95% CIs included the null. Associations between exposure to cumulative smoke waves and preterm birth were generally in the positive direction but not statistically significant.
In analyses restricted to the US West region (N=5807), associations between cumulative wildfire PM_2·5_ exposure metrics during pregnancy and preterm birth had larger point estimates, some of which were statistically significant, than in the nationwide analyses (figure 2, appendix p 6). There were increased odds of preterm birth associated with mean daily wildfire PM_2·5_ (OR 1·139 per 1-μg/m^3^ increase [95% CI 1·001–1·296]), exposure to smoke days with a wildfire PM_2·5_ concentration of 5·0 μg/m^3^ or greater (OR 1·018 per additional smoke day [1·003–1·032]) and 10·0 μg/m^3^ or greater (OR 1·030 [1·006–1·054]), and exposure to ≥4-day smoke waves of 5·0 μg/m^3^ or greater (OR 1·185 per additional smoke wave [1·044–1·347]) and 10·0 μg/m^3^ or greater (OR 1·232 [1·029–1·475]).
In both the nationwide and US West analyses, estimates were generally similar with extended covariate adjustment (model 2) in the restricted sample of births from sites with available covariate data (nationwide sample, N=16 227; US West sample, N=5226), when compared with model 1 estimates in the full samples (appendix p 6). However, in the US West samples, significant associations were observed for 3-day smoke waves with a wildfire PM_2·5_ concentration of 5·0 μg/m^3^ or greater and of 10·0 μg/m^3^ or greater in model 2 but not in model 1. When comparing the results of model 1 and 2 in the restricted samples, model 2 point estimates were uniformly higher but with overlapping confidence intervals compared with estimates from model 1 in both the nationwide sample and US West sample (appendix p 6). In the nationwide sample, sensitivity analyses exploring alternative assumptions yielded consistent conclusions with those from model 1 in the main analysis (appendix p 19).
For the secondary outcome, associations between exposure to wildfire PM_2·5_ from conception to 32 weeks’ gestation and gestational age at delivery were generally in the negative direction but small in magnitude, with 95% CIs spanning the null (appendix p 7).
Evaluation of the association between smoke days by week of gestation and preterm birth identified associations in mid-pregnancy for smoke days with wildfire PM_2·5_ concentrations above 0 μg/m^3^, of 2·5 μg/m^3^ or greater, and of 5·0 μg/m^3^ or greater, with the largest effect estimates in gestational week 21 (figure 3). By contrast, smoke days with wildfire PM_2·5_ concentration of 10·0 μg/m^3^ or greater showed associations with preterm birth in late pregnancy, peaking in gestational week 31. Sensitivity analysis of trimester-specific exposures in terms of mean daily wildfire PM_2·5_, smoke days, and smoke waves consistently showed positive point estimates of association for second-trimester exposures, albeit with most 95% CIs spanning the null. There were also elevated but imprecise associations for third-trimester high-intensity exposure (appendix p 20).
In effect modification analyses, point estimates of associations between cumulative wildfire PM_2·5_ exposure metrics and preterm birth were larger in the US West and Midwest regions compared with the other regions, although differences were not statistically significant (figure 4). There was a stronger association between wildfire smoke days (PM_2·5_ >0 μg/m^3^) and preterm birth among female infants relative to male infants (female infants OR 1·006 [95% CI 1·000–1·012] vs male infants OR 0·998 [0·992–1·004]; interaction p=0·010). There was no evidence of effect modification by race of the pregnant individual. Point estimates of association for both mean daily wildfire PM_2·5_ and smoke days were highest for births among pregnant individuals with the lowest residential poverty rates, but with interaction p values greater than 0·1.
Discussion
We evaluated associations between exposure to wildfire-specific PM_2·5_ and preterm birth in a large, geographically diverse, well characterised prospective US cohort. In nationwide analyses, associations between cumulative pregnancy exposure to wildfire smoke PM_2·5_ and preterm birth were consistently in the hypothesised direction but imprecise and included the null. Associations were observed in mid-pregnancy for low-intensity and moderate-intensity smoke days, and in late pregnancy for high-intensity smoke days. In the US West sample, we observed increased odds of preterm birth with exposure to moderate-to-high-intensity smoke days, and with longer-duration moderate-to-high-intensity smoke waves. In all analyses, point estimates of association with preterm birth were generally larger for smoke days and smoke waves of increased intensity and duration (ie, exposure–response), and were larger with more comprehensive model adjustment in the sample of births with available covariate data. We did not identify consistent effect modification based on sex of the infant or race of the pregnant individual, although the association between smoke days and preterm birth was stronger among female infants than among male infants.
