Risk factors for saccular unruptured intracranial aneurysms: a systematic review and meta-analysis
Maaike J A van Eldik, Mariam Ali, Stijn Rietkerken, Jan W Schoones, Sanne A E Peters, Hester M den Ruijter, Ynte M Ruigrok

TL;DR
This study identifies hypertension and smoking as risk factors for unruptured intracranial aneurysms but notes a lack of data on sex differences.
Contribution
The study provides a systematic review and meta-analysis of risk factors for saccular unruptured intracranial aneurysms, highlighting gaps in sex-specific data.
Findings
Hypertension increases the risk of unruptured intracranial aneurysms (OR 1.72).
Smoking is associated with a higher risk of unruptured intracranial aneurysms (OR 1.47).
Other risk factors like alcohol use and diabetes showed no significant associations.
Abstract
Intracranial aneurysms are often unruptured and two-thirds of patients with unruptured intracranial aneurysms (UIAs) are women. Rupture of an intracranial aneurysm causes aneurysmal subarachnoid haemorrhage (aSAH). While risk factors for aSAH have been extensively studied, those for UIA remain less well understood. We performed a systematic review and meta-analysis to identify risk factors for the presence of saccular UIAs and assess potential sex differences. We conducted a systematic review and meta-analysis of cohort, case–control, and cross-sectional studies on risk factors for UIA up to March 2024. Assessed risk factors included smoking, hypertension, alcohol use, diabetes, hypercholesterolaemia, physical activity, and body mass index. We performed random-effects meta-analyses to calculate pooled odds ratios (ORs) and 95% CIs for each risk factor. We identified 21 studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
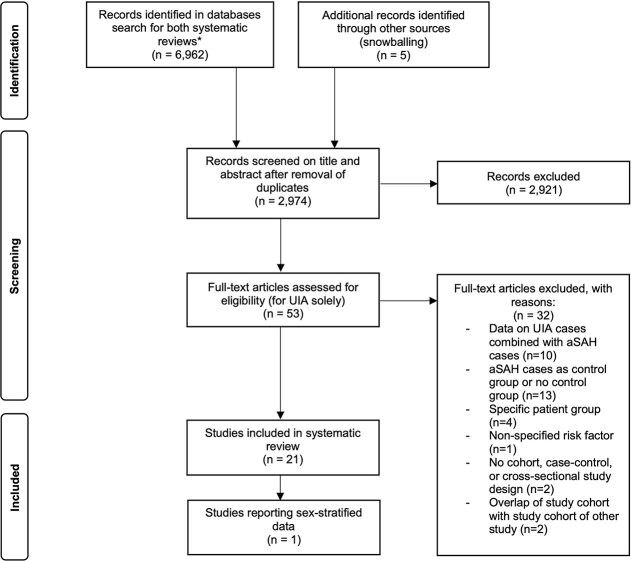 Figure 1
Figure 1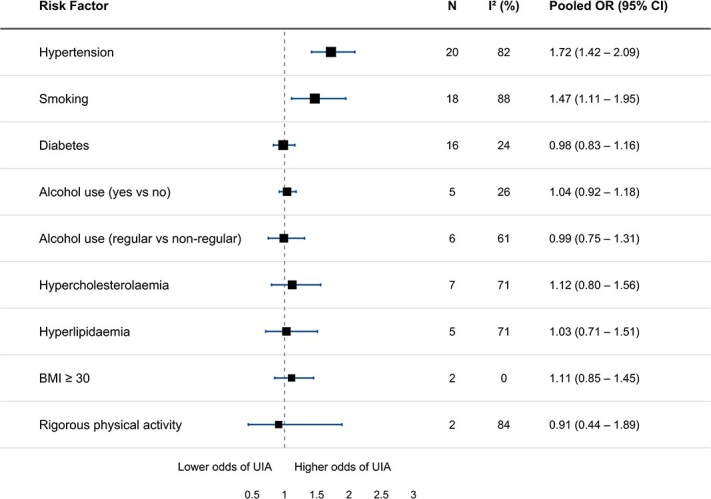 Figure 2
Figure 2|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|
| Horikoshi 2002, Japan | Case–control | 381 (unclear) | 44–85 | 127 (66) | 1997—2000 | MRA, CTA, DSA | Hypertension, hypercholesterolaemia |
| Inagawa 2010, Japan | Case–control | 1064 (65) | 34–88 | 266 (65) | 1981—2005 | MRA, CTA, angiography | Hypertension, smoking, diabetes, alcohol use, hypercholesterolaemia |
| Chen 2011, USA | Case–control | 459 (100) | 31–80 | 39 (100) | 2008—2010 (questionnaires 1994-1998) | “brain vascular imaging” | Smoking |
| Vlak 2013, The Netherlands | Case–control | 780 (69) | Mean age 55 | 206 (67) | 2006—2010 | CTA, MRA or conventional angiography | Hypertension, diabetes, alcohol use, hypercholesterolaemia, BMI, physical activity |
| Li 2013, China | Cross-sectional | 4813 (51) | 35–75 | 366 (56) | 2007–2011 | MRA | Hypertension, smoking, diabetes, alcohol use |
| Jing Li 2014, China | Cross-sectional | 3993 (46) | 20–80 | 350 (57) | 2009–2010 | 3D CE-MRA | Hypertension, smoking, diabetes, alcohol use, hyperlipidaemia |
| Matsukawa 2014, China | Case–control | 132 (67) | Mean age 62 | 66 (67) | 2013–2014 | MRA, CTA, DSA | Hypertension, diabetes, alcohol use, hypercholesterolaemia |
| Zhang 2015, China | Case–control | 294 (46) | Mean age 51 | 37 (49) | Unclear | CTA, DSA | Hypertension, smoking, diabetes, alcohol use, hypercholesterolaemia |
