Out-of-hours services in Zealand, Denmark. Consequences of changeover from GP-cooperative to integrated deputized services. A retrospective cohort study
Stig Nikolaj Fasmer Blomberg, Hauraz Haji, Ole Mazur Hendriksen, Mai-Britt Hägi-Pedersen, Helle Collatz Christensen

TL;DR
This study examines how changing the structure of out-of-hours medical services in Zealand, Denmark, affected patient care and hospital admissions.
Contribution
The study provides new insights into the impact of reorganizing out-of-hours services on patient pathways and emergency admissions.
Findings
Patient pathways in out-of-hours services decreased after transitioning to a regional service model.
Emergency department admissions per 100,000 inhabitants dropped following the organizational change.
The proportion of emergency admissions increased despite fewer overall patient cases.
Abstract
Out-of-hours services (OOHS) worldwide exhibit diverse organisational models, especially within the European Union. This study aims to describe the transformation of OOHS in Region Zealand, Denmark, from a General Practitioner cooperative (GP-OOHS) to a regional organization/service, known as the 1818 Medical Helpline (1818). Retrospective cohort study. GP-OOHS data (January 2017–October 2023) during the transition from GP-cooperative to Regional Service (October 2022) were analysed. Coded and timestamped services retrieved from the billing system were used to identify patient pathways, defined as services within a 12-hour window. Descriptive statistics were applied. A total of 2,572,951 patient pathways were recorded, with 2,258,072 under GP-out-of-hours service and 314,879 under the 1818. Overall, patient pathway volumes declined from 412,116 in 2017 to 314,879 in 2022, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
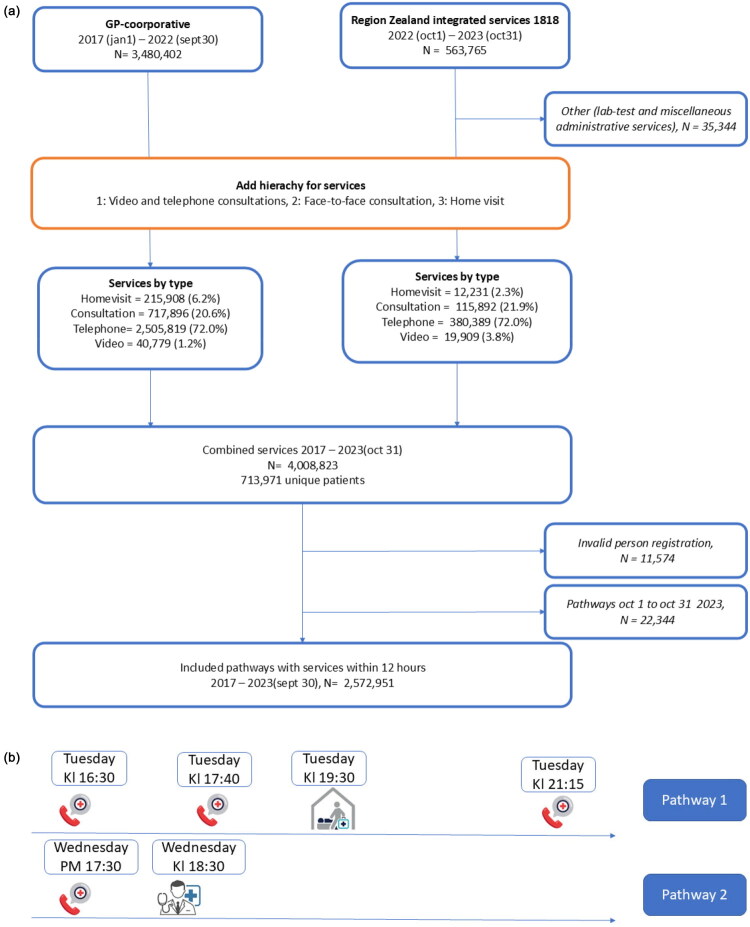 Figure 1
Figure 1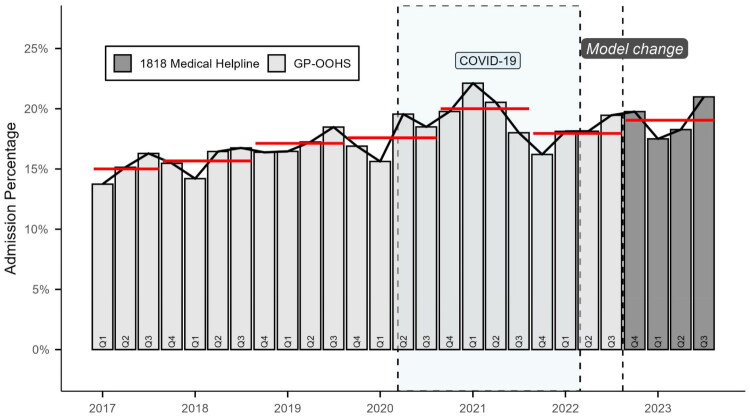 Figure 2
Figure 2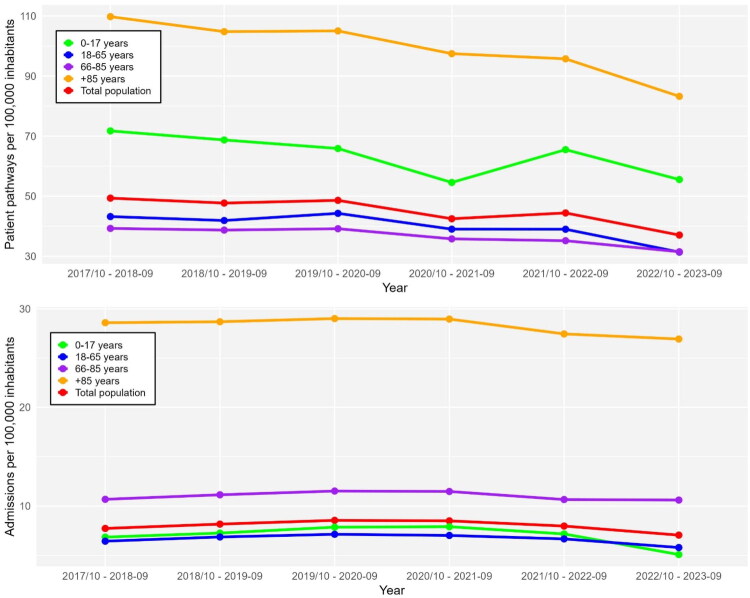 Figure 3
Figure 3| Domain | Previous model (GP cooperative, Region Zealand, before October 2022) | Current model (1818 OOHPC, Region Zealand, from October 2022) |
|---|---|---|
| Organizational structure | Regional GP cooperative organized as part of general practice out-of-hours system | Single regional out-of-hours primary care (OOHPC) service operated directly by Region Zealand |
| Service name | GP-OOHS | 1818 Medical Helpline (named after the hotline number) |
| Contact telephone number | 70 15 07 00 | 1818 |
| Access to care | Patients contacted GP-OOHS directly by telephone | Patients contact regional 1818 directly by telephone |
