Long‐Term Effect of Macrolides on Helicobacter pylori Eradication: Data From the European Registry on Helicobacter pylori Management (Hp‐EuReg)
Olga P. Nyssen, Guillermo J. Ortega, Laimas Jonaitis, Ángeles Pérez‐Aísa, Bojan Tepes, Alfredo J. Lucendo, Javier Tejedor‐Tejada, Renate Bumane, Ana Garre, Jose M. Huguet, Monica Perona, Óscar Núñez, Manuel Pabón‐Carrasco, Manuel Castro‐Fernández, Miguel Areia, Jesús Barrio

TL;DR
High use of macrolide antibiotics in the population reduces the success of Helicobacter pylori treatment, especially when used within the last few years.
Contribution
This study shows that population-level macrolide consumption significantly impacts H. pylori eradication success in treatment-naïve patients.
Findings
Higher macrolide consumption in the general population is linked to lower eradication rates of H. pylori.
Clarithromycin-based therapies become less effective as population-level macrolide use increases.
The strongest negative impact of prior macrolide use is observed within 5 years before treatment.
Abstract
Previous antibiotic use influences Helicobacter pylori antibiotic resistance. This study evaluated how prior population‐level macrolide (especially clarithromycin) use affects H. pylori eradication success in naïve patients. Retrospective, multicenter, ecological study. Multivariate logistic regression was performed with modified intention‐to‐treat effectiveness as the main outcome. Key variables included first‐line clarithromycin‐based treatments, therapy duration (7, 10, 14 days), proton pump inhibitor dose (low, standard, high), compliance (> 90%), and clarithromycin consumption (defined daily doses/1000 inhabitants/day, from the European Surveillance of Antimicrobial Consumption Network). Nested hierarchical models incorporated macrolide consumption, matched by year and country, and assessed the interaction between consumption and first‐line empirical treatments from the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
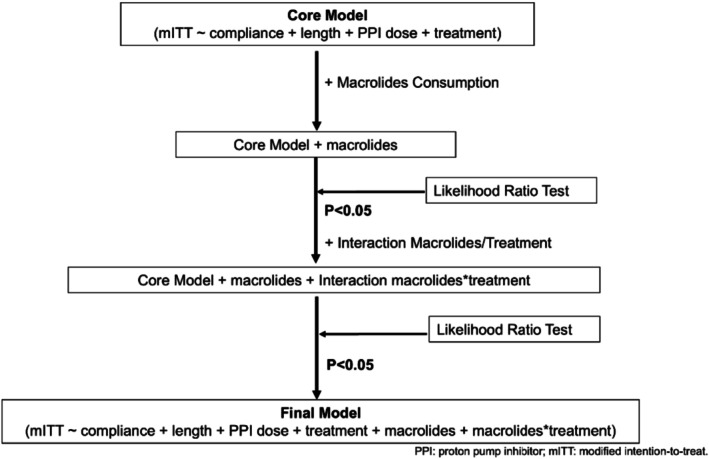 FIGURE 1
FIGURE 1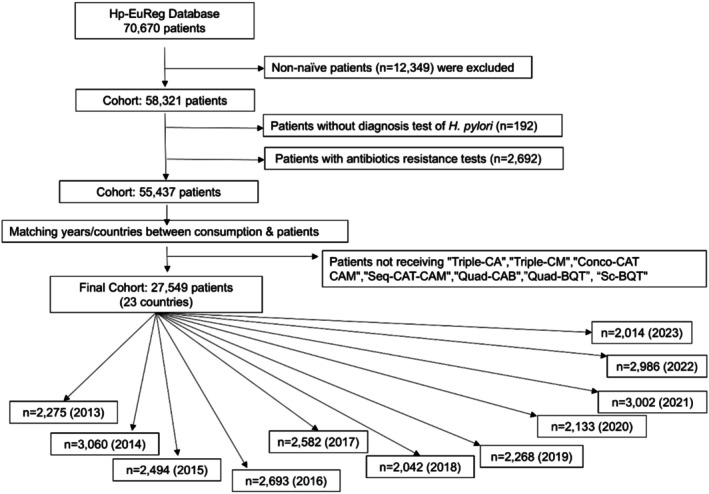 FIGURE 2
FIGURE 2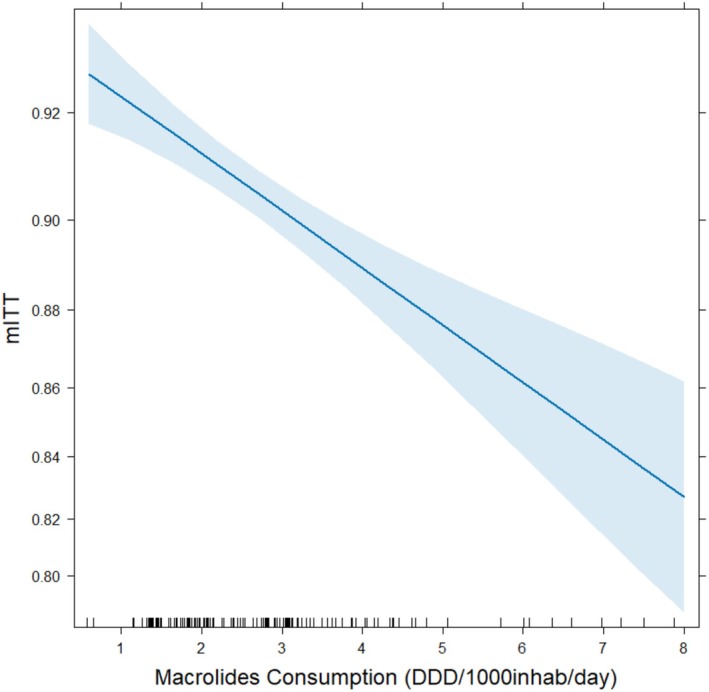 FIGURE 3
FIGURE 3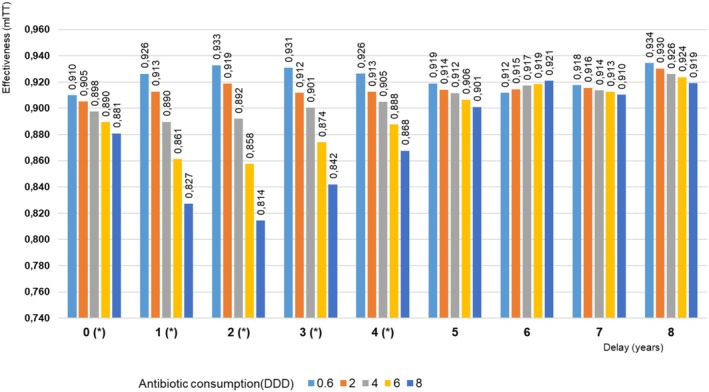 FIGURE 4
FIGURE 4| OR | 2.50% | 97.50% |
| |
|---|---|---|---|---|
| (Intercept) | 1.8039 | 1.1194 | 2.9039 | 1.53E‐02* |
| Compliance | 8.8386 | 6.9731 | 11.1915 | 5.32E‐73*** |
| Length10 days | 0.7564 | 0.6377 | 0.8957 | 1.28E‐03** |
| Length14 days | 0.8715 | 0.7288 | 1.0404 | 1.30E‐01 |
| Standard‐dose PPI | 1.7664 | 1.5519 | 2.0150 | 1.32E‐17*** |
| High‐dose PPI | 2.0250 | 1.8153 | 2.2608 | 2.01E‐36*** |
| Triple‐CA | 0.5869 | 0.3800 | 0.9070 | 1.63E‐02* |
| Triple‐CM | 0.8806 | 0.4166 | 1.8697 | 7.40E‐01 |
| Conco‐CAT CAM | 0.5119 | 0.3238 | 0.8083 | 4.11E‐03** |
