Postoperative chyle leak after pancreatic surgery: scoping review
Artur Rebelo, Enzo Rauchbach, Jörg Kleeff, Johannes Klose

TL;DR
This study reviews the occurrence and risk factors of chyle leak after pancreatic surgery, finding no significant difference between robotic and open procedures.
Contribution
The study provides a comprehensive scoping review comparing chyle leak incidence and risk factors in robotic versus open pancreatic surgery.
Findings
The pooled incidence of chyle leak after pancreatic resection was 8.0%.
No significant difference in chyle leak rates was found between robotic and open pancreatoduodenectomy.
Risk factors include female sex, diabetes, and malignancy.
Abstract
Chyle leak is a significant complication after pancreatic resection, associated with increased morbidity and mortality. Data on its incidence, risk factors, and treatment are inconsistent. Robotic pancreatic resections are increasingly performed and assumed to be associated with fewer complications than open surgery. This study evaluated the incidence, risk factors, and therapeutic strategies for chyle leak after both open and robotic pancreatic surgery. A scoping literature review was conducted across multiple databases to identify studies that included patients who underwent open or robotic pancreatic resection and experienced chyle leak as defined by the International Study Group on Pancreatic Surgery. The search period extended from database inception until 27 August 2025. In all, 58 studies published between 2007 and 2025 (30 039 patients) were included in the analysis. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
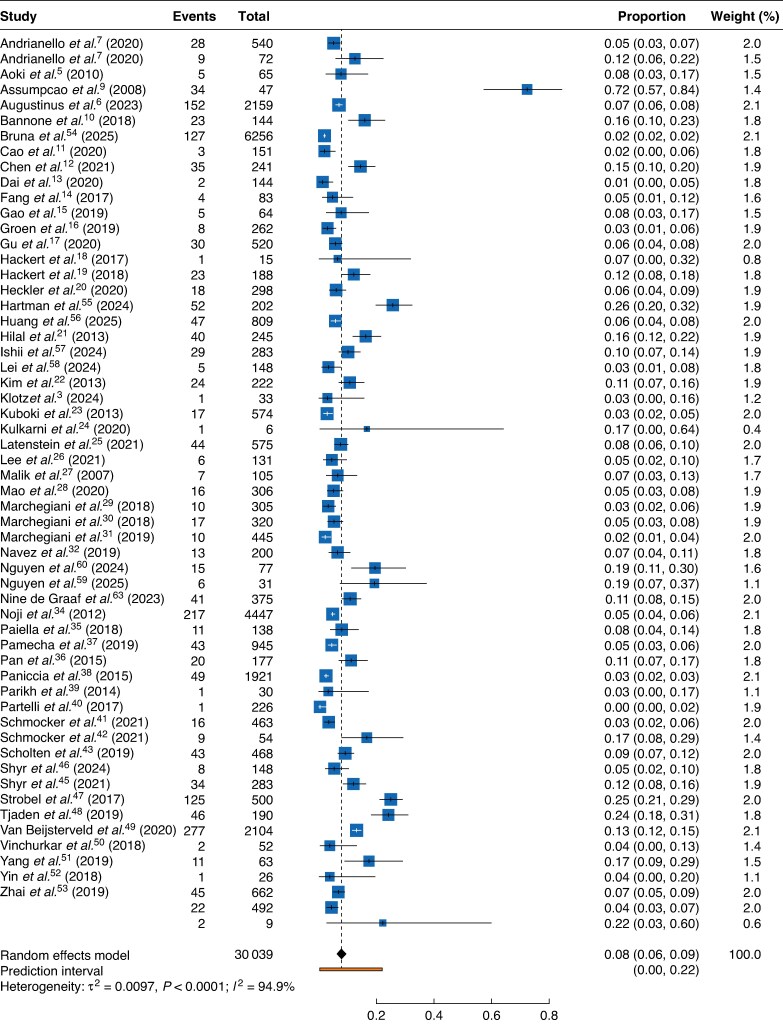 Fig. 1
Fig. 1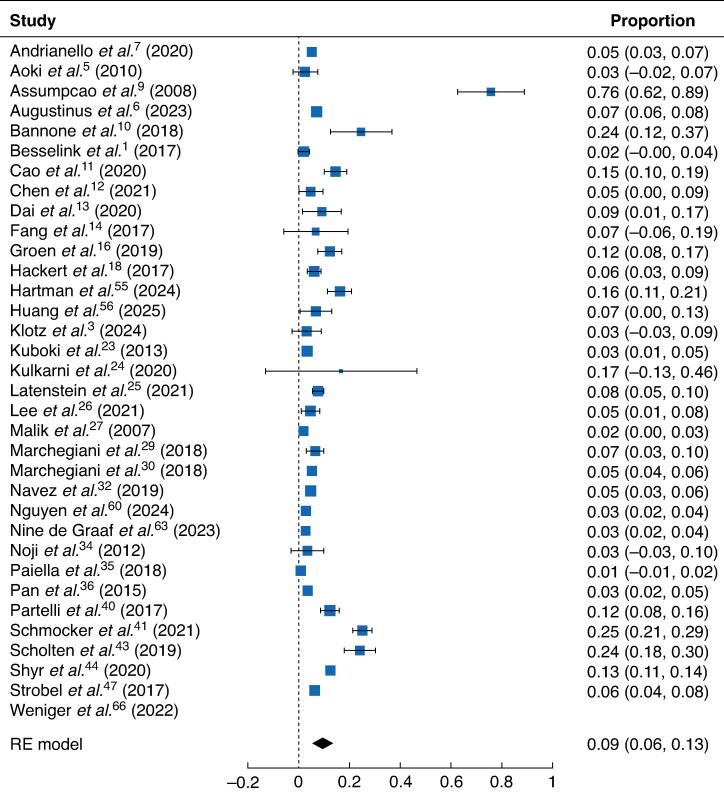 Fig. 2
Fig. 2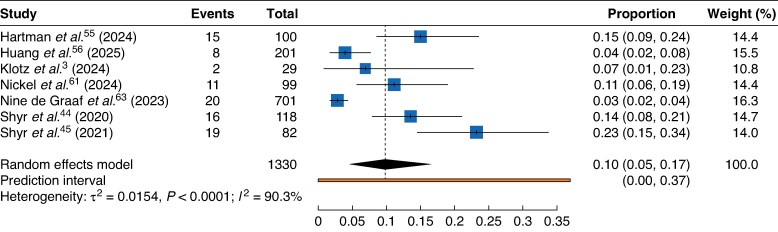 Fig. 3
Fig. 3| Study | Year | Inclusion period | No. of patients | Sex ( | Mean age (years) | Diabetes ( | Mean LOS (days) | |
|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||
| Andrianello | 2020 | 2017–2019 | 72 | 46 | 26 | 64 | 11 | 34 |
| Andrianello | 2020 | 2016–2019 | 540 | 304 | 236 | 63 | 76 | |
| Aoki | 2010 | 2001–2004 | 65 | |||||
| Assumpcao | 2008 | 1993–2008 | 3532 | 63.5 | ||||
| Augustinus | 2023 | 2017–2019 | 2159 | 1164 | 996 | 67.1 | 12 | |