| Service hours | Weekdays 4 PM–8 AM; weekends and public holidays 24/7 | Weekdays 4 PM–8 AM; weekends and public holidays 24/7 |
| Triage personnel | Telephone triage performed exclusively by GPs | Telephone triage performed by physicians from any medical specialty and nurses |
| Use of decision support | Based on GP clinical expertise and judgment; no formal decision support tools | No decision support tools; nurses follow predefined clinical instructions under delegated medical responsibility |
| Remote consultations | Telephone consultations provided by GPs; no systematic use of video | Telephone and video consultations provided by physicians and nurses |
| In-clinic consultations | All consultations conducted by GPs | Consultations conducted by physicians with nurse assistance; nurses may complete consultations after physician assessment |
| Home visits (16:00–22:00) | Home visits performed by GPs | Physicians perform home visits accompanied by paramedics |
| Home visits (22:00–08:00) | Home visits performed by GPs | Paramedics perform home visits with telephone supervision by EMCC* physician |
| Physical locations | Several fixed consultation sites, mostly located on hospital premises | Physical clinic locations unchanged |
| Diagnostics available | Limited point-of-care testing in clinics; minimal diagnostics during home visits | Not specified; likely limited diagnostics |
| Remuneration model | Fee-for-service payment to GPs | Fixed hourly wages for all staff |
| Medical record accessibility | Records not integrated with hospital records; separate GP-OOHS system (Medwin) | OOHPC records accessible to hospital staff |
| GP-OOHS, | 1818, | TOTAL, | |
|---|---|---|---|
| Age, Median (Q1;Q3) | 35 (15;59) | 35 (14;62) | 35 (15;60) |
| Male %, (n) | 44.5 (1,004,821) | 44.3 (139,370) | 44.5 (1,144,191) |
| Patient pathways per month (average) | 32,726 | 26,240 | 31,765 |
| Proportion ended in phone, % | 57.9 | 64.7 | 58.7 |
| Proportion ended in face-to-face consultation % | 31.4 | 27.0 | 30.9 |
| Proportion ended in homevisit, (%) | 9.4 | 3.3 | 8.6 |
| Proportion ended in videoconsult, (%) | 1.4 | 5.0 | 1.8 |
| Age 0–17, % (n) | 27.8 (627,753) | 28.7 (90,373) | 27.9 (718,126) |
| Age 18–65, % (n) | 52.3 (1,182,606) | 49.6 (156,155) | 52.0 (1,338,761) |
| Age 66–85, % (n) | 15.8 (355,990) | 17.3 (54,421) | 16.0 (410,411) |
| Age +85, % (n) | 4.1 (91,723) | 4.4 (13,930) | 4.1 (105,653) |
| Average number of individuals/month | 28.005 | 23.248 | 27.224 |
| Average number of patient pathways/month | 32.726 | 26.240 | 31.765 |
| Weekday, % (n) | 47.4 (1,069,856) | 47.8 (150,370) | 47.4 (1,220,226) |
