Effectiveness of Indapamide Prolonged‐Release and Perindopril Versus Perindopril Monotherapy for Treated Uncontrolled Hypertension: A Target Trial Emulation
Céline Darricarrere, Virginie Simon, Manel Pladevall‐Vila, Emmanuelle Jacquot, Morgane Ballon, Marie Mangin, Dominique Procureur, Jaume Aguado, Xabier Garcia‐Albeniz

TL;DR
Adding indapamide to perindopril lowers blood pressure more effectively than using perindopril alone in patients with uncontrolled hypertension.
Contribution
This study uses real-world data to emulate a clinical trial and demonstrates the added benefit of combining indapamide with perindopril for hypertension.
Findings
Adding indapamide to perindopril reduced systolic blood pressure by an average of 6.3 mmHg after 8 weeks.
Sensitivity analyses confirmed the robustness of the results despite different assumptions.
The combination therapy showed clinically meaningful improvements over monotherapy.
Abstract
To assess the effectiveness of indapamide prolonged release and perindopril in combination using blood pressure (BP) records collected in routine practice. Using a target trial emulation framework, an observational retrospective cohort study was conducted. The data source was the United Kingdom's CPRD Aurum general practice database. Adults with systolic BP (SBP) ≥ 145 mmHg treated with perindopril 4/5 mg for ≥ 4 weeks at a stable dose who either added indapamide 1.5 mg to perindopril (n = 193) or continued on perindopril monotherapy (n = 14 571) were included. Balance between treatment arms was achieved with propensity score matching; results were explored in additional analyses using different eligibility criteria and alternative statistical methodologies. The primary outcome was change in SBP from baseline to Week 8 between indapamide added to perindopril versus perindopril…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
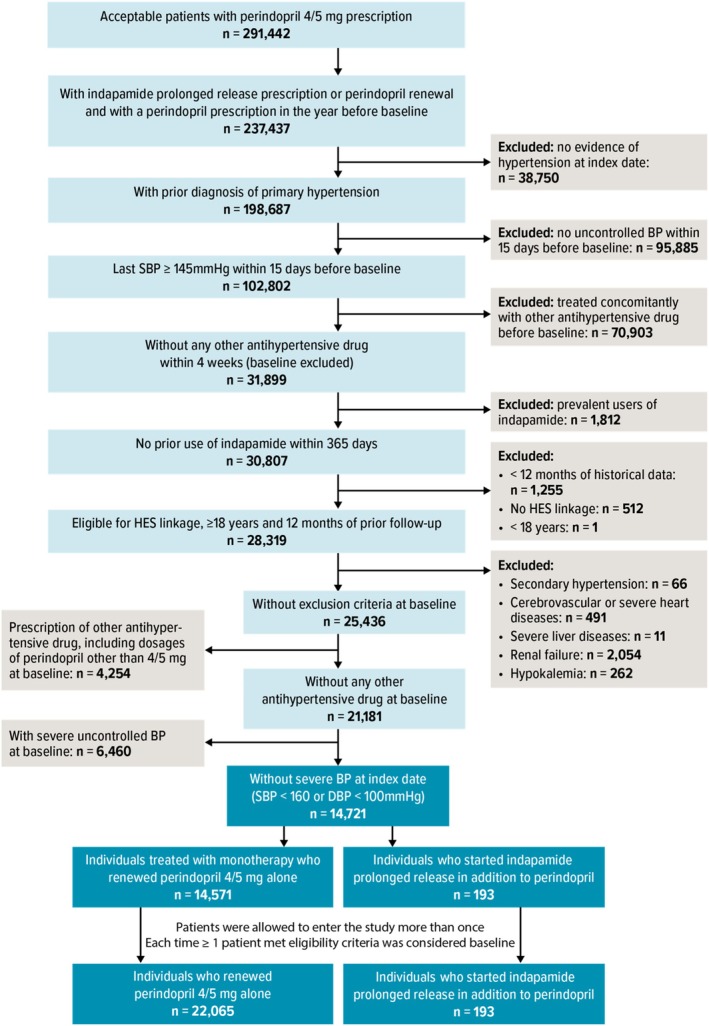 FIGURE 1
FIGURE 1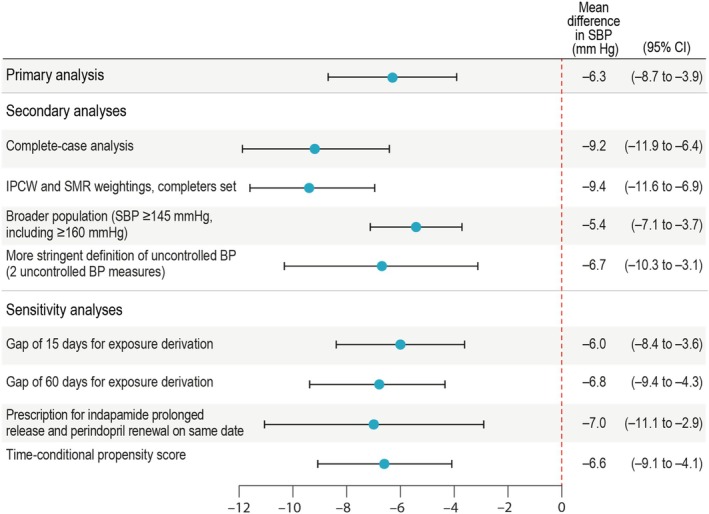 FIGURE 2
FIGURE 2| Target trial | Emulated trial | |
|---|---|---|
| Aim |
|
|
|
| ||
| Eligibility criteria | Inclusion criteria | Inclusion criteria |
|
Age ≥ 18 years |
Age ≥ 18 years | |
|
Diagnosis of primary hypertension, and the following measurements: SBP ≥ 145 mmHg and < 160 mmHg and DBP < 100 mmHg |
Diagnosis of primary hypertension, defined by the presence of a medical code for primary hypertension any time before baseline or by 2 successive records of SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg at distinct dates within 6 months before baseline Last record within 2 weeks before baseline of SBP ≥ 145 mmHg and < 160 mmHg and DBP < 100 mmHg | |
|
Received stable treatment with perindopril 5 mg for ≥ 4 weeks before baseline |
Received a prescription of perindopril 4 or 5 mg daily at a stable dose for ≥ 4 weeks before baseline Prescription of perindopril 4 or 5 mg during the year before baseline Initiated indapamide prolonged‐release 1.5 mg in addition to the ongoing exposure to perindopril or received a renewal prescription of perindipril 4 mg or 5 mg | |
|
Did not receive other antihypertensive treatment during the 4 weeks before baseline |
Did not receive other antihypertensive treatment during the 4 weeks before baseline Did not receive indapamide during the 12 months before baseline Had ≥ 12 months of continuous enrollment in the data source before baseline Had Hospital Episode Statistics linkage available | |
| Exclusion criteria | Exclusion criteria | |
|
Diagnosis of secondary hypertension |
Diagnosis of secondary hypertension | |
|
Moderate to severe uncontrolled hypertension with all SBP values ≥ 160 mmHg or all DBP values ≥ 100 mmHg recorded at baseline |
Moderate to severe uncontrolled hypertension with SBP ≥ 160 mmHg and DBP ≥ 100 mmHg ≥ 1 SBP value < 145 mmHg (indicative of controlled hypertension) if several values were recorded on the date of baseline BP Prescription at baseline of any antihypertensive treatment other than indapamide prolonged‐release 1.5 mg or perindopril 4 or 5 mg, including other dosages of perindopril, identified with record of at least 1 product code | |
|
Cerebrovascular, liver, or renal comorbidities or history of hypokalemia |
