Distal coronary sinus–left atrial fistulous communication uncovered during atrial fibrillation ablation
Yoshihiro Sobue, Tomoyuki Ohno, Eiichi Watanabe, Hideo Izawa

TL;DR
A rare anatomical connection between the distal coronary sinus and left atrium was discovered during heart ablation for atrial fibrillation, emphasizing the importance of detailed imaging.
Contribution
This case reports a previously uncommon distal coronary sinus-left atrial fistula involving the left atrial appendage and pulmonary vein.
Findings
A fistulous tract was identified between the distal coronary sinus, left atrial appendage, and left inferior pulmonary vein.
Multimodality imaging confirmed the anatomical connection pre- and post-procedure.
The anomaly was safely managed during ablation without complications.
Abstract
Congenital anomalies of the coronary sinus (CS) are rare and often overlooked on standard imaging. Among these, the unroofed coronary sinus (URCS) is the most recognized, typically involving the proximal CS and frequently associated with a persistent left superior vena cava. In contrast, fistulous communications between the distal CS and the left atrium (LA) are exceptionally uncommon. Their recognition is important during atrial fibrillation (AF) ablation, where unanticipated channels may complicate catheter manipulation and lesion delivery. A 76-year-old woman with recurrent paroxysmal AF underwent catheter ablation. A lumen-equipped multipolar catheter was positioned in the CS, and transseptal access to the LA was achieved. During electroanatomical mapping with a high-density catheter, entanglement with the CS catheter suggested an anomalous connection. Contrast injection through…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
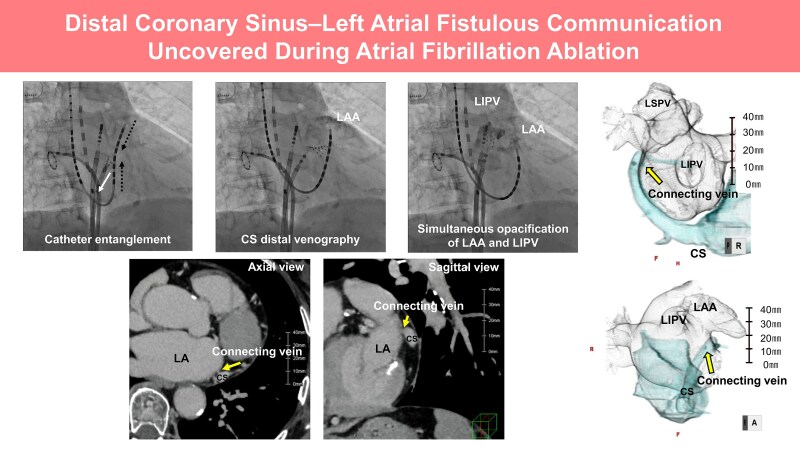 Figure 1
Figure 1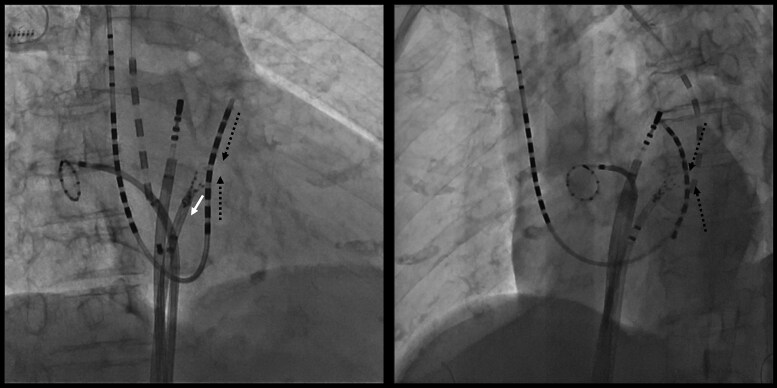 Figure 1
Figure 1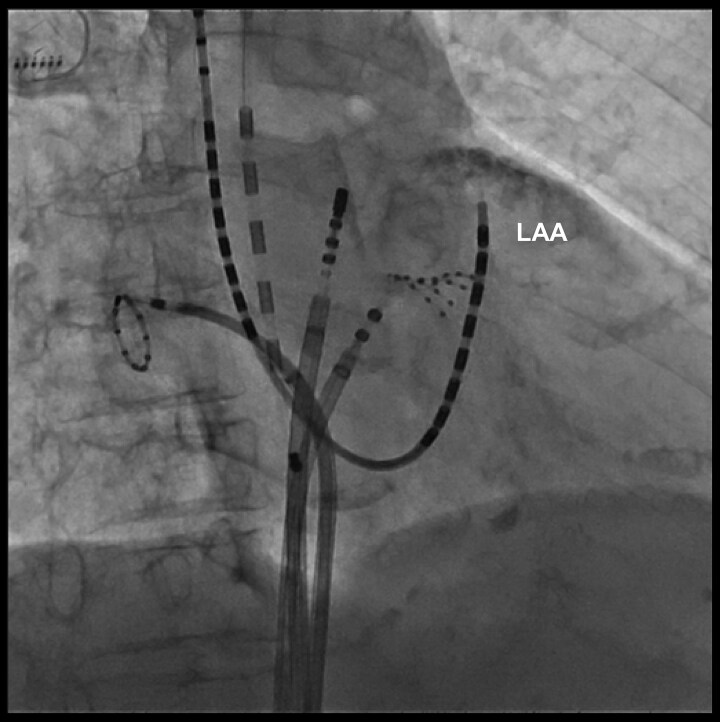 Figure 2
Figure 2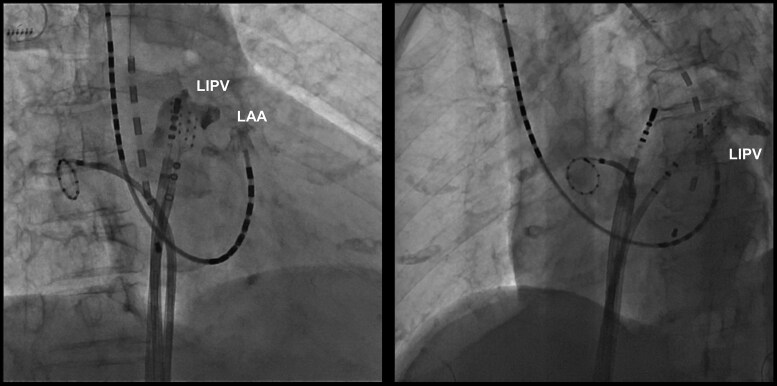 Figure 3