| Call 08–15, % (n) (weekends/ holidays only) | 30.3 (683,816) | 31.,0 (97,528) | 30.4 (781,344) |
| Call 16–22, % (n) | 54.6 (1,232,119) | 52.2 (164,380) | 54.3 (1,396,499) |
| Call 23-07, % (n) | 15.2 (342,137) | 16.8 (52,971) | 15.4 (395,108) |
| 2017/10–2018–09 | 2018/10 − 2019-09 | 2019/10 − 2020-09 | 2020/10 − 2021-09 | 2021/10 − 2022-09 | 2022/10 − 2023-09 | |
|---|---|---|---|---|---|---|
| Patient pathways, all ages, (n) | 412,116 | 399,212 | 407,052 | 356,419 | 374,686 | 314,879 |
| Incidence per 100,000 inhabitants | 49,354 | 47,711 | 48,611 | 42,490 | 44,420 | 37,051 |
| Admitted within 24 h (n) | 64,555 | 68,364 | 71,594 | 71,293 | 67,253 | 59,967 |
| Proportion admitted (%) | 15.7% | 17.1% | 17.6% | 20.0% | 17.9% | 19.0% |
| Patient pathways, age 0–17, (n) | 119,556 | 113,357 | 107,733 | 88,818 | 106,591 | 90,373 |
| Incidence per 100,000 inhabitants | 71,749 | 68,731 | 65,888 | 54,572 | 65,504 | 55,539 |
| Admitted within 24 h (n) | 11,418 | 11,974 | 12,853 | 12,869 | 11,674 | 8,277 |
| Proportion admitted, (%) | 9.6% | 10.6% | 11.9% | 14.5% | 11.0% | 9.2% |
| Patient pathways, age 18–65, (n) | 213,526 | 207,059 | 218,255 | 192,067 | 192,634 | 156,155 |
| Incidence per 100,000 inhabitants | 43,210 | 41,900 | 44,283 | 39,023 | 38,989 | 31,382 |
| Admitted within 24 h (n) | 31,829 | 33,938 | 35,19 | 34,563 | 32,964 | 28,854 |
| Proportion admitted (%) | 14.9% | 16.4% | 16.1% | 18.0% | 17.1% | 18.5% |
| Patient pathways, age 66–85, (n) | 62,512 | 62,881 | 64,836 | 60,17 | 59,999 | 54,421 |
| Incidence per 100,000 inhabitants | 39,269 | 38,708 | 39,167 | 35,786 | 35,175 | 31,490 |
| Admitted within 24 h (n) | 17,005 | 18,095 | 19,069 | 19,296 | 18,182 | 18,329 |
| Proportion admitted (%) | 27.2% | 28.8% | 29.4% | 32.1% | 30.3% | 33.7% |
| Patient pathways, age +85, (n) | 16,522 | 15,915 | 16,228 | 15,364 | 15,462 | 13,930 |
| Incidence per 100,000 inhabitants | 109,803 | 104,814 | 105,063 | 97,481 | 95,764 | 83,259 |
| Admitted within 24 h (n) | 4,303 | 4,357 | 4,482 | 4,565 | 4,433 | 4,507 |
| Proportion admitted (%) | 26.0% | 27.4% | 27.6% | 29.7% | 28.7% | 32.4% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEmergency and Acute Care Studies · Primary Care and Health Outcomes · Hospital Admissions and Outcomes
Introduction