| Bannone | 2018 | 2016–2017 | 292 | 166 | 126 | 64 | 51 | |
| Bruna | 2025 | 2007–2020 | 6256 | |||||
| Cao | 2020 | 2010–2017 | 151 | 92 | 59 | 59 | 25 | 19.7 |
| Chen | 2019 | 2014–2018 | 241 | 143 | 98 | 64 | 15.7 | |
| Dai | 2020 | 2014–2018 | 144 | 79 | 65 | 56.1 | 30 | 13.16 |
| Fang | 2017 | 2009–2014 | 83 | 55 | 28 | 70 | 14 | 19.35 |
| Gao net al. | 2019 | 2009–2016 | 64 | 34 | 30 | 64 | 12.5 | |
| Groen | 2018 | 2013–2017 | 262 | 133 | 129 | 63 | 9.5 | |
| Gu | 2020 | 2014–2019 | 520 | 214 | 306 | 63 | 10.75 | |
| Hackert | 2017 | 2016 | 15 | 7 | 8 | 60 | ||
| Hackert | 2018 | 2013–2016 | 188 | 104 | 84 | 63.3 | 37 | 14.75 |
| Hartman | 2024 | 2020–2024 | 202 | |||||
| Huang | 2025 | 2016–2023 | 809 | |||||
| Heckler | 2020 | 2006–2014 | 298 | 128 | 170 | 66 | ||
| Hilal | 2013 | 2007–2010 | 245 | 129 | 116 | 64.9 | 48 | |
| Ishii | 2024 | 2016–2022 | 283 | 141 | 142 | 76 | ||
| Lei | 2024 | 2017–2022 | 148 | 92 | 58 | |||
| Kim | 2013 | 2002–2010 | 222 | 115 | 107 | 61.3 | 25.05 | |
| Klotz | 2024 | 2020–2022 | 62 | 33 | 29 | 63.6 | 15 | |
| Kuboki | 2013 | 2000–2011 | 574 | 334 | 240 | 63.5 | ||
| Kulkarni | 2020 | 2012–2019 | 6 | 3 | 3 | 43.6 | ||
| Latenstein | 2021 | 2017–2018 | 575 | 315 | 260 | 68 | ||
| Lee | 2021 | 2014–2020 | 131 | 69 | 63 | 66.5 | 46 | |
| Malik | 2007 | 1999–2005 | 105 | 59 | 61,5 | 61.5 | ||
| Mao | 2020 | 2012–2014 | 306 | 186 | 120 | 62 | ||
| Marchegiani | 2018 | 2014–2016 | 445 | 238 | 207 | 65 | ||
| Marchegiani | 2018 | 2016–2017 | 320 | 167 | 153 | 62.9 | 53 | 11.4 |
| Marchegiani | 2018 | 2015–2016 | 91 | 51 | 40 | 63 | 16 | |
| Navez | 2019 | 2008–2017 | 200 | 105 | 95 | 65 | 18 | |
| de Graaf | 2023 | 2014–2021 | 1378 | 744 | 634 | 69 | ||
| Nguyen | 2024 | 2020–2022 | 77 | 43 | 34 | 58.2 | 20 | |
| Nguyen | 2025 | 2021–2023 | 31 | 16 | 15 | 58.7 | ||
| Nickel | 2024 | 2017–2022 | 375 | 212 | 163 | 64.9 | ||
| Noji | 2012 | 1995–2010 | 138 | 60 | 78 | 66 | ||
| Paiella | 2018 | 2014–2016 | 945 | 493 | 463 | 63 | 185 | 9 |
| Pamecha | 2019 | 2009–2018 | 177 | 131 | 46 | 57.1 | ||
| Pan | 2015 | 2007–2013 | 1921 | 1218 | 703 | 58.5 | ||
| Paniccia | 2015 | 2013–2014 | 30 | 63.1 | ||||
| Parikh | 2014 | 2007–2011 | 246 | 124 | 122 | 63 | 64 | |
| Partelli | 2017 | 2013–2015 | 463 | 261 | 202 | 68 | ||