Cerebrovascular, | |
| Treatment strategies |
|
|
|
|
| |
| We considered treatment to be continuous if there was a gap of less than 30 days between successive prescriptions. Overlap of prescription was shifted forward. | ||
| Treatment assignment | Patients are randomly assigned to either arm at baseline. Baseline is defined as the beginning of the randomization period (i.e., the time of treatment assignment). | We classified individuals according to the observed treatment strategy at baseline and emulated randomization by matching individuals in the monotherapy arm to those in the free‐combination arm on a 3:1 basis based on the PS. Baseline covariates that remained imbalanced after matching |
| Patients who initiated indapamide prolonged‐release during an ongoing episode of perindopril and those who initiated indapamide prolonged‐release at the same time as renewal of a perindopril prescription were included in the free‐combination arm. Baseline in this group was the date of indapamide prolonged‐release prescription. Patients who received a renewal prescription of perindopril 5 or 4 mg without adding any other antihypertensive treatments were assigned to the monotherapy arm. Baseline in this group was the date of perindopril prescription renewal. | ||
| Eligibility criteria were met several times: patients were included in a treatment group (as individuals) each time they were eligible and aligned with study treatment strategies. A single patient could be included and contribute to the analysis as several individuals with different baselines and, potentially, different exposures (i.e., multiple eligibility) [ | ||
| Follow‐up | Patients are followed from treatment assignment to 12 weeks afterward. | Patients were followed from treatment assignment until the end of practice data, transfer out of the practice, any change in assigned treatment (including addition of other antihypertensive treatments or increased dose of indapamide prolonged‐release or perindopril), discontinuation of treatment of interest, death, or 1 year after baseline, whichever occurred first. |
| Patients are monitored with 1 visit and BP measurement after 4 and 8 weeks. | ||
| Outcome | Change in SBP (primary outcome) or DBP (secondary outcome) between baseline and Week 8. | Same |
| Baseline BP was defined as the measurement taken within 2 weeks before or at baseline. Outcome BP was defined as the measurement taken between Weeks 4 and 24 after baseline that was closest to Week 8 after baseline. | ||
| When multiple BP measurements were recorded on the same day, the mean value was used. | ||
| Estimand | The primary estimand of interest is the difference in mean change from baseline in sitting SBP after 8 weeks of indapamide prolonged‐release 1.5 mg in addition to perindopril 5 mg compared with perindopril 5 mg monotherapy in patients with hypertension not controlled (SBP 145–159 mmHg and DBP < 100 mmHg) on perindopril 5 mg monotherapy, assuming no other antihypertensive concomitant treatments were taken and assuming no switch to other therapy following premature treatment discontinuation. | Same |
| The ICEs that are considered in the estimand definitions are: premature treatment discontinuation or dose increase or use of any other antihypertensive treatment. | ||
| Statistical analysis | The change in mean BP is estimated via linear regression (ANCOVA). | Same |
| Additional adjustment occurred for imbalanced baseline variables. | ||
| Patients deviating from the assigned treatment strategy are censored and assigned a missing outcome. Missing outcomes in case of ICEs are imputed with the baseline BP value assuming no treatment benefit. | Patients deviating from the assigned treatment strategy, including addition of or switch to other antihypertensive treatments, increased dose, or discontinuation of assigned treatment, were censored. Missing outcomes in case of such ICEs were imputed with the baseline BP value assuming no treatment benefit. | |