Out-of-hours services (OOHS) vary in their organizational models worldwide, reflecting national variations in healthcare organization, workforce capacity, and service delivery models [1–3]. Within the European Union, countries typically operate between three and 10 coexisting models, with general practitioner (GP) cooperatives being the most common, followed by primary care centres and rota groups of GPs [4,5]. Recent trends in OOHS include organizational restructuring and service upscaling [6]. These developments reflect a broader shift towards centralization, optimization, professionalization, and expanded diagnostic capabilities. However, these national variations in OOHS organization underscore regional disparities in access and raise concerns about potential care fragmentation.
The Danish healthcare system provides emergency medical services (EMS) and out-of-hours care for medical problems arising outside regular working hours [1,7]. Until October 2022, OOHS in Region Zealand’s were provided by GP cooperatives. These services were staffed by GPs working outside regular office hours. However, increasing difficulty in maintaining on-call coverage, driven by physician shortages and healthcare centralization prompted the region to implement a new integrated service model.
The new system, known as ‘1818’ (after the designated phone number), employs physicians of any specialty directly to triage all calls and compensates them on an hourly basis. To enhance flexibility and efficiency nurses were introduced during peak times. Although physical service locations remained unchanged, the payment model was altered: GPs was employed by the region and paid on hourly basis. Before implementation, emergency departments (ED), already understaffed and overburdened - expressed concern that the reorganisation might increase ED activity, as had been observed in the neighbouring Capital Region after a similar reform in 2014 [15].
The characteristics of the two types of organisations are shown in Table 1.
This retrospective cohort study investigates the impact of the reorganization on ED admissions. We hypothesized that the transition would result in higher ED admission rates as seen in The Capital Region. Secondary outcomes included differences in overall activity between the two service models.
Methods
Setting
Region Zealand is a mixed rural-urban region in Denmark with 850,000 inhabitants, where Out-of-hours medical needs are met by regionally organized services outside standard GP opening hours.
The OOHS operates through telephone triage, where patients’ needs are assessed and results in one of several outcomes: telephone advice, video-consultation, physical consultation, home visit, or ED admission. Patients are free to choose any OOHS facility and may be booked for the consultation that best fits their location and preferences. OOHS is available from 4:00 PM to 8:00 AM on weekdays and all hours on weekends and public holidays [7,8].