| Schmocker | 2020 | 2008–2018 | 54 | 25 | 29 | 62.7 | 4 | |
| Schmocker | 2020 | 2011–2018 | 468 | 222 | 246 | 65 | 125 | |
| Scholten | 2019 | 2006–2016 | 148 | 82 | 60 | |||
| Shyr | 2020 | 2012–2017 | 283 | 129 | 129 | 24 | ||
| Shyr | 2021 | 2014–2019 | 451 | 240 | 211 | 65 | ||
| Shyr | 2023 | 2012–2021 | 132 | 41 | 47 | 67 | ||
| Strobel | 2017 | 2008–2012 | 2881 | 738 | ||||
| Tjaden | 2019 | 2001–2018 | 52 | 8 | 44 | 29 | 3 | 10 |
| Van Beijsterveld | 2020 | 2016–2018 | 63 | 31 | 32 | 68 | 6 | 14 |
| Vinchurkar | 2018 | 2012–2016 | 26 | 14 | 12 | 55 | ||
| Yang | 2015 | 2009–2016 | 1921 | 1218 | 703 | 58.5 | ||
| Yang | 2019 | 2006–2018 | 59 | 35 | 24 | 62 | ||
| Yin | 2018 | 2012–2014 | 492 | 315 | 177 | 60.5 | 13.5 | |
| Zhai | 2019 | 2017–2018 | 9 | 7 | 2 | 63.3 | 4 | 29 |
| Study | Male | Female | Pancreatic adenocarcinoma | Cholangiocarcinoma | Duodenal adenocarcinoma | Ampullary carcinoma | Other diagnosis |
|---|---|---|---|---|---|---|---|
| Andrianello | 46 (–) | 26 (–) | 21 (–) | 9 (–) | 9 (–) | 11 (–) | 20 (–) |
| Andrianello | 304 (–) | 236 (–) | |||||
| Aoki | − (4) | − (1) | |||||
| Assumpcao | − (25) | − (22) | − (32) | − (2) | − (4) | − (8) | − (1) |
| Augustinus | 1164 (83) | 995 (69) | 1193 (83) | 315 (23) | 259 (21) | 339 (20) | |
| Bannone | 166 (–) | 126 (–) | 186 (–) | 0 | 0 | 0 | 106 (–) |
| Bruna | 127 (6256) | ||||||
| Cao | 92 (–) | 59 (–) | |||||
| Chen | 143 (–) | 98 (–) | 109 (–) | 65 (–) | 11 (–) | 31 (–) | 25 (–) |
| Dai | 79 (–) | 65 (–) | 72 (–) | 6 (–) | 6 (–) | 9 (–) | 32 (–) |
| Fang | 55 (–) | 28 (–) | |||||
| Gao net al. | 34 (–) | 30 (–) | |||||
| Groen | 133 (–) | 129 (–) | |||||
| Gu | 214 (–) | 306 (–) | 263 (–) | 0 | 0 | 51 (–) | 206 (–) |
| Hackert | 7 (–) | 8 (–) | |||||
| Hackert | 104 (–) | 84 (–) | 80 (–) | 0 | 0 | 0 | 108 (–) |
| Hartman | 128 (–) | 170 (–) | 224 (–) | 31 (–) | 0 | 26 (–) | 17 (–) |
| Huang | 52 (202) | ||||||
| Heckler | 47 (809) | ||||||
| Hilal | 129 (20) | 116 (20) | 110 (19) | 26 (6) | 8 (2) | 40 (3) | 34 (6) |
| Ishii | 29 (283) | ||||||
| Lei | 5 (148) | ||||||
| Kim | 115 (9) | 107 (15) | 85 (8) | 69 (7) | 11 (1) | 54 (7) | 3 (1) |
| Klotz | 33 (–) | 29 (–) | 22 (–) | 3 (–) | 0 | 3 (–) | 5 (–) |
| Kuboki | 334 (9) | 240 (8) | |||||
| Kulkarni | 3 (–) | 3 (–) | 2 (–) | 0 | 0 | 4 (–) | |