| Other missing data (missing outcomes in compliant patients and baseline variables in any patient) are handled via multiple imputation under the assumption that they are MAR. | Missing outcomes for patients who remained treated with the baseline strategy until 24 weeks were handled via multiple imputation, under the assumptions that they are MAR and that these individuals would have had similar effectiveness outcomes as individuals from their treatment group. |
| Monotherapy ( | Free combination ( | ASD | |
|---|---|---|---|
| Gender, | |||
| Male | 294 (50.8) | 103 (53.4) | |
| Female | 285 (49.2) | 90 (46.6) | 0.052 |
| Age (years), mean ± SD | 61.2 ± 12.1 | 61.5 ± 12.8 | 0.025 |
| Ethnicity, | |||
| White | 532 (91.9) | 178 (92.2) | 0.013 |
| Mixed/multiple ethnic groups | < 5 | — | 0.083 |
| Asian or Asian British | 10 (1.7) | 6 (3.1) | 0.090 |
| Black/African/Caribbean/Black British | 9 (1.6) | < 5 |
|
| Other | < 5 | < 5 | 0.059 |
| Missing | 25 (4.3) | 7 (3.6) | 0.035 |
| Body mass index, class, | |||
| Underweight | — | < 5 |
|
| Normal | 119 (20.6) | 39 (20.2) | 0.009 |
| Overweight | 210 (36.3) | 72 (37.3) | 0.021 |
| Obesity | 74 (12.8) | 25 (13.0) | 0.005 |
| Severely obese | 69 (11.9) | 21 (10.9) | 0.033 |
| Missing | 107 (18.5) | 35 (18.1) | 0.009 |
| Body mass index (kg/m2), mean | 29.1 ± 5.6 | 28.9 ± 5.2 | 0.034 |
| SBP at baseline (mmHg) | |||
| Mean ± SD | 152.5 ± 5.3 | 152.8 ± 4.7 | 0.053 |
| Median | 152.0 | 152.0 | |
| Q1; Q3 | 149.0; 156.0 | 150.0; 156.0 | |
| DBP at baseline (mmHg) | 0.010 | ||
| Mean ± SD | 86.2 ± 8.7 | 86.1 ± 9.2 | |
| Median | 88.0 | 88.0 | |
| Q1; Q3 | 80.0; 92.0 | 80.0; 92.0 | |
| Severity of hypertension, | |||
| SBP 145–159 mmHg and/or DBP 90–99 mmHg | 558 (96.4) | 186 (96.4) | 0.000 |
| SBP 160–179 mmHg and/or DBP 100–119 mmHg | 18 (3.1) | 7 (3.6) | 0.029 |
| SBP ≥ 180 mmHg and/or DBP ≥ 120 mmHg | < 5 | — |
|
| Number of previous antihypertensive treatments in the year before baseline (perindopril excluded), mean ± SD | 0.3 ± 0.6 | 0.3 ± 0.6 | 0.014 |
| 0 | 442 (76.3) | 143 (74.1) | 0.052 |
| 1 | 99 (17.1) | 39 (20.2) | 0.080 |
| 2 | 33 (5.7) | 10 (5.2) | 0.023 |
| 3 | < 5 | < 5 | 0.022 |
| ≥ 4 | < 5 | — | 0.059 |
| Cardiovascular comorbidities, | |||
| Stroke | 82 (14.2) | 26 (13.5) | 0.020 |
| Myocardial infarction | < 5 | < 5 |
|
| Heart failure | < 5 | < 5 | 0.000 |
| Periphery artery disease | 22 (3.8) | 5 (2.6) | 0.069 |
| Coronary artery disease | 29 (5.0) | 8 (4.1) | 0.041 |
| Cardiac revascularization | < 5 | < 5 | 0.026 |
| Left ventricular hypertrophy | 8 (1.4) | < 5 | 0.032 |
| Monotherapy ( | Free combination ( | |
|---|---|---|
|
| ||
| SBP at baseline (mmHg) | ||
| Mean ± SD | 152.5 ± 5.3 | 152.8 ± 4.7 |
| Median | 152.0 | 152.0 |
| Q1; Q3 | 149.0; 156.0 | 150.0; 156.0 |
| Min; Max | 145; 188 | 145; 170 |
| SBP at Week 8 (mmHg) | ||
| Mean ± SD | 149.2 ± 12.4 | 142.8 ± 12.0 |
| Median | 149.0 | 145.0 |
| Q1; Q3 | 142.0; 155.0 | 135.0; 152.0 |
| Min; Max | 106; 218 | 105; 172 |
| SBP change between baseline and Week 8 (mmHg) | ||
| Mean ± SD | −3.3 ± 12.8 | −9.9 ± 12.2 |
| Median | −2.0 | −8.0 |
| Q1; Q3 | −10.0; 0.8 | −18.0; 0.0 |
| Min; Max | −48; 68 | −50; 17 |
| Comparison between treatment groups of SBP change (mmHg), estimate (95% CI) | −6.3 (−8.7 to −3.9) | |
|
| ||
| DBP at baseline (mmHg) | ||
| Mean ± SD | 86.2 ± 8.7 | 86.1 ± 9.2 |
| Median | 88.0 | 88.0 |
| Q1; Q3 | 80.0; 92.0 | 80.0; 92.0 |
| Min; Max | 51; 110 | 60; 102 |
| DBP at Week 8 (mmHg) | ||
| Mean ± SD | 84.6 ± 8.9 | 82.2 ± 9.0 |
| Median | 85.0 | 82.0 |
| Q1; Q3 | 80.0; 90.0 | 78.0; 88.0 |
| Min; Max | 51; 120 | 58; 104 |
| DBP change between baseline and Week 8 (mmHg) | ||
| Mean ± SD | −1.6 ± 8.4 | −3.8 ± 8.0 |
| Median | 0.0 | −1.6 |
| Q1; Q3 | −5.9; 2.0 | −8.0; 0.0 |
| Min; Max | −37; 48 | −30; 36 |
| Comparison between treatment groups of DBP change (mmHg), estimate (95% CI) | −2.3 (−3.7; −0.8) |
- —Servier10.13039/501100011725
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Heart rate and cardiovascular health · Anesthesia and Sedative Agents
Introduction
1