Data collection
Administrative and billing data were obtained from both the GP-OOHS and the 1818. The dataset had information on the type of service delivered (code), patients’ ID and time of service delivery. The data structure was uniform during the entire study period, with no changes to the electronic health record system.
All services provided by GP-OOHS or 1818 in the dataset are given a code and a timestamp.e.g. ‘0101 Consultation’, ‘0301 Telephone Consultation’, ‘0471 Home Visit’ etc. For each patient pathway, all codes were stored with a timestamp for the service, and the patient’s personal identifier [9]. Data were collected for the period between January 1, 2017, and October 1, 2023. The transition from independent GP-OOHS to 1818 was effective from October 1, 2022.
Defining Patient Pathways: In this study, we define a patient pathway as a sequence of one or more services delivered within a 12-hour window. Each patient pathway reflects a single episode of acute care and includes all OOHS interactions (calls, consultations, visits) during that time frame. The 12-hour window was chosen as it corresponds to the typical period until general practices reopen the following day. This definition allows us to analyse the number of distinct acute episodes requiring out-of-hours care, rather than the number of individual service interactions. (See Figure 1(b)).
a. Population flowchart, Out-of-hours-services in Region Zealand. b. Patient pathways in Out-of-hours-services in Region Zealand.
The term patient pathway is used throughout the manuscript to denote these grouped episodes of care. While the underlying dataset consists of timestamped service codes (e.g. phone calls, home visits), our analyses focus on patient pathways as the unit of analysis.
This grouping was chosen to reflect the clinical reality of acute illness episodes rather than individual service events. By treating multiple services within a 12-hour window as a single patient pathway, we avoid overcounting patients who may, for example, call several times in the same episode of illness. For the purposes of this study, the key unit of analysis is not the number of service interactions, but the number of distinct patient episodes that triggered OOHS involvement. This is particularly important when assessing downstream outcomes such as ED admission. Using individual services as the denominator would give a misleading picture of the admission rate, as some patients, especially those with more complex or uncertain symptoms, might generate multiple entries for what is in practice a single clinical situation. For each patient pathway, the time of the first and last service were recorded, as well as the service with the highest clinical hierarchy. Telephone and video consultations were ranked lowest, followed by face-to-face consultations, and home visits ranked highest. Thus, in the example described above, the first patient pathway would be categorized as ending in a home visit.
Linking to ED Admissions: Once the dataset of patient pathways was created, we added data on ED admissions. ED admissions were identified by linkage through the unique personal identification number (CPR) to the Danish National Patient Register (LPR) [9,10]. Any admission occurring within 24 h after the last recorded service was categorized as a ED admission using a binary variable.
For trend analyses, we restricted the dataset to the period October 2017–October 2023 to allow for consistent year-over-year comparisons. The first five years (October 2017–October 2022) correspond to the GP-OOHS model, and the final year (October 2022–October 2023) corresponds to the 1818.
Statistics
Descriptive analyses were performed, and absolute numbers and percentages for variables were reported. To assess changes over time and the potential impact of the organisational transition to the 1818 (October 2022), an interrupted time series (ITS) regression analysis was conducted based on aggregated 12-month periods (October–September). The models estimated pre-intervention trends and post-intervention level changes for both pathway counts (Poisson regression) and admission proportions (binomial regression). The data analyses and management were conducted using R (version 3.5.3, R Core Team), and SAS statistical software (version 9.4, SAS Institute).
Results
Between 2017 and October 2023, a total of 2,572,951 patient pathways were recorded (Table 2). The median patient age was 35 years in both organizations, with slight variation in age distribution: in GP-OOHS, the interquartile range was 15–59 years, while in 1818 it was 14–62 years. The GP-OOHS handled a higher average monthly volume of 32,726 patient pathways compared to 26,240 patient pathways per month in 1818.
Seasonal variation was comparable between the two models, although GP-OOHS consistently maintained a higher level of activity (Figure 2).