| Seq‐CAT‐CAM | 0.8371 | 0.3140 | 2.2303 | 7.22E‐01 |
| Quadruple‐CAB | 2.0910 | 0.5973 | 7.6683 | 2.56E‐01 |
| Macrolides | 0.9604 | 0.8419 | 1.0991 | 5.52E‐01 |
| Triple‐CA:Macrolides | 0.7990 | 0.6836 | 0.9318 | 4.50E‐03** |
| Triple‐CM:Macrolides | 0.4921 | 0.3558 | 0.6801 | 1.69E‐05*** |
| Conco‐CAT CAM:Macrolides | 1.0648 | 0.9083 | 1.2476 | 4.38E‐01 |
| Seq‐CAT‐CAM:Macrolides | 0.9517 | 0.7354 | 1.2345 | 7.08E‐01 |
| Quad‐CAB:Macrolides | 0.5561 | 0.3471 | 0.8856 | 1.39E‐02* |
| Signif. codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘ ’ 0.1 ‘ ’ 1 | ||||
|
|
|
|
| Years | |
|---|---|---|---|---|---|
| Same year | 0.07294 | 1.848e‐14 | 25,525 | 23 | 10 |
| 1 year‐delay | 3.843e‐07 | 1.155e‐13 | 23,131 | 21 | 9 |
| 2 year‐delay | 1.782e‐08 | 8.944e‐16 | 19,935 | 19 | 8 |
| 3 year‐delay | 7.271e‐06 | 2.103e‐09 | 17,381 | 16 | 7 |
| 4 year‐delay | 0.002985 | 1.008e‐08 | 14,683 | 16 | 6 |
| 5 year‐delay | 0.3623 | 2.2e‐16 | 12,106 | 16 | 5 |
| 6 year‐delay | 0.6422 | 2.209e‐14 | 9992 | 16 | 4 |
| 7 year‐delay | 0.7378 | 3.058e‐05 | 7882 | 15 | 3 |
| 8 year‐delay | 0.4899 | 6.207e‐05 | 5850 | 16 | 2 |
| Years of delay | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| Triple‐CA:Macrolides | 0.65 | 0.80 | NS | NS | 0.76 | 0.61 | 0.56 | 0.72 | 0.63 |
| Triple‐CM:Macrolides | 0.35 | 0.50 | 0.51 | 0.55 | NS | 0.60 | 0.57 | NS | NS |
| Conco‐CAT CAM:Macrolides | NS | NS | 1.25 | 1.18 | NS | NS | NS | NS | NS |
| Seq‐CAT‐CAM:Macrolides | 0.78 | NS | NS | NS | NS | 1.18 | NS | NS | NS |
| Quad‐CAB:Macrolides | NS | 0.56 | 0.53 | NS | NS | 6.44 | NS | 88,000 | 0.009 |
- —HORIZON EUROPE Health10.13039/100018696
- —UK Research and Innovation10.13039/100014013
- —EU4Health10.13039/100032850
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastroesophageal reflux and treatments · Pathogenesis and Treatment of Hiccups
Introduction
1
Helicobacter pylori ( H. pylori ) infects over 40% of the global population [1], causing symptoms or disease in 10% of the cases, potentially impacting 800 million people [2]. It commonly leads to dyspepsia but can also cause severe conditions like gastric cancer [3, 4, 5].
Helicobacter pylori ( H. pylori ) infection is challenging due to limited effective antibiotics and rising resistance. Commonly used clarithromycin‐based therapies [6] lose efficacy when resistance exceeds 15%, as shown in several studies, particularly when empirical (non–susceptibility‐based) therapies are used [7, 8, 9]. Based on these data, current guidelines discourage its use beyond this threshold [4, 5], and clarithromycin should only be administered as a susceptibility‐based therapy.