| Latenstein | 315 (–) | 260 (–) | 310 (–) | 152 (–) | 14 (–) | 99 (–) | 0 |
| Lee | 69 (–) | 63 (–) | 19 (–) | 45 (–) | 3 (–) | 29 (–) | 36 (–) |
| Malik | 59 (2) | 61 (5) | |||||
| Mao | 186 (–) | 120 (–) | 206 (–) | 0 | 0 | 0 | 0 |
| Marchegiani | 238 (–) | 207 (–) | 445 (–) | 0 | 0 | 0 | 0 |
| Marchegiani | 167 (–) | 153 (–) | 168 (–) | 0 | 0 | 0 | 152 (–) |
| Marchegiani | 51 (–) | 40 (–) | 42 (–) | 2 (–) | 1 (–) | 7 (–) | 39 (–) |
| Navez | 105 (–) | 95 (–) | |||||
| de Graaf | 744 (–) | 634 (–) | 464 (–) | 194 (–) | 103 (–) | 225 (–) | 392 (–) |
| Nguyen | 15 (77) | ||||||
| Nguyen | 6 (31) | ||||||
| Nickel | 41 (375) | ||||||
| Noji | 60 (4) | 78 (7) | 59 (–) | 0 | 0 | 0 | 79 (–) |
| Paiella | 493 (20) | 463 (23) | 445 (18) | 38 (1) | 0 | 78 (3) | 395 (21) |
| Pamecha | 131 (–) | 46 (–) | 0 (–) | 42 (–) | 19 (–) | 83 (–) | 0 |
| Pan | 1218 (32) | 703 (17) | |||||
| Paniccia | |||||||
| Parikh | 124 (–) | 122 (–) | |||||
| Partelli | 261 (–) | 202 (–) | |||||
| Schmocker | 25 (–) | 29 (–) | |||||
| Schmocker | 222 (–) | 246 (–) | |||||
| Scholten | 72 (–) | 4 (–) | 1 (–) | 3 (–) | 68 (–) | ||
| Shyr | 129 (20) | 129 (14) | 96 (18) | 0 | 0 | 0 | 187 (16) |
| Shyr | 240 (–) | 211 (–) | 176 (–) | 30 (–) | 23 (–) | 103 (–) | 119 |
| Shyr | 41 (–) | 47 (–) | |||||
| Strobel | |||||||
| Tjaden | 8 (–) | 44 (–) | |||||
| Van Beijsterveld | 31 (–) | 32 (–) | 42 (–) | 0 | 0 | 0 | 21 (–) |
| Vinchurkar | 14 (–) | 12 (–) | 0 | 0 | 0 | 26 (–) | 0 |
| Yang | 1218 (–) | 703 (–) | 878 (–) | 288 (–) | 0 | 137 (–) | 272 (–) |
| Yang | 35 (–) | 24 (–) | 34 (–) | 0 | 0 | 0 | 25 (–) |
| Yin | 315 (–) | 177 (–) | 272 (–) | 51 (–) | 91 (–) | 68 (–) | 10 (–) |
| Zhai | 7 (–) | 2 (–) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphatic Disorders and Treatments · Abdominal vascular conditions and treatments · Pleural and Pulmonary Diseases
Introduction
According to the International Study Group on Pancreatic Surgery^1^, chyle leak is defined as the output of milky-coloured fluid from a drain, drain site, or wound on or after postoperative day 3, with a triglyceride content ≥ 110 mg/dl. Recent data suggest that chyle leak may occur in approximately one in eight patients after pancreatic resection^1^. A systematic review by Varghese et al.^2^ identified several risk factors for the occurrence of chyle leak after pancreatic resection, including patient-dependent and patient-independent variables. However, it should be noted that these data were obtained in the pre-robotic era and compared laparoscopic with open surgical approaches.