Previous studies of wildfire smoke and preterm birth have also generally identified adverse effects.^4,23^ In the USA, a 1 μg/m^3^ increase in mean daily wildfire PM_2·5_ during pregnancy was associated with increased odds of preterm birth among 534 798 births in Colorado^8^ (OR 1·055 [95% CI 1·033–1 078]) and among 5 155 026 births in California^12^ (OR 1·013 [1·008–1·017]). A study in eight southwestern US states reported elevated but null estimates of association between pregnancy mean wildfire PM_2·5_ and preterm birth.^11^ In New South Wales, Australia, an IQR increase in pregnancy mean wildfire PM_2·5_ (0·85 μg/m^3^) was associated with a hazard ratio of 1·069 (95% CI 1·058–1·081) for preterm birth among 330 884 births.^6^ These findings are similar in magnitude but more precise relative to our estimated OR of 1·069 (95% CI 0·938–1·165) for a 1-μg/m^3^ increase in mean daily wildfire PM_2·5_ with primary adjustment, and 1·080 (0·968–1·204) with extended adjustment. Heft-Neal and colleagues^7^ observed a 0·498% (95% CI 0·407–0·588) increase in the risk of preterm birth with each additional day within a wildfire smoke plume during pregnancy in California among 3 063 672 births. In the present analysis, we detected associations with smoke days only for moderate-to-high-intensity smoke days (ie, wildfire PM_2·5_ ≥5 μg/m^3^ and ≥10 μg/m^3^) in the US West. Other studies have used exposure metrics defined by the occurrence of nearby wildfires or megafires and identified associations with preterm birth.^9,10^ Differences in findings between previous studies and the present study likely stem from variable exposure assessment methods, study design, adjustment for confounding, geographical regions of focus, and outcome assessment.^4,23^
We identified larger point estimates of association between wildfire PM_2·5_ exposure and preterm birth in the US West relative to the nationwide study sample. A number of factors could contribute to this finding. First, regional differences in fuel sources and fire severity affect the composition and toxicity of wildfire-derived PM_2·5_.^24^ Second, the US West is exposed to wildfire smoke that is more recent in origin relative to other regions,^25^ and fresh wildfire smoke might have different toxicity relative to aged smoke due to physicochemical changes during long-range transport.^3^ Third, regional differences in housing characteristics, use of air conditioning, and weather conditions (including co-occurrence of wildfire smoke and heat) could potentially modify the association between wildfire PM_2·5_ and health outcomes.^16,26^ Finally, the mean concentration of wildfire PM_2·5_ on smoke days was highest in the US West, and the predictive accuracy of the exposure model was highest in the Pacific Northwest and central and northern California.^19^ Thus, effect estimates might be biased towards the null in other regions due to lower exposure heterogeneity and higher exposure measurement error.
Our findings suggest that critical windows of exposure might depend on the intensity of wildfire PM_2·5_. Models assessing smoke days by week of gestation identified associations with preterm birth in mid-pregnancy for low-to-moderate-intensity smoke days, and in late pregnancy for high-intensity smoke days. Six previous studies estimated the strongest increased risk of preterm birth with second-trimester exposure to wildfire PM_2·5_ or smoke days, with some significant associations also observed for third-trimester exposure.^6–9,11,12^ Although not the focus of the present analysis, Ha and colleagues^16^ explored wildfire smoke as a potential trigger of delivery, identifying an increased risk of delivery on days with wildfire smoke. Previous studies of ambient PM_2·5_ have also identified mid-pregnancy and near-delivery as potential windows of fetal vulnerability.^27,28^ The second trimester of pregnancy is the period of largest placental growth and angiogenesis and has been identified as a period of heightened vulnerability to the biological effects of PM_2·5_.^29^
We did not find consistent trends in effect modification across exposures and outcomes. Among female infants, the associations between wildfire smoke days of any concentration of wildfire PM_2·5_ (>0 μg/m^3^)—but not mean daily wildfire PM_2·5_—and preterm birth were stronger than among male infants. Requia and colleagues^10^ also reported stronger associations between wildfire smoke and preterm birth among female infants, while Zhang and colleagues^6^ found stronger associations between wildfire PM_2·5_ and preterm birth for male infants. We did not observe significant differences in associations between wildfire PM_2·5_ exposure metrics and preterm birth by neighbourhood poverty rate tertile or race of the pregnant individual, a finding that aligns with other studies.^7,11^
This study has limitations. First, the spatiotemporal model of wildfire PM_2·5_ has spatially heterogeneous performance, relies on US EPA monitors which are more concentrated in populated areas, and does not distinguish between wildfires, prescribed burns, and agricultural burning. However, the model incorporates spatiotemporal data inputs that have comprehensive coverage, performs well on out-of-sample data, has been validated against other recent wildfire PM_2·5_ models in California, and has been previously used in epidemiological applications.^19,30,31^ Second, we evaluated several exposure–response relationships to a significance level of 0·05, increasing the probability of incorrectly rejecting the null hypothesis. To mitigate this potential issue, we focused on the trends with respect to wildfire smoke intensity and duration when interpreting findings. Third, although the large geographical scope is a strength of our study, generally low wildfire smoke exposure in the Northeast and South census regions likely contributed to low statistical power to detect associations. We also evaluated pregnancy-average temperature as a potential confounder, but we did not explore potential interactions between temperature and wildfire PM_2·5_ exposure. Both extreme heat and extreme cold have been associated with adverse birth outcomes including preterm birth, and extreme heat might co-occur with wildfire-related PM_2·5_ exposure and have combined health effects.^16,26^ Future studies could more comprehensively explore the perinatal health effects of heatwaves in combination with wildfire PM_2·5_.