Rational antibiotic use is crucial in preventing microbial resistance [10], and a clear relationship exists between antibiotic consumption and H. pylori resistance [11, 12, 13, 14, 15, 16, 17]. However, it remains unclear whether prior antibiotic use in the general population impacts the effectiveness of H. pylori eradication treatments.
In this ecological study, our objective was to analyze the relationship between the population level of antibiotic consumption (by year and country) in Europe and the effectiveness of eradication treatments in individual treatment‐naïve patients infected with H. pylori .
Methods
2
Antibiotic consumption data were obtained from the European Centre for Disease Prevention and Control (ECDC) through the European Surveillance of Antimicrobial Consumption Network (ESAC‐Net), which tracks antibiotic use (J01 group of the anatomic therapeutic chemical (ATC) classification) [10] in the community and hospitals. Antibiotic use is measured in daily dose (DDD) per 1000 inhabitants per day (DID) [18]. These data exclude antibiotic use in animal husbandry and fish culture.
Helicobacter pylori ( H. pylori ) treatment efficacy data for naïve patients were sourced from Hp‐EuReg. Hp‐EuReg is a multicenter, non‐interventional registry (38 countries) started in 2013 by the European Helicobacter and Microbiota Study Group (www.helicobacter.org) [6, 18]. The study follows ethical guidelines, was approved by the Hospital Universitario de La Princesa Ethics Committee, and is registered on ClinicalTrials.gov (NCT02328131). Further information is detailed in the published protocol [19].
Data Management
2.1
Hp‐EuReg data were recorded in an Electronic Case Report Form (e‐CRF) at REDCap hosted at “Asociación Española de Gastroenterología” (AEG; www.aegastro.es) [20, 21], anonymized, and included first‐line treatments registered between June 2013 and June 2023. Written informed consent was obtained from all participants. The data set was restricted up to 2022 to align with ESAC‐Net records.
After data extraction, the Hp‐EuReg data were quality‐reviewed and discordances were resolved by querying the investigators.
The data collection from the ESAC‐Net database was evaluated for validity using a checklist addressing various biases, including coverage bias in census data, sampling bias in sample data, unaccounted over‐the‐counter sales in reimbursement data, issues with parallel trade or inadequate registration of non‐reimbursed antibiotics, and shifts in antibiotic use between ambulatory and hospital care. To ensure comparability, results were standardized as Defined Daily Doses (DDD) per 1000 inhabitants per day (DID), with population estimates based on mid‐year figures from the WHO European Health for All database [22]. A comprehensive methodology description, including data provider details and discussions on validity, is available in a separate publication [23].