Hypertension is a major cardiovascular risk factor, and reduction of blood pressure (BP) can decrease mortality and mortality due to cardiovascular disease [1]. In the United Kingdom (UK), the prevalence of hypertension was 30% in men and 26% in women in 2018 [2]. A primary reason for uncontrolled hypertension is that many patients receive only monotherapy [3, 4], although patients may benefit from multiple therapies to achieve optimal and sustained BP control [5]. Based on NICE guidelines, treatment should be initiated with an angiotensin‐converting enzyme inhibitor, angiotensin receptor blocker, or calcium channel blocker, depending on patient profile. If BP control is inadequate on a single agent, a second drug should be added, such as a thiazide‐like diuretic or a calcium channel blocker, if not already used in the first line [6]. For example, the combination of the antihypertensive treatments perindopril (an angiotensin‐converting enzyme inhibitor) and indapamide (a diuretic drug) may yield better control of hypertension compared with monotherapy [7, 8, 9].
Antihypertensive treatment efficacy is typically evaluated in randomized controlled trials (RCTs) with protocolized, iterative measuring of BP. When RCTs are not feasible or pragmatic, observational analyses using real‐world data (RWD) can provide evidence on the comparative effectiveness of potential interventions [10, 11]. With explicit specification of the hypothetical target trial and rigorous statistical methods to control for biases and confounding, observational analyses can elicit similar estimates of treatment effects as would be achieved with an RCT [10]. Within a target trial emulation framework, BP measurements from electronic medical records (EMRs) are a valuable data source for assessing the antihypertensive effectiveness of treatments used in routine care.
The objective of this study was to estimate change in BP from baseline to Week 8 in patients who are adding indapamide prolonged‐release formulation to perindopril (free‐combination therapy) compared with perindopril alone (monotherapy). Perindopril and indapamide were largely studied alone or in combination [7, 8, 12, 13, 14, 15, 16], but no data are available comparing the prolonged‐release formulation of indapamide in combination with perindopril to perindopril alone. A secondary methodological objective was to assess alternative statistical methods and population definitions for identifying the antihypertensive effects of free‐combination therapy versus monotherapy. Specifically, we analyzed BP measures collected in routine practice via EMRs in the UK's Clinical Practice Research Datalink (CPRD Aurum) and implemented several approaches to minimize potential confounding and selection bias when comparing antihypertensive strategies.
Materials and Methods
2
Target Trial Specification
2.1
To estimate the effect of adding indapamide prolonged‐release formulation to perindopril on BP using observational data, we first specified the target trial (Table 1). Briefly, eligibility criteria for the trial population would have been age ≥ 18 years, diagnosis of primary hypertension at baseline (systolic blood pressure [SBP] ≥ 145 mmHg and < 160 mmHg in the 2 weeks before baseline) despite stable therapy with perindopril 5 mg for ≥ 4 weeks, and no use of any other antihypertensive treatment in the preceding 4 weeks. To exclude transient limited increase of SBP and ensure inclusion of true uncontrolled hypertension, 145 mmHg was selected as the threshold for uncontrolled systolic hypertension (typically defined by SBP ≥ 140 mmHg in clinical practice). Patients with moderate to severe uncontrolled hypertension (SBP ≥ 160 mmHg and diastolic blood pressure [DBP] ≥ 100 mmHg) would have been excluded for ethical reasons, to avoid enrolling patients who could benefit from a more aggressive therapy (particularly if they were randomized to the arm with no addition of indapamide prolonged‐release). Patients would have been randomized either to continue receiving perindopril 5 mg (control arm) or to receive indapamide prolonged‐release 1.5 mg in addition to perindopril 5 mg (free‐combination arm). The primary estimand [18] of interest would have been the difference in mean change from baseline in SBP after 8 weeks of perindopril 5 mg/indapamide prolonged‐release 1.5 mg compared with perindopril 5 mg monotherapy in patients with hypertension not controlled on perindopril 5 mg monotherapy, assuming no change in assigned therapy.