Our study has a number of notable strengths. To our knowledge, it is among the first studies to incorporate the use of smoke waves to evaluate the effect of wildfire PM_2·5_ exposure intensity and duration on adverse birth outcomes, as well as the first to use data from a longitudinal cohort rather than administrative records. We included a geographically, socioeconomically, and demographically diverse study population across the contiguous USA, building on previous literature at the state and regional level. We also had access to data on sociodemographic variables and health during pregnancy that are not typically reliable in birth records, including tobacco use and alcohol consumption during pregnancy, and prepregnancy BMI. In the sample of births with available covariate data, adjustment for these additional variables strengthened effect estimates for preterm birth. Another strength of the ECHO data is the availability of longitudinal residential history during pregnancy, rather than reliance on residence at time of delivery.
Our analysis found that the odds of preterm birth were increased with exposure to moderate-to-high-intensity smoke days and longer-duration moderate-to-high-intensity smoke waves in the US West region. Climate change and associated changes in temperature and vegetation aridity are projected to contribute to increases in the frequency, size, duration, and destructivity of wildfire activity,^32,33^ indicating the potential for more widespread population exposure to higher intensity and longer-duration wildfire episodes. Our research suggests that public health interventions to reduce exposure to wildfire smoke events could help to prevent adverse birth outcomes related to wildfire smoke exposure.
Supplementary Material
1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burke M, Driscoll A, Heft-Neal S, Xue J, Burney J, Wara M. The changing risk and burden of wildfire in the United States. Proc Natl Acad Sci U S A 2021; 118: e 2011048118.33431571 10.1073/pnas.2011048118 PMC 7812759 · doi ↗ · pubmed ↗
- 2Wegesser TC, Pinkerton KE, Last JA. California wildfires of 2008: coarse and fine particulate matter toxicity. Environ Health Perspect 2009; 117: 893–97.19590679 10.1289/ehp.0800166 PMC 2702402 · doi ↗ · pubmed ↗
- 3Kim YH, Sinha A, George IJ, De Marini DM, Grieshop AP, Gilmour MI. Toxicity of fresh and aged anthropogenic smoke particles emitted from different burning conditions. Sci Total Environ 2023; 892: 164778.37302606 10.1016/j.scitotenv.2023.164778 PMC 12131020 · doi ↗ · pubmed ↗
- 4Padula AM, Raynes-Greenow C. Health effects of wildfire smoke during pregnancy and childhood. In: Loboda TV, French NHF, Puett RC, eds. Landscape fire, smoke, and health. American Geophysical Union, 2024: 249–63.
- 5Frey HA, Klebanoff MA. The epidemiology, etiology, and costs of preterm birth. Semin Fetal Neonatal Med 2016; 21: 68–73.26794420 10.1016/j.siny.2015.12.011 · doi ↗ · pubmed ↗
- 6Zhang Y, Ye T, Yu P, Preterm birth and term low birth weight associated with wildfire-specific PM 2·5: a cohort study in New South Wales, Australia during 2016–2019. Environ Int 2023; 174: 107879.36958111 10.1016/j.envint.2023.107879 · doi ↗ · pubmed ↗
- 7Heft-Neal S, Driscoll A, Yang W, Shaw G, Burke M. Associations between wildfire smoke exposure during pregnancy and risk of preterm birth in California. Environ Res 2022; 203: 111872.34403668 10.1016/j.envres.2021.111872 · doi ↗ · pubmed ↗
- 8Abdo M, Ward I, O’Dell K, Impact of wildfire smoke on adverse pregnancy outcomes in Colorado, 2007–2015. Int J Environ Res Public Health 2019; 16: 3720.31581673 10.3390/ijerph 16193720 PMC 6801422 · doi ↗ · pubmed ↗