Robotic pancreatic resection is associated with several potential advantages, including lower rates of postoperative complications and therefore lower rates of postoperative morbidity^3^. Data from the EUROPA trail suggest no lower rates of chyle leak after robotic pancreatoduodenectomy^3^. However, the incidence of chyle leak after robotic pancreatic resection has not been investigated systematically as yet. Thus, the aim of the present study was to analyse the incidence of and risk factors for chyle leak after pancreatic resection, focusing on the comparison between open and robotic surgical approaches.
Methods
Search strategy
A literature search and data analysis were conducted according to the PRISMA extension for scoping reviews guidelines^4^ to identify studies that included patients who underwent open or robotic pancreatic resection and experienced lymphatic fistula. This study has been registered in the PROSPERO database (CRD42024575905).
A comprehensive literature search was conducted across the PubMed/MEDLINE, Web of Science Core Collection, Cochrane Library, and ClinicalTrials.gov databases (Supplementary Figure 1). Searches were performed via the respective online search engines and covered the period from database inception to 27 August 2025. The full search strategy is provided in the supplementary methods.
Following the literature search, all records identified were imported into reference management software, and duplicates were removed. Two reviewers (A.R., E.R.) independently screened titles and abstracts to identify studies relevant to the review question using predefined eligibility criteria. Records were categorized as ‘include’, ‘exclude’, or ‘unclear’. The full text of all potentially relevant or unclear records was retrieved and the articles were screened independently by the same two reviewers. Disagreements at any stage were resolved through discussion, and a third reviewer (J.Klo.) was consulted if consensus could not be reached.