Variable Categorization and Definitions
2.2
To enhance data interpretation, variables were categorized. Proton pump inhibitor (PPI) doses were standardized to omeprazole equivalents and grouped as low‐dose (4.5–27 mg of omeprazole equivalents given twice a day), standard‐dose (32–40 mg of omeprazole equivalents given twice a day), and high‐dose (54–128 mg of omeprazole equivalents given twice a day) [24, 25].
Treatment durations were classified as 7, 10, or 14 days. Compliance was defined as ≥ 90% of medication taken. Only empirically treated patients were included. Seven treatment regimens were analyzed. Those including macrolides were: Triple‐CA (PPI, clarithromycin, amoxicillin); Triple‐CM (PPI, clarithromycin, metronidazole); Seq‐CAT‐CAM and Conco‐CAT‐CAM (PPI, clarithromycin, amoxicillin, metronidazole or tinidazole); Quad‐CAB (PPI, clarithromycin, amoxicillin, bismuth). Regimens without macrolides were: BQT (PPI, metronidazole or tinidazole, tetracycline, and bismuth) and Sc‐BQT (PPI, metronidazole, tetracycline, and bismuth prescribed as a three‐in‐one single capsule).
Effectiveness was evaluated using a modified intention‐to‐treat (mITT) analysis, including all patients empirically treated (not receiving a susceptibility‐guided antibiotic prescription) who completed follow‐up. H. pylori eradication was confirmed ≥ 4 weeks post‐treatment using urea breath test, stool antigen, or histology.
Data Analysis
2.3
A logistic regression model was initially constructed to assess the effectiveness of different H. pylori eradication treatments. The explanatory variables included compliance (Yes/No), treatment duration (7, 10, or 14 days), PPI dose (low, standard, or high), and treatment type (seven categories: Triple‐CA, Triple‐CM, Conco‐CAT‐CAM, Seq‐CAT‐CAM, Quad‐CAB, BQT, and Sc‐BQT). The outcome variable was treatment success or failure based on the mITT analysis. BQT and Sc‐BQT, which do not contain macrolides, were used as the reference category for treatment comparison.
To refine the model, an Akaike step‐backward selection was performed, but none of the variables could be removed without compromising model performance. The Akaike Information Criterion (AIC) was used to balance model fit and complexity, with lower AIC values indicating better optimization.
To evaluate the potential ecological association between community‐level macrolide consumption and clarithromycin‐based treatment effectiveness, macrolide consumption data (mean: 2.77; range: 0.58–7.88) were incorporated in the regression model. A country‐ and year‐matched approach was applied to align macrolide consumption values with patient treatments. The analysis explored whether past macrolide consumption influenced treatment outcomes using three approaches:
- Annual consumption data from previous years (1–10 years before treatment, covering 2013–2022).
- Cumulative consumption over 1–10 years (2013–2022).
- Average macrolide consumption during the same period (2013–2022).
A delay of zero years was applied for patients who received treatment in the same year as macrolide consumption, regardless of whether the antibiotics were taken before or after treatment.
To assess the interaction between macrolide consumption and clarithromycin‐based treatments, an interaction term was included in the regression model. This interaction was evaluated through the ratio of two odds ratios (OR). The first OR compared clarithromycin‐based treatments to non‐clarithromycin‐based treatments at a given value of macrolide consumption, a continuous variable. The second OR examined the same comparison but with macrolide consumption increased by one unit. The resulting ratio, usually referred to as the OR of the interaction, indicated whether macrolide consumption influenced treatment effectiveness; an OR less than one suggests that increased macrolide consumption is associated with reduced effectiveness of clarithromycin‐based treatments, indicating a potential negative impact. Conversely, an OR greater than one implies a potentiation effect, where higher macrolide consumption may enhance the effectiveness of these treatments.
Model improvement was evaluated using the likelihood ratio test (LRT), which compared nested models to determine whether additional predictors significantly enhanced the model fit. The first step involved adding macrolide consumption to the core model, followed by evaluating its impact with the LRT. If this addition improved the model, an interaction term was subsequently introduced, and its significance was also tested again with LRT (Figure 1).
Hierarchical models. The flow chart depicts the construction of three models used in this study: the core model, the model with macrolide consumption, and the model with macrolide consumption–treatment interaction. mITT, modified intention‐to‐treat effectiveness; PPI, proton pump inhibitor.
Qualitative variables were reported as relative frequencies, expressed as percentages with 95% confidence intervals (CIs). Statistical significance was defined as p < 0.05. All analyses were conducted using R version 4.1.2, with custom scripts and base functions from the R programming environment (http://www.R‐project.org; the R Foundation for Statistical Computing, Vienna, Austria) [26].