Target Trial Emulation
2.2
Data Sources
2.2.1
We emulated this target trial via a matched cohort design (Table 1) [10, 11] using the UK's CPRD Aurum database, which collects anonymized EMR data from general practitioners and, as of April 2021, included data for approximately 13 million patients registered at approximately 1400 practices [19]. The study was approved by the CPRD's Independent Scientific Advisory Committee (ISAC) in March 2021 (protocol number 20_000194). eAppendix A describes CPRD Aurum in detail. For assessment of covariates, primary care data from CPRD Aurum were linked to 2 additional data sources: Index of Multiple Deprivation (IMD) for socioeconomic data and the Hospital Episode Statistics Admitted Patient Care (HES APC) for diagnoses recorded in hospitals.
Study Population
2.2.2
Patients were identified between January 2000 and March 2020 and were followed for up to 12 months. To emulate the target trial eligibility criteria, a diagnosis of primary hypertension was defined by the presence of a medical code for primary hypertension any time before baseline or by 2 successive records of elevated BP (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg) at distinct dates within 6 months before baseline. Table 1 presents the inclusion and exclusion criteria. Eligible patients either initiated indapamide prolonged‐release 1.5 mg in addition to an ongoing exposure to perindopril arginine 5 mg (or an equivalent dose of perindopril tert‐butylamine 4 mg) daily (free‐combination initiation) or received a renewal prescription of perindopril 4 mg or 5 mg daily (monotherapy continuation) the same day or in the 2 weeks after an SBP measurement of ≥ 145 mmHg and < 160 mmHg. Perindopril 5 mg is rarely used in the UK, and perindopril 4 and 5 mg are bioequivalent [20]; thus, these 2 dosages were interchangeably used. Study baseline was the date of the new indapamide prolonged‐release prescription for the free‐combination arm or renewed perindopril prescription for the monotherapy arm. Eligibility was assessed at the study baseline. To properly evaluate baseline variables, patients were required to have ≥ 12 months of continuous enrollment in CPRD Aurum before baseline and linkage with HES APC data.
Patients were followed from treatment assignment until the end of practice data, transfer out of practice, any change from assigned treatment including addition of other antihypertensive treatments, increased dose, or discontinuation, death, or 1 year after baseline, whichever occurred first.
Treatment Groups
2.2.3
Treatment strategies were the same as in the target trial. Eligibility criteria could be met several times (see Figure 1) and patients were included in a treatment group (as individuals) each time they were eligible and aligned with study treatment strategies. Therefore, a single patient could be included in and contribute to the analysis as several individuals with different baselines and, potentially, different exposures (i.e., multiple eligibility) [17]. Patients were matched in a 3:1 ratio (monotherapy: free combination) on a propensity score (PS) that accounted for sociodemographic characteristics, hypertension history, practice‐specific variables, treatment history, cardiovascular history, use of healthcare resources, comorbidities, and concomitant therapies (Table 1). Comorbidities selected to balance the study population were the most medically relevant confounders on SBP measurement. The absolute standardized difference (ASD) was used to assess covariate balance between treatment groups before and after matching. Variables with an ASD ≥ 0.1, indicative of remaining imbalance in the matched population, were adjusted on in the final treatment‐effect estimation model (see eAppendix B).
Study population flow chart. BP = blood pressure; DBP = diastolic blood pressure; HES = Hospital Episode Statistics; HT = hypertension; SBP = systolic blood pressure. eTable D1 presents the number of inclusions in the perindopril arm and/or free combination arm in the matched cohort.
Estimand
2.2.4
The estimand [18] was the effectiveness estimate for free combination compared with monotherapy in the treated population (i.e., average treatment effect in the treated population [ATT]) with SBP ≥ 145 mmHg, during ongoing exposure to the assigned therapy. The primary outcome of the emulated trial was change in SBP between baseline and Week 8. To account for actual frequency of BP reports in EMRs, the BP measurement closest to Week 8 in the interval of Weeks 4–24 after baseline was used to maximize the number of patients with an available BP outcome. Intercurrent events (ICEs) considered for this estimand were treatment changes including prescription of other antihypertensive treatments, increased dose, and discontinuation of assigned treatment.
Primary Analysis
2.3
The treatment effect—the mean difference in SBP (primary outcome) between baseline and Week 8 for matched treatment groups—was estimated by a linear regression (analysis of covariance). ICEs were handled using a hypothetical strategy of treatment failure, and outcomes of patients with ICEs (and no BP record before ICE occurrence) were imputed using the baseline BP value and assuming no treatment benefit or worsening (missing not at random assumption) [21]. Thus, the treatment effect reflected a lack of benefit for the patient without considering the effect of other therapies following premature treatment change.
Missing outcomes for patients treated with the baseline strategy until Week 24 and without ICEs were handled via multiple imputation, assuming that these patients would have had similar effectiveness outcomes as patients from their treatment group (missing at random [MAR] assumption) [21].