The reference lists of all included studies were also manually screened to identify further potentially relevant publications. Targeted hand-searching and author-based searches were also conducted to capture additional studies that may not have been retrieved through the initial database search.
Inclusion and exclusion criteria
Only articles published in English were considered for inclusion. Studies with patients undergoing pancreatic surgery (partial pancreatoduodenectomies, distal pancreatectomies, total pancreatectomies, and enucleations) that reported on the occurrence of lymphatic fistula were included. Review articles, case reports, case series with fewer than five patients, commentaries, and letters were excluded. In addition, patients who only underwent exploration were excluded from the analysis.
Data collection
Data from the included studies were extracted separately by two authors (A.R., E.R.) and stored in a dedicated database. The following descriptive data were documented for each included study: the total numbers and subsets of pancreatoduodenectomies (standard and robotic), pylorus-preserving pancreatoduodenectomies, distal pancreatectomies, mixed procedures (if no specific type of pancreatic resection was documented), total pancreatectomies, and enucleations; demographic data, including patient sex and age; clinical variables such as diabetes status, length of hospital stay, operation time, and the occurrence of pancreatic fistulas; and oncological diagnosis regarding pancreatic head adenocarcinoma, cholangiocarcinoma, ampullary carcinoma, and duodenal adenocarcinoma, classified as total, positive, or negative for chyle leak.
In every study, the risk of bias was evaluated using the Newcastle–Ottawa Scale^5^.
Statistical analysis
In line with the descriptive aims of this scoping review, pooled incidence rates for selected outcomes were calculated using a random effects model in Jamovi (version 2.3). Additional data handling and descriptive analysis were conducted using SPSS^®^ version 29 (IBM, Armonk, NY, USA). No quantitative synthesis was performed due to the high heterogeneity of the included studies.
Results
After excluding non-relevant articles, 58 studies^3,6–62^ including 30 039 patients and published between 2007 and 2025 were reviewed and included in this analysis (Table 1). The reported incidence of chyle leak after pancreatic resection varied considerably across studies, ranging from 1 to 72%. The pooled incidence of chyle leak across all 30 039 pancreatic resections was 8.0% (Fig. 1).
Pooled incidence of chyle leak after all pancreatic resectionsValues in parentheses are 95% confidence intervals.
Demographic risk factors
Eight studies reported the sex-stratified incidence of chyle leak (Table 2). The incidence of chyle leak ranged from 3.4 to 15.5% in male patients and from 5.0 to 17.2% in female patients. Across studies, the direction and magnitude of differences between sexes were inconsistent: some studies reported slightly higher rates for female patients and others reported higher rates for male patients. No systematic sex-related trend could be identified. Given the heterogeneity in study design, surgical procedures, and outcome reporting, no pooled analysis was performed.
Diagnosis
Only a subset of studies reported pooled incidence stratified by diagnosis (Table 2). A subset of studies reported chyle leak incidence stratified by underlying diagnosis (Table 2). Among patients with pancreatic ductal adenocarcinoma, the reported incidence of chyle leak ranged from 3.5 to 18.8%. For cholangiocarcinoma, the incidence of chyle leak ranged from 4.3 to 15.1%, whereas rates of chyle leak in duodenal adenocarcinoma ranged from 5.3 and 18.4%. In patients with ampullary carcinoma, the incidence of chyle leak incidence ranged from 3.6 to 13.3%. Across studies, no consistent trend indicating higher or lower chyle leak rates by tumour type could be identified.
Type of surgery
The pooled incidence of chyle leak after partial pancreatoduodenectomy, as estimated using a random effects model, was 9.50% (Fig. 2). Patients from 33 studies were included in the analysis. The incidence of chyle leak after pylorus-preserving pancreatoduodenectomy was reported in a smaller subset of studies (Fig. S2); among these patients, the pooled incidence of chyle leak was 8.36%. The pooled incidence of chyle leak, estimated using a random effects model, was 6.89% (Fig. S3) after distal pancreatectomy, 1.70% after enucleation (Fig. S4), and 6.22% after total pancreatectomy (Fig. S5).