Temporal volume of consultations resulting in admission. This figure illustrates the temporal trend (percentage of quarterly cases) admitted to emergency department during the study period (2017–2023). The bars in light grey (Q1 2017 to Q3 2022) represent the period with patient management using the GP-OOHS, whereas the dark grey bars (Q4 2022 to Q3 2023) represent the period with patients managed by 1818. The dashed vertical line marks the transition between the models. The horizontal red lines showcase the median admission percentage prior to the transition (GP-OOHS) and one year after (1818).
Face-to-face consultations were more frequent in GP-OOHS (31.4%) than in 1818 (27.0%). Similarly, home visits were more common in GP-OOHS (9.4% vs. 3.3%). Conversely, telephone consultations accounted for a larger share of patient pathways in 1818 (64.7%) compared to GP-OOHS (57.9%). Video consultations were introduced later in GP-OOHS (2021), which explains their lower overall share (1.4% vs. 5.0%).
Approximately half of all patient pathways occurred on weekdays (GP-OOHS: 47.4%, 1818: 47.8%). Most patient pathways took place in the early evening (16:00–22:00), with 54.6% in GP-OOHS and 52.2% in 1818. Weekend daytime patient pathways (08:00–15:00) were largely equivalent between GP-OOHS and 1818 (31.0% vs. 30.3%), while night-time patient pathways (23:00–07:00) were marginally lower in GP-OOHS (15.2% vs. 16.8%). Throughout the study period, the total number of patient pathways decreased from 412,116 in 2017 to 314,879 in 2023. ED admissions following OOHS patient pathways also declined, from 64,555 admissions in 2017 to 59,967 in 2023 equivalent to 15.7% and 19.0% of pathways, respectively. In the interrupted time series analysis using 12-month periods (October–September), the number of pathways showed a continuous annual decline of approximately 3% prior to the organisational transition to the 1818, followed by an additional 12% level decrease after October 2022 (p < 0.001). Although the crude proportion of admitted patients increased over time, the binomial model indicated that the odds of admission decreased by about 6% relative to the pre-intervention trend (p < 0.001), suggesting that the previously increasing tendency in ED admissions flattened following the transition. (Table 3, Figure 3). Among children (0–17 years), the proportion of patient pathways resulting in admission rose steadily in the early years of the study: from 9.6% in 2017 to 10.6% in 2018, 11.9% in 2019, and 14.5% in 2020. After the organizational shift to 1818, admission rates declined to 11.0% in 2022 and reached 9.2% in 2023. This decline coincided with a marked reduction in the number of paediatric patient pathways over time.
Incidence rates of patient pathways and admissions. This figure illustrates the temporal trends in incidence rates of patient pathways to the out-of-hours service (top) and admissions resulting from these patient pathways (bottom), measured per 100,000 inhabitants across age groups from 2017 to 2023. The age groups represented are ‘0–17 years,’ ‘18–65 years,’ ‘66–85 years,’ ‘+85 years,’ and ‘Total.’ The incidence rates are displayed for each year period. The upper plot shows the overall incidence of patient pathways, while the lower plot focuses on the subset that resulted in hospital admissions. Each colored line represents a specific age group, and the ‘Total’ is shown separately for comparison.
In adults aged 18–65 years, the total number of patient pathways decreased from 213,526 in 2017 to 192,634 in 2022 and further to 156,155 in 2023 equivalent to a 27% reduction over the period. Despite this decline in patient pathways, the proportion admitted increased throughout most of the period, reaching 18.5% in 2023. However, the absolute number of admissions in this group fell to 28,854 by 2023, the lowest level observed during the study period.
Among patients aged 66–85 years, a similar decline in patient pathways was observed, particularly after the transition to the 1818. Patient pathways fell from 62,512 in 2017 to 54,421 in 2023, while the proportion admitted increased to 33.7% (18, 329) in 2023 compared to 30.3% (18, 182) in 2022 and 27.2% (17,005) in 2017.