Results
3
A subset of 58,321 treatment‐naïve patients was first selected from the original Hp‐EuReg database (70,670 patients enrolled between 2013 and 2023). From this group, a further refined subsample of 27,549 patients was chosen for analysis based on their treatment regimen. Patients included in the final analysis had received one of the following seven first‐line eradication treatments: Triple‐CA, Triple‐CM, Conco‐CAT‐CAM, Seq‐CAT‐CAM, Quad‐CAB, BQT, and Sc‐BQT (Figure 2). These patients were recruited from 23 European countries, with the highest number of participants coming from Spain (n = 16,517), followed by Italy (n = 3247), and Slovenia (n = 2889). The patient distribution across the remaining countries covered Western, Northern, Southern, Central, and Eastern Europe, as well as the Baltic region.
Flow chart of patient selection. A, amoxicillin; B, bismuth; BQT: Bismuth quadruple therapy prescribed with metronidazole, tetracycline and bismuth administered separately; C, clarithromycin; M, metronidazole; n, number of treatment‐naïve patients prescribed with an empirical therapy; Sc‐BQT, bismuth quadruple therapy prescribed with metronidazole, tetracycline and bismuth all administered in a single capsule (Pylera); T, tinidazole; PPI, proton pump inhibitor.
Global Effect of Macrolide Consumption on Treatment Effectiveness
3.1
The impact of macrolide consumption on treatment effectiveness was analyzed by adding this variable as covariate in the core model. Model performance improved significantly when macrolide consumption was introduced (LRT p = 3.84 × 10^−7^). The analysis of 23,131 patients across 21 countries revealed that clarithromycin‐based treatments became less effective with increased macrolide consumption in the previous year (Figure 3). The effect of macrolides was a reduction of treatment effectiveness of 13%.
Effect on the modified intention‐to‐treat effectiveness of macrolide community consumption a year before clarithromycin‐based treatment. DDD, defined daily dose (expressed as number/1000 inhabitants/day); mITT, modified intention to treat effectiveness.
We analyzed the effect of macrolide consumption on mITT effectiveness at different time delays before treatment (Figure 4). For each added year of delay, marginal effects were assessed at five macrolide consumption values. The core models with and without this variable were compared by LRT. Effectiveness decline was most pronounced within the first 2 years after consumption, peaking at 3 years before beginning to recover at four‐ and five‐year delays.
*Effect of macrolide community consumption on clarithromycin‐based treatment effectiveness for different delay periods between consumption and treatment. Different consumption levels (0.6, 2, 4, 6, 8 DDD/1000 inhabitants/day) are color‐coded. The x‐axis represents delay times between consumption and treatment year. Treatment effectiveness by modified intention to treat (mITT) was analyzed. Significant model improvement with a likelihood ratio test (LRT), p < 0.05. DDD, defined daily dose.
When countries with the highest number of reported cases were excluded—Spain alone (59%); Spain and Italy (72%); or Spain, Italy, and Slovenia (82%) (Figure S1)—the overall pattern did not change substantially. However, across all three sensitivity analyses, a negative association between antibiotic consumption and resistance emerged during the first 3 years, in contrast to the global model where the resistance peak appeared after a two‐year lag. Moreover, a shift in treatment efficacy was observed toward the fourth year. Notably, for the entire series from 0 to 8 years, the model excluding Spain (the country with the highest number of cases) alone consistently converged—that is, it consistently supported the inclusion of macrolide use—whereas the original model ceased to converge from the fifth year onward. Similar results were obtained when excluding patients from Spain and Italy, or from Spain, Italy, and Slovenia.
Interactions Between Macrolide Consumption and Treatments
3.2
To further assess the impact of macrolide consumption on mITT effectiveness, an interaction term between macrolide consumption and treatment was added to the core model (Figure 1). LRT analysis confirmed that including these terms improved model fit across all time delays (Table 1). For one‐year delay, the treatments most affected were Triple‐CA (OR: 0.80, p: 4.5 × 10^−3^), Triple‐CM (OR: 0.50, p: 1.69 × 10^−5^), and Quad‐CAB (OR: 0.55, p: 1.39 × 10^−2^). Increasing macrolide consumption by one unit reduced Triple CA effectiveness by 20% (OR: 0.8). Similar patterns were observed for delays up to 8 years, improving the fit of the model at all the time delays (Table 2). (Table 3) presents the effects of the interaction macrolide consumption/treatment on treatment effectiveness for delays of 0–8 years. For Triple‐CA, the interaction with macrolide consumption was significant across most delays. ORs were below one, indicating that higher levels of macrolide consumption were associated with reduced effectiveness compared to non‐clarithromycin‐based treatments. Similar patterns were observed for Triple‐CM, throughout different delays.
TABLE 3: Effect on treatment effectiveness of the interaction between H. pylori eradication treatments and macrolide consumption in the community throughout the full range of delays between macrolide consumption and treatment.