| Kang 2015, South-Korea | Cross-sectional | 18 954 (39) | Mean age 57 | 367 (51) | 2004–2014 | MRA | Hypertension, smoking, diabetes, alcohol use |
| Kim Tackeun 2016, Korea | Prospective cohort study | 131 999 (41) | Unclear | 491 (59) | 2005–2013 | ICD-10 code I67.1 | Hypertension, smoking, diabetes, BMI, physical activity, alcohol use, hypercholesterolaemia |
| Atchaneeyasakul 2018, USA | Case–control | 486 (53) | Mean age 61 | 243 (71) | 2004–2014 | DSA | Hypertension, smoking, diabetes, alcohol use, hyperlipidaemia |
| Imaizumi 2018, Japan | Cross-sectional | 4070 (42) | Mean age 51 | 176 (60) | 2014–2015 | MRI/MRA | Hypertension, smoking, diabetes, hyperlipidaemia |
| Yoon 2019, South-Korea | Case–control | 238 (32) | 18+, mean age 62 | 25 (36) | 2014–2016 | MRA or CTA | Hypertension, smoking, diabetes |
| Müller 2019, Norway | Prospective cohort study | 83 710 (53) | Unclear | 92 (75) | 1999–2014 | MRA, CTA, DSA | Hypertension, smoking |
| Cras 2020, The Netherlands | Cross-sectional | 5841 (55) | Mean age 64 | 134 (68) | 2005–2015 | MRI | Hypertension, smoking, diabetes, hypercholesterolaemia |
| Ogilvy 2020, USA (single centre) | Case–control | 194 (100) | 30–60 | 64 (100) | 2016–2018 | MRA | Hypertension, smoking, diabetes |
| Ogilvy 2020, USA and Canada (multicentre) | Case–control | 226 (100) | 30–60 | 113 (100) | 2016–2018 | MRA | Hypertension, smoking, diabetes |
| Kim Jae Ho 2021, Korea | Cross-sectional | 2118 (44) | Mean age 54 | 80 (55) | 2011–2012 | MRA | Hypertension, smoking, diabetes, hyperlipidaemia |
| Igase 2021, Japan | Cross-sectional | 1376 (59) | 31–91 | 79 (70) | 2006–2013 | MRA | Hypertension, smoking, diabetes |
| Räisänen 2022, Finland | Retrospective cohort study | 1419 (50) | Median age 46 | 42 (50) | 1975–2014 | MRA, CTA, or 4-vessel DSA | Hypertension, smoking, alcohol use |
| Park 2023, Korea | Case–control | 85 360 (68) | Mean age 60 | 5335 (68) | 2003–2019 | ICD-10 code I67.1 | Hypertension, smoking, alcohol use |
- —Dutch Heart Foundation
- —European Research Council under the European Union’s Horizon 2020 research and innovation program
- —VIDI Fellowship
- —Dutch Organization for Health Research and Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Neurological Complications and Syndromes · Cerebral Venous Sinus Thrombosis
Introduction
Unruptured intracranial aneurysms (UIAs) have a prevalence of approximately 3% in the general population.1 Rupture of an intracranial aneurysm causes aneurysmal subarachnoid haemorrhage (aSAH), a severe type of stroke with approximately one in three patients dying and one in three patients remaining dependent.2 Both UIA and aSAH are more common in women than in men, with overall two-thirds of patients being women.1^,^3 The reasons for this female preponderance remain unclear.