To account for the effect of multiple eligibility and matching on variance estimation, 1000 bootstrapped samples were generated to estimate the 95% confidence intervals (CIs). Estimates and variance estimates were combined using Rubin rules [22].
Secondary and Sensitivity Analyses
2.4
As a secondary outcome, the mean difference in DBP from baseline to Week 8 between matched treatment groups was estimated with a similar approach as in the primary analysis. A secondary methodological objective of the study was to assess several definitions of the study population and different analytical approaches to the study of BP in CPRD Aurum. Specifically, a complete‐case analysis was conducted to assess the impact of missing data, and standardized mortality ratio (SMR) weighting [23] was used instead of PS matching. Additional study populations, including a “broader population” of patients with more severe hypertension and a “restricted uncontrolled population” of patients with 2 successive measurements of SBP ≥ 145 mmHg, were explored. Multiple sensitivity analyses were conducted evaluating different definitions of continuous treatment, the impact of restricting the free‐combination arm to patients initiating indapamide on the same date their perindopril prescription was renewed, the potential for bias in the comparison of new users of free‐combination therapy with prevalent users of monotherapy due to differences in disease course between treatment arms using a time‐conditional PS approach, and the impact of extending the window for SBP outcome assessment to 52 weeks after baseline. eAppendix C describes these additional analyses in detail.
Results
3
Study Population
3.1
Applying the inclusion and exclusion criteria to the 291 442 users of perindopril 4/5 mg identified between January 2000 and March 2020 resulted in 22 065 individuals (corresponding to 14 571 unique patients) assigned to the monotherapy arm and 193 individuals (all unique) assigned to the free‐combination arm (Figure 1).
Before PS matching, the overall included population was 54.3% male (monotherapy: 54.3%; free combination: 53.4%); mean (± standard deviation [SD]) age was 64.5 years (±12.4), and individuals receiving free combination were younger than those receiving monotherapy (61.5 vs. 64.6 years, respectively). Most individuals were aged < 75 years (monotherapy: 77.3%; free combination: 84.3%); most were White (monotherapy: 92.1%; free combination: 92.2%), followed by Asian (3.1% and 3.1%, respectively). Additional demographics, clinical characteristics, and details of medical and treatment history, before and after PS matching, are summarized in eAppendix D (eTables D2–D8).
All 193 eligible individuals in the free‐combination arm were successfully matched to 579 individuals in the monotherapy arm. In this matched cohort, 1 patient contributed as an eligible individual to both the free‐combination arm and the monotherapy arm, 192 patients contributed uniquely and only once as individuals to the free‐combination arm, and 548 patients contributed as 578 individuals (15 patients contributed twice) only to the monotherapy arm (eTable D1). Covariates at baseline were generally well balanced after matching (Table 2 and eTables D2–D8, eAppendix D). Some covariates that remained imbalanced after matching (see eFigure D1, eAppendix D) had an ASD that exceeded 0.1, but all were close to 0.1. These covariates were added in the final treatment‐effect estimation model to account for the remaining confounding bias. Mean (±SD) duration of follow‐up was 7.6 months (±4.6) for the overall matched cohort, 6.2 months (±4.7) for the free‐combination arm, and 8.0 months (±4.5) for the monotherapy arm.
Primary Analysis
3.2
In the primary analysis, time to the SBP measurement used as an outcome is described in eTable D9. After PS matching, 58 individuals (30.1%) in the free‐combination arm and 89 (15.4%) in the monotherapy arm changed or stopped their original treatment (before having BP recorded between 4 and 24 weeks); outcome BP was imputed by baseline value for these individuals. Nineteen individuals (9.8%) in the free‐combination arm and 151 individuals (26.1%) in the monotherapy arm without outcome or ICEs between Weeks 4–24 had their outcome imputed using multiple imputation. At Week 8, mean (±SD) reduction in SBP values was −3.3 mmHg (±12.8) for individuals receiving monotherapy and −9.9 mmHg (±12.2) for individuals receiving free combination; mean (±SD) reductions in DBP values were −1.6 mmHg (±8.4) and −3.8 mmHg (±8.0), respectively (Table 3). Once adjusted for final imbalanced covariates, the addition of indapamide prolonged‐release to perindopril led to an additional reduction of −6.3 mmHg (95% CI, −8.7 to −3.9) in SBP (Figure 2) and −2.3 mmHg (95% CI, −3.7 to −0.8) in DBP compared with the continuation on perindopril monotherapy (Table 3).
Forest plot of the primary outcome: Primary, Secondary, and Sensitivity Analyses. BP = blood pressure; CI = confidence interval; IPCW = inverse probability censoring weighting; SBP = systolic blood pressure; SMR = standardized mortality ratio.
Secondary Analyses
3.3
When considering the subpopulation of matched completers (patients with an outcome recorded while treated with baseline strategy; N = 460), the additional SBP reduction was −9.2 mmHg (95% CI, −11.9 to −6.4) for free‐combination compared with monotherapy (Figure 2; eTable E1, eAppendix E). When the alternative SMR–ICPW method was applied to completers, the additional SBP reduction was −9.4 mmHg (95% CI, −11.6 to −6.9) (Figure 2; eTable E2, eAppendix E).