Conversely, ORs for Conco‐CAT‐CAM were slightly above one for two‐ and three‐year delays, as was that of Seq‐CAT‐CAMat for the five‐year delay, though effects were clinically minor. Quad‐CAB showed reduced effectiveness for one‐ and two‐year delays, but extreme OR values (6.44 and 88,000) for longer delays, likely due to small sample sizes affecting model stability. In fact, the last four cases for this treatment (5‐, 6‐, 7‐, and 8‐year delays) were calculated with 7.3%, 4%, 3.6%, and 3.5% of cases with respect to the reference level, highlighting a clear lack of robustness due to model instability.
Despite these variations, results remained consistent in the analysis of data from all countries and from those with the largest patient samples (Spain and Italy), thus reinforcing the reliability of the findings.
Average and Accumulated Macrolide Consumption
3.3
Macrolide consumption was analyzed as both accumulated and average intake over the years, but neither approach improved the core model, as LRT analysis showed no statistically significant effect.
Discussion
4
In the current study, we observed that previous macrolide consumption at the population level was ecologically associated with a significant reduction in the effectiveness of clarithromycin‐containing therapies in individual patients.
Several studies link personal antibiotic use to resistance and reduced efficacy [27, 28]. Accordingly, some authors recommend against clarithromycin‐based regimens after prior exposure [27], while others highlight the benefit of optimizing treatments based on past macrolide use [29].
Our study found that the effectiveness of clarithromycin‐based treatments was influenced not just by whether clarithromycin was used, but also by the DDD amount. A linear relationship was observed, with eradication rates declining as the daily dose increased. Specifically, eradication rates dropped from 93% for consumption below 1 DDD to 82% for 8 DDD. We also unveiled two key findings: firstly, higher levels of prior macrolide consumption were linked to lower treatment effectiveness, particularly if consumption occurred within 4 years before treatment; secondly, the negative impact was more pronounced for consumption within 2 years prior to receiving treatment and at higher macrolide doses.
Studies on other infections have shown that antibiotic resistance is higher when exposure occurs closer to treatment [30, 31], and decreases gradually over time [32, 33]. This pattern has been observed in both primary care and hospital settings [31, 34]. In hospitals, resistance often develops within 0 to 6 months after exposure [34]. For macrolides, resistance can persist for at least three months [30].
In our study, the global effects—analyzed with the core model including macrolide consumption but not the interaction between macrolide consumption and treatment—remained significant for up to a four‐year delay. Although adding macrolide consumption from the fifth year onward did not improve the core model's fit, the results still followed a similar pattern to earlier years, except for the six‐year delay. This pattern suggested that higher antibiotic consumption remained associated with lower treatment effectiveness over an extended period, though with a weaker impact. Previous studies suggest that longer intervals between exposure and treatment reduce the negative impact on H. pylori eradication [13, 14]. This may be due to interactions among diverse H. pylori colonies within a patient, leading to the disappearance of resistant strains. However, research beyond 5 years is limited [15], and longitudinal studies tracking strain evolution are lacking. Clarithromycin resistance results from irreversible mutations in the 23S rRNA gene, the antibiotic's binding site, with A2143G, A2142G, and A2142C being the most common mutations worldwide [12, 35]. Triple therapies were most affected by prior antibiotic use, with Triple‐CM and Triple‐CA showing a 50% and a 20% reduction, respectively. It is reasonable to assume that triple therapies involving antibiotics with higher antibiotic resistance rates, such as clarithromycin (over 15%) and metronidazole (over 30%), are more directly influenced by previous antibiotic consumption; thus, the greater susceptibility of Triple‐CM (OR = 0.50) to macrolide exposure compared to Triple‐CA (OR = 0.80) might stem from potential synergistic resistance between clarithromycin and metronidazole. Regional resistance data may help clarify this interaction as the decline persisted in the analysis of longer delays, especially for Triple‐CM. Interestingly, Quad‐CAB also showed reduced effectiveness with prior clarithromycin use, suggesting that even with bismuth, clarithromycin resistance remains influential. Additionally, Extreme OR values, such as ORs 88,000 or 0.009 for Quad‐CAB at 7 and 8‐year delay, reflect model instability due to small samples. These were retained for transparency but should be interpreted cautiously. Missing values in Table 3, such as for Triple‐CA and Triple‐CM in 2–4 years, reflect strata non‐significant interactions. Interestingly, for Conco‐CAT‐CAM, ORs were slightly above one for 2‐ and 3‐year delays, raising the possibility that concomitant therapy may be less susceptible to the effects of prior clarithromycin exposure. This finding contrasts with the treatment's exclusion in recent ACG guidelines and warrants further investigation in future trials.