Figure 3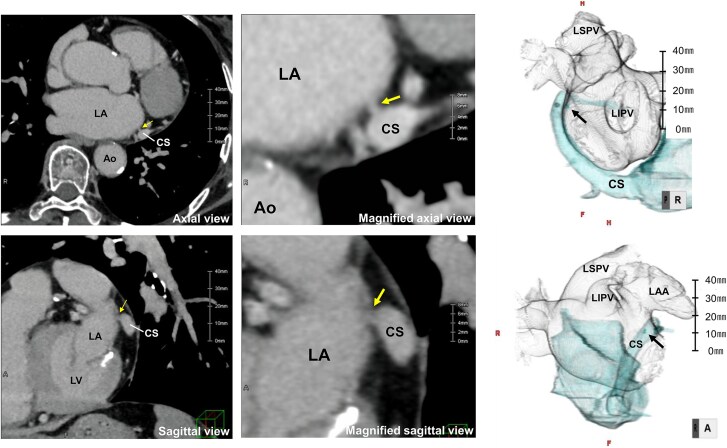 Figure 4
Figure 4| Type | Complete or partial defect | Defect site of CS | With PLSVC | Without PLSVC |
|---|---|---|---|---|
| I | Complete | – | Ia | Ⅰb |
| Ⅱ | Partial | Proximal | Ⅱa | Ⅱb |
| Ⅲ | Partial | Distal | Ⅲa | Ⅲb |
| Ⅳ | Partial | Connecting vein | Ⅳa | Ⅳb |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Coronary Artery Anomalies · Cardiac Arrhythmias and Treatments
Introduction
The coronary sinus (CS) originates embryologically from the left horn of the sinus venosus.^1^ In normal anatomy, the CS courses along the posterior atrioventricular groove and drains into the right atrium through a discrete ostium located between the inferior vena cava and the tricuspid annulus.
Congenital anomalies of the CS are uncommon, with an estimated prevalence of approximately 0.1%–1.0% in the general population.^1^ Reported variants include persistent left superior vena cava (PLSVC), unroofed coronary sinus (URCS), coronary sinus ostial atresia, and CS diverticulum. Unroofed coronary sinus represents the rarest form of atrial septal defect, characterized by partial or complete absence of the CS wall, usually involving its proximal segment and frequently associated with PLSVC.^2–4^ Although URCS represents the most common congenital anomaly associated with communication between the proximal CS and the left atrium (LA), fistulous connections arising from the distal CS to the LA remain little known and poorly characterized. Herein, we describe a rare and anatomically distinctive case of a distal CS fistulous connection with both the left atrial appendage (LAA) and the left inferior pulmonary vein (LIPV), identified incidentally during catheter ablation for atrial fibrillation (AF).
Summary figure
Distal CS–left atrial fistulous communication identified during atrial fibrillation ablation. Coronary sinus distal venography showed opacification of the LAA with simultaneous LIPV filling, and CT (axial and sagittal views) confirmed the connecting vein.