Results for the alternative populations were similar to those for the main population (Figure 2; eTable E1, eAppendix E). The analysis of the broader matched population (including more severe patients, with no restriction for those who had all their SBP values ≥ 160 mmHg or DBP ≥ 100 at baseline [N = 2332]) yielded an additional SBP reduction of −5.4 mmHg (95% CI, −7.1 to −3.7) with free combination compared with monotherapy. The analysis of the matched population that applied a stringent definition of uncontrolled BP (i.e., the restricted uncontrolled population; see eAppendix C) (N = 376) resulted in an additional SBP reduction of −6.7 mmHg (95% CI, −10.3 to −3.1).
Sensitivity Analyses
3.4
The sensitivity analyses produced results similar to those from the main analysis (Figure 2). Mean differences in SBP for the comparison of free combination versus monotherapy were in line with results from the main analysis when gaps of 15 days (−6.0 mmHg; 95% CI, −8.4 to −3.6) or 60 days (−6.8 mmHg; 95% CI, −9.4 to −4.3) were used to derive treatment‐exposure duration. When restricting the free‐combination arm to patients with prescriptions for both indapamide prolonged‐release and perindopril renewal on the same date, the difference in SBP between study arms was −7.0 mmHg (95% CI, −11.1 to −2.9). Results from the analysis using time‐conditional PS were similar to those from the main analysis: an additional SBP reduction of −6.6 mmHg (95% CI, −9.1 to −4.1) was observed for free combination compared with monotherapy. Finally, applying a 52‐week window for evaluating the SBP outcome closest to Week 8 resulted in a similar estimate for SBP reduction as in the main analysis (−6.5 mmHg; 95% CI, −8.8 to −4.1). In this analysis, the number of patients with a BP outcome available while on their original treatment increased from 116 to 126 for the free‐combination arm and from 339 to 465 for the monotherapy arm.
Discussion
4
Results of this study reveal that beginning the addition of indapamide prolonged‐release 1.5 mg to perindopril 4/5 mg for patients with an SPB ≥ 145 mmHg was associated with a clinically relevant decrease in SBP. In the primary analysis, the addition of indapamide prolonged‐release to perindopril led to an additional SBP reduction of −6.3 mmHg (95% CI, −8.7 to −3.9) and an additional reduction of −2.3 mmHg (95% CI, −3.7 to −0.8) in DBP at Week 8 compared with perindopril monotherapy. Results are consistent with previous studies comparing the antihypertensive effects of combination regimens to monotherapy and with current guidelines on the management of hypertension [9, 25, 26, 27, 28]. Results are also within the range of results from placebo‐controlled clinical trials evaluating the antihypertensive effects of indapamide or indapamide plus perindopril, which have reported decreases in SBP between 5.6 and 15 mmHg [29].
In the analysis of matched completers, the additional reduction in SBP achieved with free combination was greater (−9.2 mmHg [95% CI, −11.9 to −6.4]) than in the primary analysis. The results of the complete‐case analysis can only be applied to the entire study population under the assumption that data are missing completely at random. To relax such strong assumptions, we imputed baseline values to the outcomes of patients who changed their assigned treatment (30.1% in the free‐combination arm and 15.4% in the monotherapy arm). Such single imputation assumes that the reason for changing treatment was no improvement in SBP and provides a conservative effect estimate. For patients with missing outcomes and no treatment change, these were imputed via multiple imputation, which assumes that the outcome is MAR. A third approach to deal with missing outcomes comprised the use of inverse probability weighting, which weights completers to account for similar individuals without outcome records or with ICEs who are excluded from the analysis, assuming that missingness is at random conditional on the covariates used to estimate the weights (in our case, the same used for the PS model). Additionally, a wider time‐window for SBP outcome assessment, using the closest SBP value up to 8 weeks over a period of 4–52 weeks after baseline was used to decrease the number of missing outcomes. This wider period to ascertain the outcome assumes that it does not introduce measurement error in the outcome. All assumptions to deal with missing outcomes are unverifiable, but the consistency of the results under all different approaches (and assumptions) is reassuring for a true effect of the free‐combination on SBP compared with monotherapy. The potential for regression to the mean was accounted for by including baseline SBP in the final model.
Results of the primary analysis were consistent with results from samples defined using different eligibility criteria, including those defined by moderate to severe uncontrolled hypertension. Results stratified by calendar year and by age were consistent with the main analysis (eTable E3). In the target trial, these individuals would have been excluded to avoid enrolling patients who could potentially benefit from more aggressive therapy. In this observational study, BP outcomes for individuals with more severe uncontrolled hypertension were able to be evaluated with no additional harm. Results of the primary analysis were also consistent with those from sensitivity analyses, including use of time‐conditional PS matching (−6.6 mmHg [95% CI, −9.1 to −4.1]). Alternative methods to adjust for selection bias due to censoring and confounding provided a different estimate of treatment effect (−9.4 mmHg [95% CI, −11.6 to −6.9]) closer to the complete‐case result. Overall, study findings were consistent across alternative methods accounting for the real‐world nature of the data.