Our study has several limitations. Firstly, due to its retrospective nature, several variables that may influence outcomes, such as smoking, alcohol consumption, socioeconomic status, hygiene practices, use of concomitant medications, and body mass index, among others, could not be analyzed. Antibiotic consumption was not assessed at the individual level; therefore, a potential bias may exist between individual antibiotic use and the presence of resistance or the eradication of H. pylori in that individual. Parallel data on antibiotic resistance for each country during the study period were also unavailable. Nonetheless, as observed in other studies of infections similar to ours, [30, 31] resistance tends to follow antibiotic consumption patterns. Importantly, antibiotic sales records can provide an approximate measure of population‐level antibiotic pressure and how such consumption may influence the efficacy of empiric treatments that include the same antibiotic; however, this approach has inherent limitations, as it does not capture individual exposure histories, indication‐specific use, or fully reflect resistance patterns, and therefore should be interpreted cautiously as a surrogate for treatment efficacy. The small sample size in some countries and treatment regimens limited subgroup analysis, though results remained consistent when focusing on Spain and Italy. Additionally, generalizing our findings is challenging due to the limited number of cases and centers in many countries. The impact of prior antibiotic use on second‐line treatment was not assessed, and neither was antibiotic susceptibility (with genetic analyses or cultures). Furthermore, we did not differentiate types of macrolides, and the system could only model macrolide consumption, not that of other antibiotics like metronidazole or levofloxacin. However, resistance to metronidazole has been reported to have minimal impact on eradication success. We also acknowledge that key confounders such as smoking status, alcohol use, body mass index (BMI), and CYP2C19 metabolizer phenotype were not available in the registry and could not be included in the models. Lastly, as this was an ecological study, it linked community‐level macrolide use with individual outcomes, introducing a risk of ecological fallacy and limiting causal inference, as individual macrolide exposure was not measured. Additionally, potential confounders such as personal antibiotic history and regional resistance patterns may have influenced the overall findings.
The study strengths include the large sample size (27,549 patients), the long follow‐up (10‐year evaluation), the use of international antibiotic data, and the assessment of real‐world treatment effectiveness across multiple countries and common regimens.
In conclusion, prior clarithromycin exposure in the general population significantly reduces the efficacy of first‐line H. pylori clarithromycin‐containing eradication regimens, particularly when exposure occurred within the past 5 years and at higher doses. The most affected regimens were clarithromycin‐based triple therapies and certain bismuth‐based quadruple therapies containing clarithromycin. It is necessary for governments to develop and standardize mandatory reporting items to enable meaningful comparisons—such as treatment indications, treatment types, diagnostic methods, adverse effects, resistance rates, and others. Additionally, prospective longitudinal studies in large populations, including biological samples and extended follow‐up periods, are needed to establish the biological and epidemiological mechanisms underlying this association.
Author Contributions
Olga P. Nyssen, Scientific Director and member of the project's Scientific Committee, planned and coordinated the study, designed and programmed the electronic case report form, extracted, analyzed, synthesized, and interpreted the data, wrote the first draft, acted as critical reviewer of the manuscript drafts, and approved the final submitted manuscript. Guillermo J. Ortega planned and coordinated the study, extracted, analyzed, synthesized, and interpreted the data, contributed to writing the first draft, and approved the final submitted manuscript. Leticia Moreira, Scientific Director and member of the project's Scientific Committee critically reviewed and approved the final submitted manuscript. Anna Cano‐Català, Pablo Parra, Francis Mégraud, and Colm O’Morain: members of the project's Scientific Committee, critically reviewed the manuscript drafts and approved the submitted manuscript. Luis Bujanda and Concepción Bravo‐Pache assisted with data interpretation, contributed to the writing of the first draft, and approved the submitted manuscript. Javier P. Gisbert, Principal investigator of the project, member of the Scientific Committee, obtained funding, designed the protocol and planned the study, analyzed and interpreted the data, collected patients, critically reviewed the manuscript drafts, and approved the final submitted manuscript. Laimas Jonaitis, Ángeles Pérez‐Aísa, Bojan Tepes, Pablo M. Wolfe Garcia, Perminder Singh Phull, Samuel J. Martínez Dominguez, Alfredo J. Lucendo, Javier Tejedor‐Tejada, Renate Bumane, Ana Garre, Jose M. Huguet, Monica Perona, Óscar Núñez, Manuel Pabón‐Carrasco, M. Castro‐Fernández, Miguel Areia, Jesús Barrio, Antonio Moreno Loro, Thomas J. Butler, María Soledad Marcos, Alma Keco‐Huerga, Manuel Domínguez Cajal, Maja Denkovski, Matteo Pavoni, György Miklós Buzás, Frode Lerang, Giuseppe Losurdo, Pablo M. Wolfe García, Samuel J. Martínez‐Domínguez, Juozas Kupcinskas, Mārcis Leja, Ricardo Marcos‐Pinto, Sinead M. Smith, Antonio Gasbarrini, Veronika Papp, Blas José Gómez Rodríguez, Mónica Sánchez Alonso, Ramón Pajares Villarroya, Pilar Pazo Mejide, Manuel Jiménez‐Moreno, Marta Pascual‐Mato, Milagrosa Montes, Leticia Moreira, Luis Bujanda, Javier P. Gisbert: acted as patients’ recruiters, critically reviewed the manuscript drafts, and approved the submitted manuscript.