For patients aged 85 years and older, the total number of patient pathways decreased from 15,462 in 2017 to 13,390 in 2023. Simultaneously, the number of admissions increased slightly from 4,433 (28.7%) in 2017 to 4,507 (32.4%) in 2023.
Across all age groups, incidence rates of patient pathways to OOHS declined over the study period, while incidence rates of ED admissions showed a less pronounced decline (Figure 3). Seasonal variations and the impact of the COVID-19 pandemic were also observed. In particular, a reduction in face-to-face consultations occurred during the pandemic period, followed by a return to pre-pandemic levels by 2022 under 1818 (Supplementary Figure 1).
Discussion
In this retrospective cohort study of patients contacting OOHS in Region Zealand from January 2017 to October 2023, we analysed a dataset of 2,572,951 patient pathways. A decline in patient pathways and subsequent ED-admissions was found, and the decline was stable including last year when the organisation transitioned from GP-OOHS to 1818.
Over the study period, the annual number of patient pathways declined from 412,116 to 314,879, and subsequent ED admissions decreased from 64,555 to 59,967. The reduction in patient pathways predominantly affected patient categories that did not result in ED admission. Age-specific patterns showed a decline among the youngest patients, a moderate decrease among middle-aged groups, and relatively stable admission rates among the oldest patients. In the last year of the study period where the 1818 was operated as an integrated service, a larger proportion of the patients were admitted to the ED, though this in absolute numbers was lower than in any of the previous years. For comparison, there were a total of 281,577 ED admissions in Region Zealand in 2023.
The transition from GP-OOHS to 1818 is part of a broader trend, where OOHS mainly operated by GPs is in decline internationally [11]. While several studies have described the influx of patients in OOHS [12] , little is known about the impacts of new systems in treating medical conditions outside office hours. In a European setting, Danish OOHS are known to be amongst the most visited OOHS [13]. In a previous study, Huibers et al. found that Danish OOHS had 481 crude contacts per 1,000 personyears, which was found to be higher than comparative system [14]. We investigated several consecutive years (2017–2023), allowing us to investigate the use of OOHS over time.
The Danish EDs have seen an overall increasing level of activity, and especially The Capital Region of Denmark have shown an increasing incidence rate of contacts, after the organisational change of the OOHS to an integrated organisation [15]. Such an increase could be expected in The Capital Region, where patients are seen at hospital-based facilities, and it has given rise to some debate regarding its potential impact on ED workload. While the concern is very real and was voiced prior to the transition from GP-OOHS to 1818 in October 2022, in this study the actual number of admitted patients decreased in absolute numbers, while the proportion of OOHS patient pathways with a subsequent admission increased. Further, in the interrupted time series analysis, we found that the transition towards an integrated organisation appeared to slow down the previous upward trend in the proportion of contacts resulting in admission, even though the overall proportion of admissions was higher. Preliminary observations from an ongoing investigation may offer some context for these developments. Early analyses of patients’ contact patterns prior to admission indicate a shift in help-seeking behaviour during the study period. Specifically, we observe indications of an increasing proportion of patients contacting the emergency medical number 1-1-2 rather than OOHS before admission. Moreover, we found a rise in patients being admitted without any preceding contact. These findings are unpublished and not yet peer-reviewed, and should therefore be interpreted with caution. Nevertheless, they may reflect broader changes in patient behaviour that could contribute to the observed decline in OOHS pathways and admissions.