Pooled incidence of chyle leak after pancreatoduodenectomyValues in parentheses are 95% confidence intervals. RE, random effects.
Robotic pancreatoduodenectomy
Seven studies published between 2020 and 2025, including a total of 6339 patients, compared chyle leak after robotic versus open pancreatoduodenectomy. The pooled incidence of chyle leak across these studies was 11%.
Across seven studies including 1330 patients who underwent robotic pancreatoduodenectomy, the reported incidence of chyle leak ranged from 3 to 23%. The pooled incidence of chyle leak in this group was 10% (Fig. 3), whereas among the 5739 patients in the open surgery group, the pooled incidence was 12%.
Pooled incidence of chyle leak after robotic pancreatoduodenectomyValues in parentheses are 95% confidence intervals.
Discussion
The aim of the present comprehensive scoping review was to investigate the incidence of chyle leak after open and robotic pancreatic surgery. This study revealed that chyle leak is a frequent complication after pancreatic surgery, independent of the type of resection, and that robotic pancreatic resection is not associated with a clinically significant reduction in the rate of postoperative chyle leak.
There is no doubt as to the importance of chyle leak as a major complication after pancreatic surgery. Chyle leak may result in extended hospitalization periods, leading to increased healthcare costs and the consumption of medical resources. In addition, the initiation of adjuvant therapies may be delayed in patients with chyle leak after pancreatic surgery, resulting in impaired long-term outcomes^63^.
Further analysis revealed that the pooled incidence of chyle leak was higher after partial pancreatoduodenectomy, followed by distal pancreatectomy, total pancreatectomy, and finally enucleation. Strikingly, no significant interprocedural differences in the incidence of chyle leak were observed. In 2017, Strobel et al.^48^ reported that among more than 3000 patients, distal pancreatectomy was associated with a higher risk of postoperative chyle leak than other resections (P = 0.001). These data were quite surprising given that it was assumed that partial pancreatoduodenectomy would be associated with the highest risk of postoperative chyle leak^10^.
Minimally invasive pancreatic surgery, especially robotic-assisted surgery, raised hopes of a reduction in complications associated with the open approach. In the EUROPA trial^3^, a single-centre randomized clinical study, equivalent rates of chyle leak were reported after robotic partial pancreatoduodenectomy and open surgery, similar to the findings of a Dutch retrospective observational cohort study^7^. In another Dutch study, which compared only robotic and open partial pancreatoduodenectomy, revealed a trend towards lower rates of postoperative chyle leak after robotic resection^34^. Shyr et al.^64^ reported no differences in the incidence of chyle leak after robotic versus open partial pancreatoduodenectomy. Given that the surgical technique may not influence the risk of postoperative chyle leak, it is possible that the underlying disease might. This could also be explained by the fact that robotic partial pancreatoduodenectomy is reserved for relatively smaller tumours that do not require vascular resection. Only limited data on the extent of lymphatic tissue clearance during robotic pancreatoduodenectomy have been reported. The triangle operation is defined as complete removal of any lymphatic tissue between the portal vein, the coeliac trunk, and the superior mesenteric artery^45^. Data on the incidence of chyle leak are inconsistent, but extended resections appear to be associated with a higher risk of chyle leak^65^. Another recent study demonstrated that minimally invasive surgery is a risk factor for postoperative chyle leak after pancreatic resections^66^. Strobel et al.^48^ identified pancreatic ductal adenocarcinoma as a risk factor for postoperative chyle leak (adjusted hazard ratio 2.03; P < 0.001). Malik et al.^28^ found no significant effect of T or N tumour stage on lymphatic fistula formation, whereas Shyr et al.^45^ reported a significantly (P = 0.019) higher rate of lymphatic fistulas in patients with pancreatic head adenocarcinoma. Lymph node metastases, the number of lymph nodes removed, and the number of positive lymph nodes were identified as individual risk factors for lymphatic fistula formation.
Several studies reported that vascular resection during surgery increased the risk of lymphatic fistulas. The duration of surgery also emerged as a significant factor, with longer operations linked to higher risks^10^.
