Rare case of left anterior descending artery compression
Lina Kapleriene, Dominykas Sudavicius, Diana Zakarkaite, Sigita Glaveckaite

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
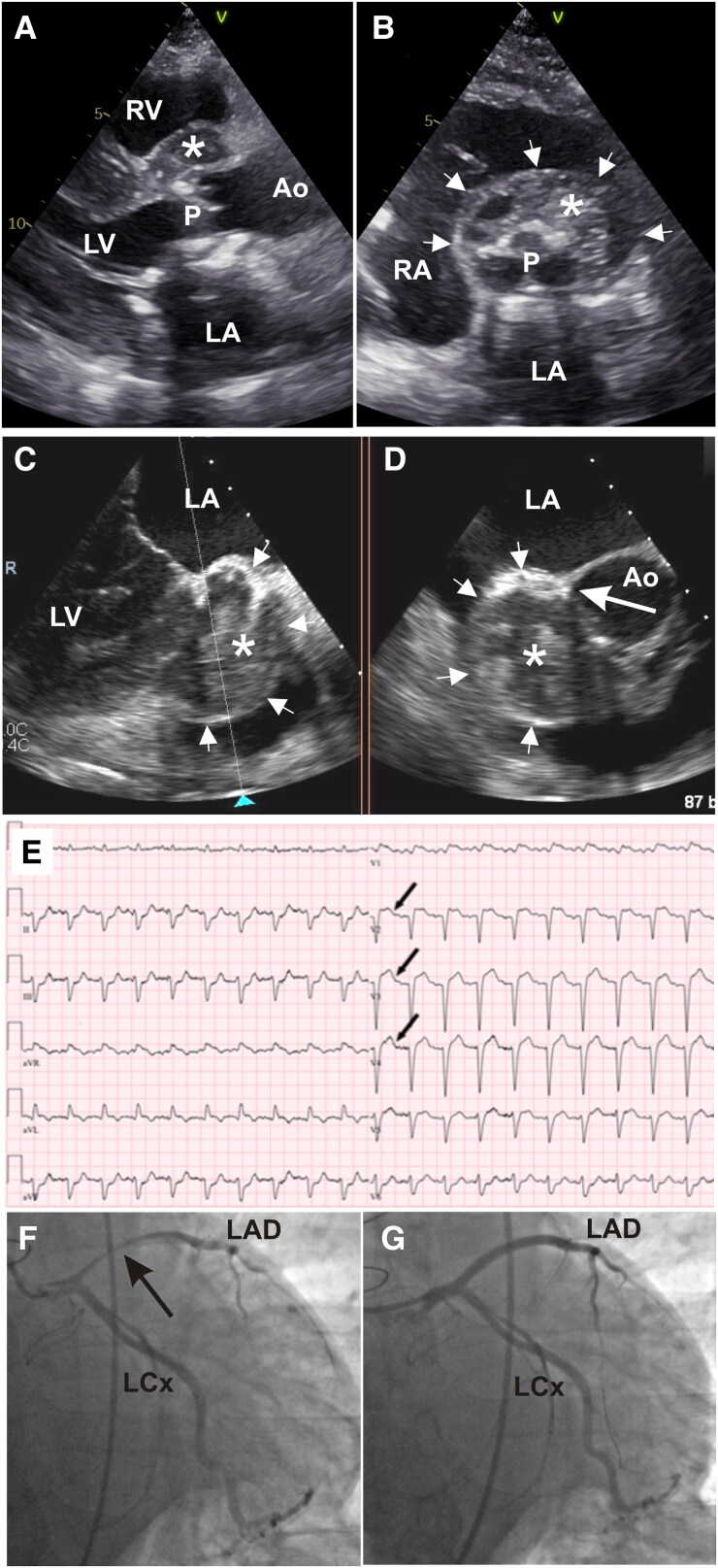 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Intracranial Aneurysms: Treatment and Complications · Vascular Procedures and Complications
Case description
A 64-year-old male patient presented with new-onset chest pain, fever, fatigue, and systolic murmur at the aortic valve (AV) auscultation point. His history revealed a bio-prosthetic AV implantation due to infective endocarditis 6 years ago. Upon admission, the patient was stable with elevated inflammatory biomarkers. Transthoracic echocardiogram showed an aortic root abscess (Figure 1A and B; Supplementary material online, Videos S1 and S2). Aortic valve peak ejection velocity measured at 3.86 m/s and mean pressure gradient at 37.63 mmHg. Transoesophageal echocardiogram showed AV destruction with a mass attached to the right cusp of the bio-prosthetic AV leaning into the left ventricular outflow tract (LVOT) (see Supplementary material online, Video S3) and an encapsulated 4.1 × 3.4 cm aortic root abscess (Figure 1C and D; Supplementary material online, Video S4) likely incorporating the proximal part of the left main coronary artery. Two sets of blood cultures as well as a urine culture were obtained and came back negative. The patient was commenced on intravenous empiric antibiotic therapy of ampicillin, oxacillin, and gentamicin. The patient remained stable and continued undergoing additional pre-surgical evaluations as directed by the cardiac surgeon. However, on the fifth day of hospitalization—just before the planned urgent cardiac surgery—the patient’s haemodynamic condition suddenly deteriorated, and the electrocardiogram showed an acute anterior ST-elevation myocardial infarction (Figure 1E). Emergency coronary angiography revealed high-grade proximal left anterior descending (LAD) artery stenosis due to extrinsic compression (Figure 1F; Supplementary material online, Video S5), in addition to the patient’s significant LVOT stenosis. Despite percutaneous coronary intervention with stenting (Figure 1G; Supplementary material online, Video S6), worsening haemodynamic condition culminated in death. Because the patient was haemodynamically stable, surgery was scheduled on an urgent rather than an emergent basis. However, an earlier surgical intervention might have saved his life. Though a few similar cases that have been described,^1–3^ our case presents a rare and excellent example of multimodality imaging that allows readers to understand the pathophysiology of external coronary artery compression caused by an aortic root abscess.
Transthoracic echocardiogram parasternal long-axis (A) and short-axis (B) views with an asterisk representing the abscess and arrows marking its borders. Transoesophageal echocardiogram two-chamber view (C) and a view perpendicular to the former (D) show the abscess (asterisk) and its boundaries (small arrows). The left coronary artery’s ostium is indicated by the big arrow (D). Electrocardiogram showing ST elevations in leads V1–V5 (E). Coronary angiogram indicating left anterior descending narrowing before (F, arrow) and after stenting (G). Ao, aorta; LA, left atrium; LCx, left circumflex artery; LV, left ventricle; P, aortic valve prosthesis; RA, right atrium; RV, right ventricle.
Supplementary Material
ytag018_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Joy G, Lewis M, Furniss S. Acute coronary syndrome caused by extrinsic coronary compression from an aortic root abscess in a patient with mechanical aortic valve endocarditis: a case report and literature review. Eur Heart J Case Rep 2020;5:ytaa 483.33554020 10.1093/ehjcr/ytaa 483PMC 7850617 · doi ↗ · pubmed ↗
- 2Roux V, Salaun E, Tribouilloy C, Hubert S, Bohbot Y, Casalta JP, et al Coronary events complicating infective endocarditis. Heart 2017;103:1906–1910.28642290 10.1136/heartjnl-2017-311624 · doi ↗ · pubmed ↗
- 3Manzano MC, Vilacosta I, San Román JA, Aragoncillo P, Sarriá C, López D, et al Acute coronary syndrome in infective endocarditis. Rev Esp Cardiol 2007;60:24–31.17288952 · pubmed ↗