The risk of aSAH depends on both the development of UIAs and their subsequent rupture. It remains unclear whether risk factors for both stages overlap or whether distinct risk factors exist for each stage. It is therefore important to identify which risk factors contribute to UIA formation, as reducing the risk of developing UIAs represents a key strategy for lowering the incidence of aSAH. For aSAH, previous studies, including our recently updated meta-analysis, identified smoking, hypertension, and excessive alcohol use as the most important risk factors.^4,5^ In contrast, rigorous physical activity and diabetes were associated with a reduced risk of aSAH, while associations with hypercholesterolaemia and body mass index (BMI) remained inconclusive.^4^ However, research on similar modifiable risk factors for UIA is less extensive. To date, only hypertension and smoking are well-established, with limited evidence for other modifiable risk factors for UIA.^3,6-10^
Sex differences in the strength of certain risk factor associations may contribute to the higher burden of UIA and aSAH in women. In our recently updated meta-analysis, we confirmed that smoking was more strongly associated with aSAH in women than in men,^4^ but if sex differences exist for UIA is unknown.
Therefore, we performed a systematic review and meta-analysis to identify risk factors for the presence of saccular UIAs and to assess potential sex differences in these risk factor relations.
Patients and methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses Statement guidelines and followed a prospectively registered protocol in PROSPERO (CRD42024529043).^11^
Data sources and search strategy
We performed a systematic search of the databases PubMed, Embase, Web of Science, Cochrane Library, and Emcare from database inception until March 2024 using search terms related to (1) UIAs, (2) predefined specific risk factors, and (3) cohort, case–control, and cross-sectional studies. Concurrently, we conducted a separate systematic review and meta-analysis on risk factors for aSAH.^8^ Given that both reviews examined the same preselected risk factors, we used a unified search strategy and conducted the screening process jointly. The search excluded reviews, case-reports, and non-English publications. A medical information specialist with expertise in systematic reviews was consulted for help in developing the search strategy. In addition, we screened the reference lists of the included articles to identify any additional eligible studies. The full search strategy is provided in Supplementary Material S1.
Selection criteria
Inclusion criteria were: (1) cohort, case–control, or cross-sectional studies reporting on risk factors associated with the presence of saccular UIAs, with no minimum sample size restriction; (2) provision of crude or adjusted effect estimates with 95% CIs for smoking, hypertension, alcohol use, diabetes, hypercholesterolaemia, rigorous physical activity, and BMI, or data allowing for their calculation; (3) confirmation of UIA presence by neuroimaging (computed tomography angiography, magnetic resonance angiography, or conventional angiography), autopsy or International Classification of Diseases codes; (4) patients aged ≥18 years; and (5) articles in English. In case of multiple publications originating from the same study population, we included data from the most recent publication.