Therapeutic strategies for chyle leak were not analysed in this study. Conservative treatment and a fat-reduced or fat-free diet are therapeutic options for patients with grade A or B chyle leak^28^. Therapeutic lymphography may be an option for patients with grade C chyle leak, with encouraging data from a single-centre experience^67^.
This scoping review has several limitations. This analysis included not only on randomized clinical trials but also observational studies, causing heterogeneity in outcome definitions and treatments. The retrospective design across studies enhanced the risk for potential selection bias. The results stem from non-randomized, uncontrolled comparisons of patients with diverse backgrounds, lacking a clear distinction between groups receiving several therapies across all studies. Despite efforts to ensure transparency and standardized reporting, a notable risk of bias persists. Caution is warranted in the interpretation and application of the data. This study was also subject to confounding variables and bias and is hampered by the quality of the pooled studies underlying the analysis. Across all studies, heterogeneity was frequently high, reflecting substantial variability in the reported incidence of chyle leak. This variability may stem from differences in patient populations, surgical techniques, perioperative management strategies, and definitions of chyle leak across studies.
Future research should focus on standardizing the definition and reporting of chyle leak to improve comparability across studies. High-quality prospective multicentre studies are needed to better characterize patient- and procedure-specific risk factors, and to develop targeted prevention strategies. The impact of surgical modifications, intraoperative lymphatic management techniques, and enhanced recovery protocols should be further explored to reduce the incidence and clinical burden of chyle leak following pancreatic surgery. Addressing these areas will help refine perioperative management and improve postoperative outcomes for patients undergoing pancreatic resections.
Supplementary Material
zraf146_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Besselink MG, van Rijssen LB, Bassi C, Dervenis C, Montorsi M, Adham M et al Definition and classification of chyle leak after pancreatic operation: a consensus statement by the international study group on pancreatic surgery. Surgery 2017;161:365–37227692778 10.1016/j.surg.2016.06.058 · doi ↗ · pubmed ↗
- 2Varghese C, Wells CI, Lee S, Pathak S, Siriwardena AK, Pandanaboyana S. Systematic review of the incidence and risk factors for chyle leak after pancreatic surgery. Surgery 2022;171:490–49734417025 10.1016/j.surg.2021.07.021 · doi ↗ · pubmed ↗
- 3Klotz R, Mihaljevic AL, Kulu Y, Sander A, Klose C, Behnisch R et al Robotic versus open partial pancreatoduodenectomy (EUROPA): a randomised controlled stage 2b trial. Lancet Reg Health Eur 2024;39:10086438420108 10.1016/j.lanepe.2024.100864 PMC 10899052 · doi ↗ · pubmed ↗
- 4Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D et al PRISMA extension for scoping reviews (PRISMA-Sc R): checklist and explanation. Ann Intern Med 2018;169:467–473. doi: 10.7326/M 18-085030178033 · doi ↗ · pubmed ↗
- 5Lo CKL, Mertz D, Loeb M. Newcastle–Ottawa scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol 2014;14:4524690082 10.1186/1471-2288-14-45PMC 4021422 · doi ↗ · pubmed ↗
- 6Aoki H, Takakura N, Shiozaki S, Matsukawa H. Milk-based test as a preventive method for chylous ascites following pancreatic resection. Dig Surg 2010;27:427–43220975273 10.1159/000320692 · doi ↗ · pubmed ↗
- 7Augustinus S, Latenstein AEJ, Bonsing BA, Busch OR, Groot Koerkamp B, de Hingh IHJT et al Chyle leak after pancreatoduodenectomy: clinical impact and risk factors in a nationwide analysis. Ann Surg 2023;277:e 1299–e 130535786606 10.1097/SLA.0000000000005449 PMC 10174101 · doi ↗ · pubmed ↗
- 8Andrianello S, Marchegiani G, Malleo G, Masini G, Balduzzi A, Paiella S et al Pancreaticojejunostomy with externalized stent vs pancreaticogastrostomy with externalized stent for patients with high-risk pancreatic anastomosis: a single-center, phase 3, randomized clinical trial. JAMA Surg 2020;155:313–32132101272 10.1001/jamasurg.2019.6035 PMC 7160692 · doi ↗ · pubmed ↗