Case presentation
A 76-year-old woman with recurrent, symptomatic paroxysmal atrial fibrillation presented with palpitations. Transthoracic echocardiography showed a preserved left ventricular ejection fraction (62%) and a mildly enlarged LA (diameter 37 mm; volume index 44.8 mL/m²). She was admitted for catheter ablation. After venous access was obtained, a lumen-equipped multipolar catheter (BeeAT, Japan Lifeline, Tokyo, Japan) was introduced into the CS for reference and pacing. Subsequently, a transseptal puncture was performed under fluoroscopic and electroanatomical guidance. Thereafter, an anatomical and activation map of the LA was systematically acquired using a high-density multipolar mapping catheter (Advisor™ HD Grid, Abbott, Abbott Park, IL, USA).
During the mapping procedure, mechanical entanglement occurred between the HD Grid catheter in the LA and the BeeAT catheter positioned in the distal CS (Figure 1; Supplementary material online, VideoS1). This raised suspicion of an anomalous communication between the CS and the LA. To confirm this suspicion, contrast medium was injected through the lumen of the BeeAT catheter, opacifying the LAA and demonstrating a fistulous tract (Figure 2;Supplementary material online, Video S2). For precise delineation of the fistulous site, the CS catheter was repositioned more proximally and selective contrast injection was repeated. This demonstrated simultaneous opacification of the LAA and the LIPV (Figure 3;Supplementary material online, Video S3), thereby establishing the presence of a fistulous communication between the distal CS, the LAA, and the LIPV.
Mechanical entanglement of an HD Grid catheter in the left atrium with a lumen-equipped BeeAT catheter in the distal coronary sinus during mapping. The white arrow indicates the direction of traction applied by the HD Grid catheter, while the black dotted line denotes the resulting force vector pulling the coronary sinus catheter electrodes.
Contrast injection through the distal coronary sinus lumen opacifying the left atrial appendage, indicating a fistulous tract.
Selective coronary sinus angiography demonstrating simultaneous opacification of the left atrial appendage and the left inferior pulmonary vein.
Electrical isolation of all four pulmonary veins was successfully achieved, and the procedure was completed without complications. Isoproterenol infusion and programmed pacing from both the distal and proximal CS were performed to assess arrhythmogenicity; however, AF was not inducible. Therefore, no ablation was applied to the connecting vein or the CS. At 8-month follow-up, the patient remained in sinus rhythm without AF recurrence. Oral anticoagulation was continued based on a CHA₂DS₂-VASc score of 2. Because the distal CS–LA communication was small, haemodynamically insignificant, and non-arrhythmogenic, no intervention was performed and conservative follow-up was chosen.
Cardiac CT was performed using a 320-detector row scanner (Aquilion ONE, Canon Medical Systems, Japan) with a slice thickness of 0.5 mm during the contrast-enhanced left atrial phase and the delayed phase (90 s after contrast injection). The CT images shown correspond to the delayed phase, which best delineated the fistulous communication. Retrospective review of the pre-procedural contrast-enhanced computed tomography images, which had initially been interpreted as normal, revealed subtle contrast continuity between the CS at the level of the mitral annulus (approximately 1 o’clock in the left anterior oblique projection) and the adjacent left atrial wall, corroborating the intra-procedural diagnosis (Figure 4).
Computed tomography images including axial, magnified axial, sagittal, and magnified sagittal views, as well as a 3D reconstruction, demonstrating a connecting vein arising from the distal coronary sinus and entering the left atrium at the left atrial appendage–left inferior pulmonary vein ridge. Yellow arrows indicate the connecting vein on CT images, and the black arrow highlights the same structure on the 3D reconstruction. Scale bars are shown for reference. LA, left atrium; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; CS, coronary sinus; Ao, aorta; LV, left ventricle.
Discussion
We reported a rare distal CS–LA communication uncovered during AF ablation, with the fistulous tract coursing between the LAA and the LIPV. As previous case reports of CS–LA fistulas have predominantly described defects arising from the proximal or mid CS,^5^ communications originating from the distal CS to the LA remain little known and poorly characterized.^6^ From an embryological perspective, these anomalies may be caused by either a distal variant within the spectrum of URCS or, alternatively, a form of partial anomalous pulmonary venous connection draining into the CS.^7^ Recognition of these variants is clinically important, not only for accurate anatomical classification but also because fistulous channels may alter local conduction properties, serve as potential triggers for atrial fibrillation, and complicate catheter manipulation.