We excluded studies (1) that analysed UIA and aSAH cases together without separate results for UIA; and (2) that focused on specific patient subgroups, such as young patients (defined as age <50 years), those with familial, fusiform, or multiple aneurysms, a specific aneurysm location or size, and those focused on UIAs related to Marfan syndrome, Loeys-Dietz syndrome, autosomal dominant polycystic kidney disease, fibromuscular dysplasia, and Ehlers-Danlos syndrome (more details available in Supplementary Material S2).
Data extraction and quality assessment
To determine study eligibility, two reviewers (M.J.A.v.E. and M.A.) independently screened titles and abstracts using the predefined in- and exclusion criteria. Subsequently, one reviewer (M.J.A.v.E.) screened full-text versions of potentially relevant articles and performed the data extraction and quality assessment of studies meeting the inclusion criteria. A second reviewer (S.R.) independently verified 50% of the full-text screenings, data extraction forms, and quality assessments, based on a predefined protocol. Data were extracted using a standardised data extraction form (more details available in Supplementary Material S3).
For quality assessment, we used an adapted version of the Newcastle-Ottawa Scale.^12^ Each study was rated as having low, high, or unclear risk of bias across the following domains (1) validation of diagnosis, (2) assessment of risk factors, (3) adjustment for confounding, and (4) generalizability (Supplementary Material S4). Disagreements at any stage, including title and abstract screening, duplicate full-text screening, data extraction, or quality assessment, were resolved through discussion with a third reviewer (Y.M.R.).
Definition and classification of risk factors
To ensure comparability of data across studies, we standardised risk factor definitions wherever possible. We categorised smoking into (1) ever smokers and (2) never smokers. Alcohol use was categorised both as (1) alcohol use vs. no alcohol use, and (2) regular use vs. non-regular use. Lipid levels often lacked precise definitions and were reported as either hypercholesterolaemia or hyperlipidaemia (the latter being a broader term that includes both cholesterol and triglycerides). Therefore, we first combined all lipid-related definitions into a single group (any lipid abnormality vs. normal lipids), and then further categorised them into (1) hypercholesterolaemia (yes vs. no), and (2) hyperlipidaemia (yes vs. no). Rigorous physical activity was categorised as (1) ≥3 times a week, and (2) <3 times a week, and BMI as (1) ≥30 kg/m^2^ vs. (2) <30 kg/m^2^. Definitions for the remaining risk factors, hypertension, and diabetes mellitus, were dichotomised as present vs. absent and followed the criteria used in the original publications, consistent with a 2005 meta-analysis on risk factors for aSAH.^5^ Studies using risk factor definitions that could not be harmonised with the above categories, were included in the systematic review, but excluded from the meta-analysis.^6,13-18^ Specifically, 2 studies were excluded from the smoking meta-analysis,^6,13^ 1 study from alcohol use,^17^ 5 from BMI,^13-17^ 1 from hyperlipidaemia,^18^ and 1 from rigorous physical activity^17^ (studies are described in Supplementary Material S5).
Statistical analysis
Pooled proportions of women among participants and UIA cases were calculated using a random effects meta-analysis, accounting for the weighted contribution of each study. We pooled data for each individual risk factor using an inverse variance weighted random effects meta-analysis. Data from case–control and cohort studies were combined. For each risk factor, we used the most adjusted effect estimates available and also included crude estimates if no adjusted estimates were available. We pooled different measures of association and interpreted them as equivalent to odds ratios (ORs).
We quantified heterogeneity between studies using the I^2^ statistic, as proposed by Higgins, and considered I^2^ of 25%–50% as moderate, 50%–75% as substantial, and >75% as considerable heterogeneity.^19^ When more than 10 studies reported on a specific risk factor, potential publication bias was assessed using funnel plots for visual inspection and Egger’s regression tests to statistically evaluate small-study effects. We planned to perform sex-stratified analyses when sufficient data were available. Additionally, we performed subgroup analyses for each risk factor, restricting to studies that reported adjusted effect estimates (ie, those that had adjusted for at least one covariate). All statistical analyses were performed using R statistical software, version 4.0.2.
