An unusual cause of upper gastrointestinal bleeding
Tony He, Gary May, Christopher Teshima

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
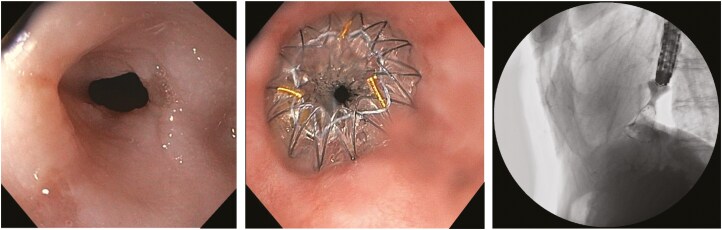 Figure 1
Figure 1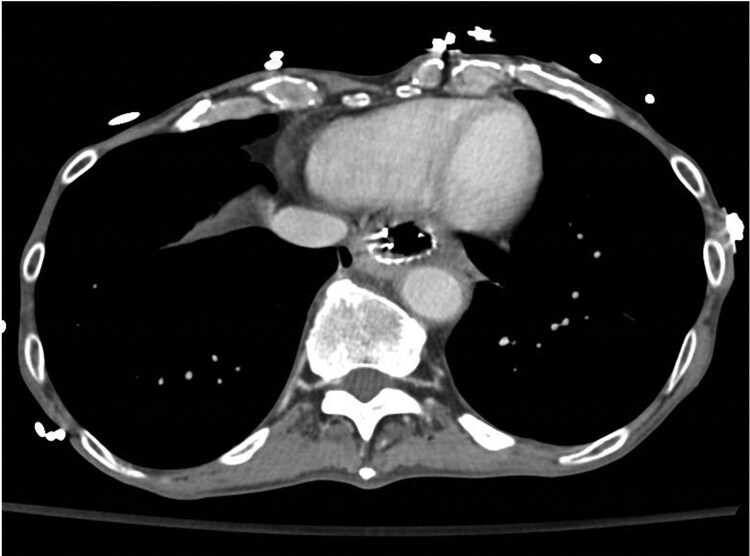 Figure 2
Figure 2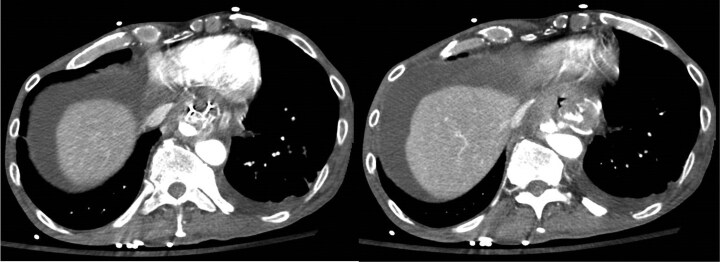 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Biliary and Gastrointestinal Fistulas · Gastrointestinal disorders and treatments
A 71-year-old gentleman presented with chronic dysphagia complicated by severe malnutrition secondary to a 1 cm length, 8 mm diameter recalcitrant distal oesophageal peptic stricture. This was on a background of spina bifida, alcohol dependence disorder, and neurogenic bladder requiring self-catheterization.
Between 2016 and 2023, the patient underwent serial dilatations with limited clinical benefit. He was then referred for placement of an oesophageal metal stent. A 14 mm wide × 30 mm long Hanaro Plumber metal stent was then placed (Figure 1).
Four days post-operatively, the patient returned with nausea and vomiting. Computed tomography (CT) did not identify a cause for his symptoms; however, the distance between the aorta and the oesophageal metal stent was 3.2 mm (Figure 2). Fourteen days post-operatively, the patient developed haematemesis complicated by severe hypotension requiring massive transfusion activation. An EGD revealed a large clot arising from within the oesophageal metal stent without a clear treatable target. A CT angiogram confirmed an aortic injury with pseudoaneurysm formation and active extravasation into the proximal stomach (Figure 3). Emergent thoracic endovascular repair was undertaken (Figure 4) and hemostasis was achieved. Despite successful hemostasis, the patient passed away 2 days later from multi-organ failure.
There are a small number of case reports that describe oesophageal stent-related aorto-oesophageal fistula (AEF) formation.^1–4^ Proposed risk factors include prior repeated dilatations, radiotherapy, or proximal stricture location.^3,4^ In our case, the bi-flanged metal stent may have also increased the risk of AEF formation secondary to local compression of the oesophageal mucosa. CT angiogram is the gold standard for diagnosis.^5^ AEF-associated mortality is approximately 75% with intervention and 100% without intervention.^5^ Prompt recognition of AEF to facilitate urgent intervention is therefore paramount.
Supplementary Material
gwae045_Supplementary_Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Unosawa S, Hata M, Sezai A, et al Surgical treatment of an aortoesophageal fistula caused by stent implantation for esophageal stenosis: report of a case. Surg Today. 2008;38(1):62–64. 10.1007/s 00595-007-3569-618085367 · doi ↗ · pubmed ↗
- 2Allgaier HP, Schwacha H, Technau K, Blum HE. Fatal esophagoaortic fistula after placement of a self-expanding metal stent in a patient with esophageal carcinoma. N Engl J Med. 1997;337(24):1778. 10.1056/NEJM 1997121133724179411255 · doi ↗ · pubmed ↗
- 3Siersema PD, Tan TG, Sutorius FF, Dees J, van Blankenstein M. Massive hemorrhage caused by a perforating Gianturco-Z stent resulting in an aortoesophageal fistula. Endoscopy. 1997;29(5):416–420. 10.1055/s-2007-10042279270927 · doi ↗ · pubmed ↗
- 4Uchida N, Katayama K, Sueda T. Endovascular stent graft for aortoesophageal fistula caused by esophageal stent. Asian Cardiovasc Thorac Ann. 2014;22(3):368. 10.1177/021849231247251724585925 · doi ↗ · pubmed ↗
- 5Bergqvist D. Arterioenteric fistula. Review of a vascular emergency. Acta Chirurgica Scandinavica 1987;153(2):81–86.3303777 · pubmed ↗