Funding
This work was supported by Horizon EUROPE Health, 101095359 UK Research and Innovation, 10058099 EU4Health, 101101252. The Hp‐EuReg project was promoted and funded by the European Helicobacter and Microbiota Study Group (EHMSG; www.helicobacter.org) and received support from the Spanish Association of Gastroenterology (AEG) and the Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd). Hp‐EuReg was co‐funded by the European Union programme HORIZON (grant agreement number 101095359) and supported by the UK Research and Innovation (grant agreement number 10058099). Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union or the Health and Digital Executive Agency (HaDEA). Neither the European Union nor the granting authority can be held responsible for them. Hp‐EuReg was co‐funded by the European Union programme EU4Health (grant agreement number 101101252). Hp‐EuReg was also funded by Diasorin, Juvisé, and Biocodex; however, clinical data were not accessible to the companies, and they were not involved in any stage of the Hp‐EuReg study (design, data collection, statistical analysis, or manuscript writing).
Ethics Statement
The Hp‐EuReg protocol was approved by the Ethics Committee of Hospital Universitario de la Princesa (Madrid, Spain), which acted as a reference Institutional Review Board (IRB, 20 December 2012), was conducted according to the guidelines of the Declaration of Helsinki, was classified by the Spanish Agency for Medicines and Medical Devices and was prospectively registered in Clinical Trials.gov under the code NCT02328131. Multinational ethics approvals were obtained at the country level (i.e., for each of the participating countries reported in Figure 2), with oversight coordinated through the Spanish reference IRB.
Consent
This information is included in the text: “Written informed consent was obtained from all participants”.
Conflicts of Interest
Javier P. Gisbert has served as speaker, consultant, and advisory member for or has received research funding from Mayoly, Allergan/Abbvie, Diasorin, Richen, Juvisé, and Biocodex. Olga P. Nyssen has served as a speaker or has received research funding from Mayoly and Allergan. The remaining authors declare no conflicts of interest.
Supporting information
Data S1: Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. K. Y. Hooi , W. Y. Lai , W. K. Ng , et al., “Global prevalence of Helicobacter pylori infection: systematic review and meta‐analysis,” Gastroenterology 153 (2017): 420–429.28456631 10.1053/j.gastro.2017.04.022 · doi ↗ · pubmed ↗
- 2J. C. Yang and C. J. Lin , “ Helicobacter pylori and associated diseases beyond gastritis and peptic ulcers,” Frontiers in Microbiology 12 (2021): 770419.
- 3C. de Martel , D. Georges , F. Bray , J. Ferlay , and G. M. Clifford , “Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis,” Lancet Global Health 8 (2020): e 180–e 190.31862245 10.1016/S 2214-109X(19)30488-7 · doi ↗ · pubmed ↗
- 4P. Malfertheiner , F. Megraud , T. Rokkas , et al., “Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report,” Gut 71 (2022): 1724–1762.
- 5J. P. Gisbert , J. Alcedo , J. Amador , et al., “V Spanish Consensus Conference on Helicobacter pylori infection treatment,” Gastroenterología y Hepatología 45 (2022): 392–417.34629204 10.1016/j.gastrohep.2021.07.011 · doi ↗ · pubmed ↗
- 6O. P. Nyssen , D. Bordin , B. Tepes , et al., “European Registry on Helicobacter pylori management (Hp‐Eu Reg): patterns and trends in first‐line empirical eradication prescription and outcomes of 5 years and 21 533 patients,” Gut 70 (2021): 40–454.32958544 10.1136/gutjnl-2020-321372 · doi ↗ · pubmed ↗
- 7L. Bujanda , O. P. Nyssen , D. Vaira , et al., “Antibiotic resistance prevalence and trends in patients infected with Helicobacter pylori in the period 2013–2020: Results of the European Registry on H. pylori Management (Hp‐Eu Reg),” Antibiotics (Basel) 10 (2021): 1058.34572640 10.3390/antibiotics 10091058 PMC 8471667 · doi ↗ · pubmed ↗
- 8L. Bujanda , O. P. Nyssen , J. Ramos , et al., “Effectiveness of Helicobacter pylori treatments according to antibiotic resistance,” American Journal of Gastroenterology 119 (2024): 646–654.37983769 10.14309/ajg.0000000000002600 · doi ↗ · pubmed ↗