Results
The systematic search identified a total of 2 969 articles. After title and abstract screening, 53 articles reporting on UIA were evaluated in full-text and of those, a total of 21 studies met the inclusion criteria (Figure 1).^6,8,10,13-18,20-31^ Details of studies excluded after full-text review are provided in Supplementary Material S6. These 21 studies included a total of 347 907 participants (range 132–131,999) and 8 698 UIA cases (range 25–5335). The pooled proportion of women was 55.2% (95% CI, 48.9–61.4) among all participants and 62.8% (95% CI, 58.6–66.8) among UIA cases. The included studies comprised 11 case–control,^6,8,13,14,18,20,22,25,27,28,31^ 7 cross-sectional,^15-17,21,23,26,29^ 2 prospective cohort studies,^10,24^ and 1 retrospective cohort study.^30^ General characteristics of the study populations are summarised in Table 1. The age of participants ranged from 18 to 91 years. Geographically, the studies originated from 13 Asian,^8,13,15,16,18,20-24,26,29,31^ 4 North-American,^14,25,27,28^ and 4 European countries.^6,10,17,30^ Hypertension (n = 20), smoking (n = 18), and diabetes (n = 16) were the most frequently reported risk factors. Alcohol use and lipid abnormalities were assessed in 11 and 13 studies, respectively, while only 2 studies each examined BMI and rigorous physical activity. Eighteen studies included both women and men, while 3 studies were conducted in female-only cohorts.^14,27,28^ One out of these 18 studies provided sex-stratified results, precluding the possibility of assessing sex differences in risk factors for UIA.^8^ This 1 study reported that hypertension and diabetes were similarly and significantly associated with the presence of UIAs in both women and men.
*PRISMA flow diagram depicting study selection The combined search identified 6 962 records, including records for a systematic review and meta-analysis on risk factors for aneurysmal subarachnoid haemorrhage. Abbreviations: UIA = unruptured intracranial aneurysms; aSAH = aneurysmal subarachnoid haemorrhage; PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality assessment
The overall quality of included studies varied (Supplementary Material S7). Two of the 21 studies were scored as having low risk of bias across all 4 assessed domains, 2 were scored as high or unclear risk in 1 domain, and the remaining 17 studies were scored as high or unclear risk in 2 or more of the 4 domains. The most common sources of bias were limited generalizability, often due to use of hospital-based populations, and insufficient adjustment for age as a confounding factor. Funnel plots were produced for smoking, hypertension, diabetes, and any lipid abnormality. Visual assessment of these funnel plots showed no clear asymmetry, and Egger’s regression tests did not indicate small-study effects (all P > .25), together suggesting low risk of publication bias (Supplementary Material S8).
Meta-analysis
Forest plots for each individual risk factor are provided in Supplementary Material S9–S18. A combined forest plot summarising the pooled effect estimates of the assessed risk factors is shown in Figure 2. Hypertension and a history of ever smoking were associated with the presence of UIA, with a pooled OR of 1.72 (95% CI, 1.42–2.09, I^2^ = 82%, 20 studies) for hypertension and a pooled OR of 1.47 (95% CI, 1.11–1.95, I^2^ = 88%, 18 studies) for ever smoking. In subgroup analyses including only studies that adjusted their effect estimates for at least one covariate (mostly sex or age), hypertension (OR 1.92, 95% CI, 1.45–2.54, I^2^ = 76%, 13 studies), and ever smoking (OR 2.28, 95% CI, 1.70–3.06, I^2^ = 68%, 9 studies) remained statistically significantly associated with an increased UIA risk (Supplementary Materials S19 and S20).
Summary of forest plots for each risk factor. Abbreviations: BMI = body mass index; N = number of studies; OR = odds ratio.
