Initial Capture Failure With Delayed Resolution in Atrial Leadless Pacemaker Implantation: A Case of ATTR Amyloidosis With Sinus Node Dysfunction
Yasuyuki Takada, Junichi Kamoshida, Muryo Terasawa, Kazuhiro Satomi, Yoshinao Yazaki

TL;DR
A patient with a rare heart condition had initial issues with a pacemaker but improved over time without needing surgery.
Contribution
Demonstrates successful expectant management of atrial capture failure in ATTR amyloidosis.
Findings
Initial atrial capture failure occurred in a patient with ATTR amyloidosis.
Delayed threshold improvement was observed without device repositioning.
Stable injury current and impedance guided successful management.
Abstract
ATTR amyloidosis patient with initial atrial capture failure showed delayed threshold improvement over time. Stable current of injury and impedance guided expectant management, avoiding unnecessary device repositioning while achieving successful outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
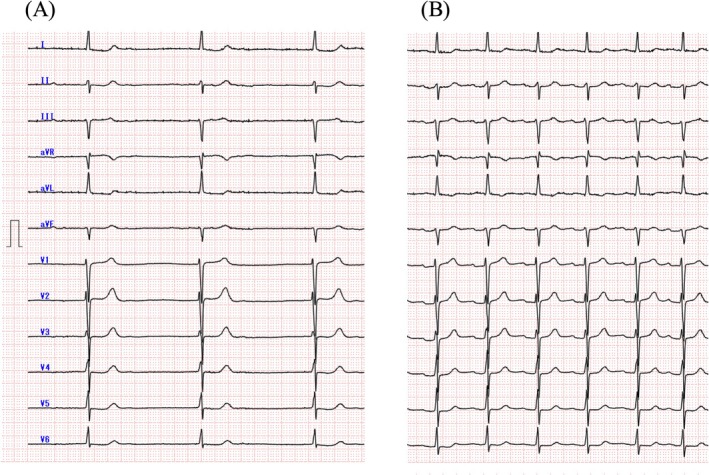 Figure 1
Figure 1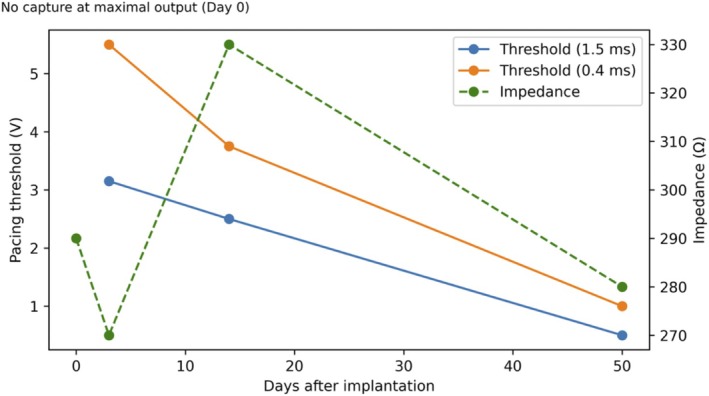 Figure 2
Figure 2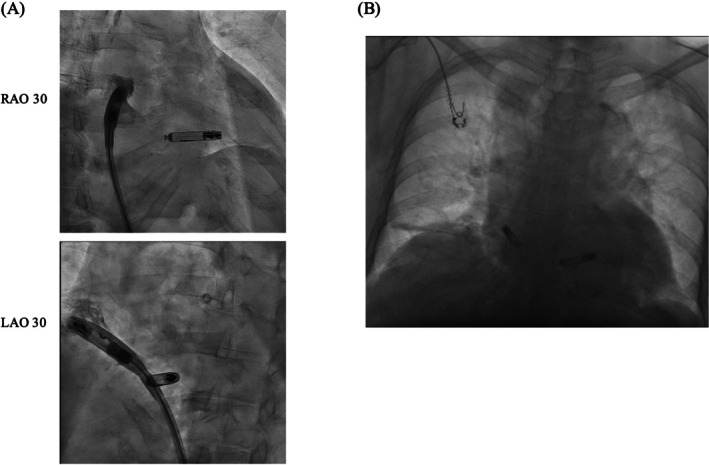 Figure 3
Figure 3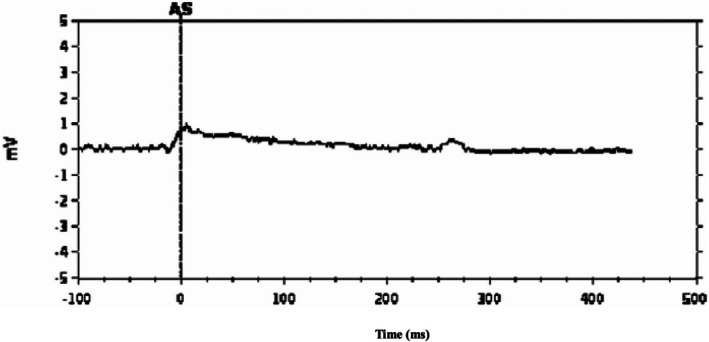 Figure 4
Figure 4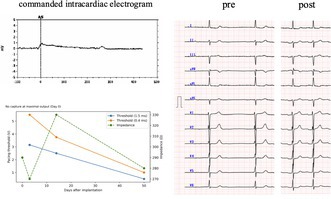 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Cardiac electrophysiology and arrhythmias · Cardiac pacing and defibrillation studies
Transthyretin cardiac amyloidosis (ATTR) is frequently accompanied by conduction abnormalities, including sinus node dysfunction requiring permanent pacing. Dual‐chamber leadless pacemakers provide an option for patients with frailty, infection risk, or limited venous access [1]. During atrial leadless pacemaker implantation, however, elevated acute pacing thresholds or absent atrial capture create uncertainty regarding device stability and repositioning needs.
An 84‐year‐old woman with ATTR amyloidosis presented with recurrent syncope and exertional dyspnea. Cardiac imaging demonstrated diffuse left ventricular hypertrophy with apical sparing, and pyrophosphate scintigraphy showed increased myocardial uptake. Fat aspiration biopsy confirmed amyloid deposition. Ambulatory monitoring revealed profound bradycardia with recurrent asystolic pauses.