As RWD become increasingly relevant in premarketing regulatory decisions, comparative‐effectiveness evidence is needed. Nonetheless, limitations related to the use of an automated healthcare database as a data source and to inconsistent BP recordings in EMRs must be noted. Assessment of SBP at Week 8 as a main outcome in CPRD Aurum was associated with missing data, and some patients discontinued or changed treatment during the outcome assessment time window without necessarily having a BP measurement taken beforehand. To avoid related selection bias, all patients in the matched cohort were analyzed, and imputation strategies accounted for ICEs and missing outcomes, as described above. Furthermore, BP readings were collected from EMRs and were not validated. Therefore, the potential for measurement bias due to measurement error (likely non‐differential) needs to be considered.
Results can be subject to confounding bias and, in particular, to channeling bias, because patients starting combination therapy may be more severe patients than patients remaining treated with perindopril alone. Measured confounders were adjusted for via PS matching. To further control for confounding related to severity, a time‐conditional PS based on duration of perindopril exposure was conducted [30]. Nonetheless, residual confounding due to unmeasured factors like diet or lifestyle may still be present, although we did adjust for body mass index, smoking, and alcohol consumption, which are likely good surrogates of those unmeasured factors. Finally, although the analyses did not account for medication adherence during follow‐up, adherence to perindopril in the year before baseline was taken into account. The occurrence of adverse events was not evaluated because they were out of the scope of this study.
Conclusions
5
This comparative‐effectiveness study used RWD from CPRD Aurum to emulate a hypothetical target trial evaluating the effectiveness of adding indapamide prolonged‐release to perindopril for BP reduction in patients with SBP ≥ 145 mmHg. Our data are compatible with a clinically meaningful BP reduction at 8 weeks of therapy due to the addition of indapamide prolonged‐release to perindopril compared with perindopril monotherapy in patients with an SBP ≥ 145 mmHg previously taking perindopril monotherapy. Results were consistent in secondary and sensitivity analyses, showcasing some epidemiological methods for analyzing BP outcomes in CPRD Aurum that may be informative for future research using this data source.
Funding
This work was supported by Servier.
Conflicts of Interest
This research and development of this publication were funded by Servier. Céline Darricarrere, Virginie Simon, Emmanuelle Jacquot, and Dominique Procureur were employees of Servier when this research was conducted. Morgane Ballon and Marie Mangin were full‐time consultants for Servier when this research was conducted. Jaume Aguado, Manel Pladevall‐Vila, and Xabier Garcia de Albeniz Martinez are employees of RTI Health Solutions, which received research funding to collaborate on this study.
Supporting information
Data S1: Supplementary appendix.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Brunström and B. Carlberg , “Association of Blood Pressure Lowering With Mortality and Cardiovascular Disease Across Blood Pressure Levels: A Systematic Review and Meta‐Analysis,” JAMA Internal Medicine 178, no. 1 (2018): 28–36, 10.1001/jamainternmed.2017.6015.29131895 PMC 5833509 · doi ↗ · pubmed ↗
- 2National Health Service England , “Health Survey for England 2018,” accessed September 20, 2023, https://digital.nhs.uk/data‐and‐information/publications/statistical/health‐survey‐for‐england/2018.
- 3K. T. Mills , J. D. Bundy , T. N. Kelly , et al., “Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population‐Based Studies From 90 Countries,” Circulation 134, no. 6 (2016): 441–450, 10.1161/CIRCULATIONAHA.115.018912.27502908 PMC 4979614 · doi ↗ · pubmed ↗
- 4C. K. Chow , K. K. Teo , S. Rangarajan , et al., “Prevalence, Awareness, Treatment, and Control of Hypertension in Rural and Urban Communities in High‐, Middle‐, and Low‐Income Countries,” JAMA 310, no. 9 (2013): 959–968, 10.1001/jama.2013.184182.24002282 · doi ↗ · pubmed ↗
- 5D. S. Wald , M. Law , J. K. Morris , J. P. Bestwick , and N. J. Wald , “Combination Therapy Versus Monotherapy in Reducing Blood Pressure: Meta‐Analysis on 11,000 Participants From 42 Trials,” American Journal of Medicine 122, no. 3 (2009): 290–300, 10.1016/j.amjmed.2008.09.038.19272490 · doi ↗ · pubmed ↗
- 6National Institute for Health and Care Excellence , “Hypertension in Adults: Diagnosis and Management,” NICE Guideline NG 136, accessed September 20, 2023, https://www.nice.org.uk/guidance/ng 136.
- 7J. J. Mourad , B. Waeber , F. Zannad , et al., “Comparison of Different Therapeutic Strategies in Hypertension: A Low‐Dose Combination of Perindopril/Indapamide Versus a Sequential Monotherapy or a Stepped‐Care Approach,” Journal of Hypertension 22, no. 12 (2004): 2379–2386, 10.1097/00004872-200412000-00021.15614033 · doi ↗ · pubmed ↗
- 8B. Dahlöf , P. Gosse , P. Guéret , et al., “Perindopril/Indapamide Combination More Effective Than Enalapril in Reducing Blood Pressure and Left Ventricular Mass: The PICXEL Study,” Journal of Hypertension 23, no. 11 (2005): 2063–2070, 10.1097/01.hjh.0000187253.35245.dc.16208150 · doi ↗ · pubmed ↗