No statistically significant associations were found between UIA and diabetes (pooled OR 0.98, 95% CI, 0.83–1.16, I^2^ = 24%, 16 studies), regular alcohol use (pooled OR 0.99, 95% CI, 0.75–1.31, I^2^ = 61%, 6 studies), BMI ≥30 (pooled OR 1.11, 95% CI, 0.85–1.45, I^2^ = 0%, 2 studies), or rigorous physical activity (pooled OR 0.91, 95% CI, 0.44–1.89, I^2^ = 84%, 2 studies). Likewise, any lipid abnormality (combined group of all reported lipid-related abnormalities) (pooled OR 1.19, 95% CI, 0.98–1.45, I^2^ = 55%, 13 studies), or hypercholesterolaemia specifically (pooled OR 1.12, 95% CI, 0.80–1.56, I^2^ = 71%, 7 studies) were not statistically significantly associated with UIA. Subgroup analyses for diabetes and hypercholesterolaemia yielded similar findings (Supplemental Materials S21 and S22).
Discussion
In this systematic review and meta-analysis aimed at identifying risk factors for UIAs, we found that both hypertension and a history of smoking were associated with the presence of UIAs. No statistically significant associations were observed for the other assessed risk factors. Although one of the objectives was to assess sex differences in risk factor associations, this was not feasible, as only one of the 18 studies that included both sexes provided sex-stratified results.^8^ This study reported similar associations between hypertension and diabetes with UIAs in both sexes.
Our meta-analysis provides the most up-to-date and precise estimates of the associations between hypertension, smoking, and the presence of UIAs, confirming these as key modifiable risk factors. Similarly, our recent meta-analysis on risk factors for aSAH, which assessed the same risk factors as our study, identified hypertension and smoking as the most important risk factors for aSAH, along with alcohol consumption.^4^ These findings support the hypothesis that key modifiable risk factors may play roles in both the formation and rupture of intracranial aneurysms. While we found no statistically significant associations between UIAs and other modifiable risk factors, the aSAH meta-analysis additionally reported diabetes and physical activity to be associated with decreased aSAH risk, with inconsistent associations for hypercholesterolaemia and BMI.^4^ Variations in risk factor definitions and the limited numbers of studies for these risk factors may partly explain why these associations were not observed in the context of UIAs. Alternatively, some of these risk factors may primarily influence the risk of aneurysm rupture rather than UIA formation, highlighting potential differences in the risk factor profiles underlying UIA development versus aSAH occurrence.
Due to lack of sex-stratified data in our included studies, as we previously emphasised,^32^ we were unable to assess whether the found associations of hypertension and smoking with UIA differ between women and men. Therefore, we could not assess whether sex differences in the strength of these risk factors’ associations might contribute to the higher burden in women.
In this study, we focused on risk factors that occur in both women and men. However, given the female preponderance in UIA, it is important to also consider the role of female-specific risk factors. In our recent aSAH meta-analysis, no statistically significant associations were found between hormone replacement therapy or oral contraceptive use and aSAH.^4^ As part of the current UIA systematic search, we also screened for studies reporting on these two risk factors, but only one matched case–control study was identified. This study reported ORs of 3.10 (95% CI 1.50-6.20) for hormone replacement therapy use and 2.10 (95% CI 1.20-3.80) for oral contraceptive use, using patients with UIAs as the reference group, suggesting a lower likelihood of UIA among users compared with non-users.^14^ As evidence is limited to this single study, robust conclusions cannot be drawn. Other female-specific risk factors, such as pregnancy-related factors, remain largely unexplored. Further large-scale studies are needed to clarify the role of hormonal and reproductive factors in UIA risk, which may help explain the persistent female preponderance.