Limitations
This study compares patient pathways in OOHS during Cooperative GP and 1818 from January 2017 to October 2023. The dataset is asymmetrically composed, with approximately 87% of contacts originating from GP-OOHS and 13% from 1818. This imbalance reflects the relative duration of each organizational period but may nonetheless limit the precision of comparative analyses. While the system used to record patient contacts and services was unchanged, there might have been differences in how patient pathways and underlying services were recorded, as physicians in 1818 were not enumerated per service delivered and hence might not have been as rigorous in recording all delivered services. However, registration was generally thorough across both organizational models. In the GP-OOHS, financial incentives may have encouraged more detailed service-level entries, whereas in 1818, structured registration procedures ensure consistent documentation. All patient contacts were required to be linked to at least one service code. Although the same coding rules applied in both systems, minor deviations cannot be excluded. By analysing complete patient pathways rather than individual services, the risk of differential under- or overcounting is minimized, as each pathway necessarily includes an initial registered service. However, we cannot exclude that call-backs within the same pathway may have contributed additional clinical information that is not fully captured in our pragmatic linkage of admissions to the highest-ranking interaction. These differences could influence the number of individual services but are unlikely to affect the integrity of patient pathway tracking.
Secondly, we have enriched the OOHS dataset with information on subsequent hospitalization. This is taken from the national patient database, and while the ED contact is within 24 h from the last contact to OOHS, the two contacts might not be related, though this is most likely. There is no referral information in the national patient database, so in this study, we assume the two contacts are linked, if admission appear within 24 h.
Finally, we have not had access to waiting time on calls to OOHS during the study period. It is known, that extended waiting times for OOHS can result in patients seeking out alternatives such as self-referral to ED or using emergency medical services [16]. This might result in a bias, which has not been investigated in this study.
Conclusion
In this retrospective cohort study of OOHS patient pathways in Region Zealand, Denmark, we investigated the effect of the new organization on admission to EDs. We found an overall decline in patient pathways in OOHS during the entire period and continuing after the organizational change. We found the decline in both the number of patient pathways in OOHS and the absolute number of patients admitted to an ED. However, the relative proportion of pathways resulting in ED admission increased slightly following the organizational change. These findings indicate a continued decline in OOHS activity and a slight shift toward more acute cases after the reorganisation.
Supplementary Material
Supplemental Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Steeman L, Uijen M, Plat E, et al. Out-of-hours primary care in 26 European countries: an overview of organizational models. Fam Pract. 2020;37(6):744–750. doi: 10.1093/fampra/cmaa 064.32597962 PMC 7699311 · doi ↗ · pubmed ↗
- 2Berchet C, Nader C. The organisation of out-of hours primary care in OECD countries. 2016.
- 3Huibers L, Giesen P, Wensing M, et al. Out-of-hours care in western countries: assessment of different organizational models. BMC Health Serv Res. 2009;9(1):105. doi: 10.1186/1472-6963-9-105.19549325 PMC 2717955 · doi ↗ · pubmed ↗
- 4Baier N, Geissler A, Bech M, et al. Emergency and urgent care systems in Australia, Denmark, England, France, Germany and the Netherlands - Analyzing organization, payment and reforms. Health Policy. 2019;123(1):1–10. doi: 10.1016/j.healthpol.2018.11.001.30503764 · doi ↗ · pubmed ↗
- 5Huibers L, Philips H, Giesen P, et al. Eur OO Hnet-the European research network for out-of-hours primary health care. Eur J Gen Pract. 2014;20(3):229–232. doi: 10.3109/13814788.2013.846320.24219341 · doi ↗ · pubmed ↗
- 6Bodenheimer T. Primary care in the United States. Innovations in primary care in the United States. BMJ. 2003;326(7393):796–799. doi: 10.1136/bmj.326.7393.796.PMC 15309912689977 · doi ↗ · pubmed ↗
- 7Søvsø MB, Huibers L, Bech BH, et al. Acute care pathways for patients calling the out-of-hours services. BMC Health Serv Res. 2020;20(1):146. doi: 10.1186/s 12913-020-4994-0.32106846 PMC 7045402 · doi ↗ · pubmed ↗
- 8Søvsø MB, Bech BH, Christensen HC, et al. Sociodemographic characteristics associated with contacts to emergency medical services and out-of-hours primary care: an observational study of 2.3 million citizens. Clin Epidemiol. 2020;12:393–401. doi: 10.2147/CLEP.S 243531.32346313 PMC 7167262 · doi ↗ · pubmed ↗