Unroofed coronary sinus is a rare congenital anomaly defined by partial or complete absence of the partition between the CS and LA. Based on the extent of unroofing and the presence or absence of a PLSVC, four morphological types with subtypes ‘a’ (with PLSVC) and ‘b’ (without PLSVC) are recognized (Table 1).^3^ In the present case, we identified a distal CS–LA communication located at the LAA/LIPV ridge in the absence of an atrial septal defect or a PLSVC. Morphologically, this anomaly corresponds to type IVb in the contemporary URCS classification, defined as an anomalous conduit between the CS and the LA without PLSVC. Although proximal CS–LA communications have been reported,^5,8^ a distal fistulous tract has not previously been demonstrated using both high-resolution 3D mapping and contrast venography. This case therefore represents the first documented distal type IVb URCS, with a connection from the distal CS to the LAA–LIPV ridge.
The connecting vein arose from the distal CS and entered the LA at the LAA–LIPV ridge. Although the vein of Marshall typically drains into the proximal to mid CS,^9,10^ the course of this channel overlapped its expected trajectory, suggesting an embryologically related but distinct vestigial variant with a persistent atrial opening. This region can be arrhythmogenic, but no spontaneous or inducible triggers were observed.
Small or incidentally detected URCS variants are generally managed conservatively, with intervention reserved for cases involving significant shunting or associated congenital anomalies. In this patient, the absence of haemodynamic impact or arrhythmogenic substrate justified conservative management with continued anticoagulation based on the CHA₂DS₂-VASc score. Their identification carries important procedural implications, underscoring the need for meticulous imaging and intra-procedural assessment to ensure safe and effective ablation strategies.
Conclusion
Distal CS–LA fistulous connections represent an exceedingly rare venous anomaly that may reflect either a distal variant of URCS or an embryologic remnant of the VOM. Recognition of these variants is of clinical importance, as their presence has direct implications for safe catheter manipulation and procedural planning and therapeutic strategies in left atrial interventions.
Lead author biography
Dr Yoshihiro Sobue is a cardiologist and electrophysiologist at Fujita Health University Bantane Hospital, Nagoya, Japan. He received his MD and PhD from Fujita Health University and has specialized training in cardiac electrophysiology and catheter ablation. His clinical and research interests focus on atrial fibrillation, ventricular arrhythmias, heart failure, and advanced mapping/imaging technologies. He has published widely in peer-reviewed journals and actively contributes as a reviewer and editorial board member for international cardiovascular journals.
Supplementary Material
ytag030_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Azizova A, Onder O, Arslan S, Ardali S, Hazirolan T. Persistent left superior vena cava: clinical importance and differential diagnoses. Insights Imaging 2020;11:110.33057803 10.1186/s 13244-020-00906-2PMC 7561662 · doi ↗ · pubmed ↗
- 2Bonardi M, Valentini A, Camporotondo R. Unroofed coronary sinus with persistent left superior vena cava: a case report. J Ultrasound 2012;15:179–182.23450671 10.1016/j.jus.2012.06.001PMC 3558062 · doi ↗ · pubmed ↗
- 3Ma J, Zheng Y, Xu S, Teng H, Lv L, Li Y, et al The value of cardiac CT in the diagnosis of unroofed coronary sinus syndrome. BMC Cardiovasc Disord 2022;22:516.36460953 10.1186/s 12872-022-02966-2PMC 9716674 · doi ↗ · pubmed ↗
- 4Zhi AH, Dai RP, Ma WG, Zhang P, Lv B, Jiang SL. CT angiography for diagnosis and subcategorization of unroofed coronary sinus syndrome. J Thorac Dis 2017;9:3946–3955.29268405 10.21037/jtd.2017.09.03PMC 5723801 · doi ↗ · pubmed ↗
- 5Abazid RM, Goha A, Romsa JG, Warrington JC, Akincioglu C, Stodilka RZ, et al Coronary sinus to left atrium fistula on computed tomography angiography: differentiation from unroofed coronary sinus with literature review. J Cardiovasc Comput Tomogr 2021;15:e 15–e 17.33229304 10.1016/j.jcct.2020.11.003 · doi ↗ · pubmed ↗
- 6Ootaki Y, Yamaguchi M, Yoshimura N, Oka S, Yoshida M, Hasegawa T. Unroofed coronary sinus: diagnosis, classification, and surgical treatment. J Thorac Cardiovasc Surg 2003;126:1655–1656.14666054 10.1016/s 0022-5223(03)01019-5 · doi ↗ · pubmed ↗
- 7Anderson RH, Brown NA, Moorman AF. Development and structures of the venous pole of the heart. Dev Dyn 2006;235:2–9.16193508 10.1002/dvdy.20578 · doi ↗ · pubmed ↗
- 8Shafter AM, Almeida SO, Syed U, Shaikh K, Budoff MJ. Anomalous coronary sinus communication to the left atrium. J Cardiol Cases 2019;20:122–124.31969939 10.1016/j.jccase.2019.06.007PMC 6962757 · doi ↗ · pubmed ↗