A strength of our study is that it included assessments of a wide range of risk factors, encompassing 347 907 participants and 8698 UIA cases. Furthermore, we provided an extensive risk of bias assessment with additional funnel plots to evaluate the quality of the included studies and to assess publication bias, thereby strengthening the interpretation of our findings. Our study also has several limitations. First, we observed considerable heterogeneity across the included studies in terms of study design, population characteristics, and risk factor definitions. Although we standardised risk factor definitions where possible to enable the meta-analysis, the underlying heterogeneity remains a limitation. The variability in definitions of risk factors also necessitated dichotomisation of most risk factors, which limits our ability to assess thresholds of exposure. Secondly, the overall quality of the included studies was limited; with only two of the 21 studies rated as low risk of bias in our quality assessment. This precluded a subgroup analysis based solely on high-quality studies. However, we did perform a sensitivity analysis restricted to studies that adjusted their effect estimates for at least one covariate, which partially addressed potential confounding. Still, substantial heterogeneity remained. This likely reflects both incomplete adjustment for confounding, since a substantial number of studies did not adjust for age and the covariates included in adjustments varied widely, as well as differences in study populations and methodological approaches. Third, we analysed risk factors independently and did not assess their joint or synergistic effects. However, some patients may have had multiple risk factors, and prior research has shown that the combined effect of hypertension and smoking exceeds the sum of their individual risks.^6^ As a result, our independent assessments may underestimate the true effect sizes.
In summary, we reaffirm that hypertension and smoking are associated with the presence of UIAs. These risk factors were previously established as being associated with aneurysm rupture, and our study now also confirms their role in UIA occurrence. These modifiable risk factors should be actively managed in patients at high risk of developing UIAs, as well as in those already diagnosed with a UIA, to potentially reduce the risk of aneurysm formation and rupture. Future research should not only focus on stratifying results by sex, but also on the investigation into female-specific risk factors, such as hormonal and pregnancy-related factors. A deeper understanding of the female predisposition to UIA is essential to optimise both prevention strategies and clinical management.
Standard protocol approvals, registrations, and patient consents
Review board approval and informed consent were not required because this research used only published, deidentified data.
Supplementary Material
Clean_Revised_Supplemental_material_ESJ_aakaf028
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vlak MH, Algra A, Brandenburg R, Rinkel GJE. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10:626-636. 10.1016/S 1474-4422(11)70109-021641282 · doi ↗ · pubmed ↗
- 2Nieuwkamp DJ, Setz LE, Algra A, et al. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 2009;8:635-642. 10.1016/S 1474-4422(09)70126-719501022 · doi ↗ · pubmed ↗
- 3Fréneau M, Baron-Menguy C, Vion AC, et al. Why are women predisposed to intracranial aneurysm? Front Cardiovasc Med. 2022;9:815668. 10.3389/fcvm.2022.815668 · doi ↗
- 4Ali M, van Eldik MJA, Rietkerken S, et al. Risk factors of aneurysmal subarachnoid Hemorrhage including analysis by sex: a systematic review and meta-analysis. Neurology. 2025;104:e 213511. 10.1212/WNL.000000000021351140153684 PMC 11952700 · doi ↗ · pubmed ↗
- 5Feigin VL, Rinkel GJE, Lawes CMM, et al. Risk factors for subarachnoid hemorrhage: an updated systematic review of epidemiological studies. Stroke. 2005;36:2773-2780. 10.1161/01.STR.0000190838.02954.e 816282541 · doi ↗ · pubmed ↗
- 6Vlak MH, Rinkel GJ, Greebe P, et al. Independent risk factors for intracranial aneurysms and their joint effect: a case-control study. Stroke. 2013;44:984-987. 10.1161/STROKEAHA.111.00032923422088 · doi ↗ · pubmed ↗
- 7Gu YX, Chen XC, Song DL, et al. Risk factors for intracranial aneurysm in a Chinese ethnic population. Chin Med J (Engl). 2006;119:1359-1364. 10.1097/00029330-200608020-0000816934182 · doi ↗ · pubmed ↗
- 8Inagawa T . Risk factors for the formation and rupture of intracranial saccular aneurysms in Shimane. Jpn World Neurosurg. 2010;73:155-164. 10.1016/j.surneu.2009.03.007 · doi ↗