Considering the patient's diminished activities of daily living and the need to minimize postoperative mobility demands, we proceeded with implantation of a dual‐chamber leadless pacemaker (Aveir DR, Abbott). Following implantation of the right ventricular device, which exhibited favorable acute electrical parameters (threshold 0.75 V/0.4 ms; impedance 290 Ω), we proceeded with implantation of the atrial leadless pacemaker. The blood pool impedance measured in the inferior vena cava at that time was 260 Ω. Multiple pre‐mapping attempts were performed within the right atrial appendage; however, even at maximal output (6 V/1.5 ms), atrial capture was intermittent, and stable atrial capture could not be achieved. At a pulse width of 0.4 ms, no atrial capture was observed, even at maximal output. Despite the absence of capture, the current of injury (COI) characterized by ST‐segment elevation on the intracardiac electrogram, was clearly present (1 mV), and impedance remained stable (290 Ω; Figure 1).
We considered retrieving the atrial device and proceeding with right ventricular implantation alone. However, isolated right ventricular pacing in patients with sinus node dysfunction has been associated with an increased risk of heart failure [2]. In this patient, the underlying ATTR cardiomyopathy with diastolic dysfunction created conditions in which chronic right ventricular apical pacing would be expected to cause further hemodynamic deterioration. Therefore, following atrial leadless pacemaker implantation, we elected to observe whether the atrial pacing threshold would improve during the chronic phase. After a 30‐min observation period, the atrial pacing threshold remained unchanged; however, the COI and impedance were stable.
Previous reports in atrial leadless pacemaker implantation have shown that a steep increase COI ≧ 2 mV and impedance reflects adequate contact with viable atrial myocardium and is predictive of subsequent improvement in chronic pacing thresholds [3]. In our case, although the magnitude of COI elevation was limited to approximately 1 mV, the increase was steep, and an increase in local impedance relative to the blood pool impedance was observed at the implantation site.
In conventional transvenous pacemaker systems with active‐fixation leads, a sustained positive deflection of the current of injury measured at 80 milliseconds after its onset (CI80) has been shown to reflect secure helix engagement and to predict subsequent improvement in pacing thresholds over the chronic phase, spanning several weeks to months [4]. In our case, CI80 also demonstrated a sustained positive deflection.
Accordingly, the atrial leadless pacemaker was left in situ, with the expectation of potential improvement in chronic‐phase thresholds (Figure 2). By postoperative Day 3, atrial capture appeared (3.0 V/1.5 ms; 5.5 V/0.4 ms). At 2 weeks, the thresholds improved (2.5 V/1.5 ms; 3.0 V/0.4 ms) and the impedance increased to 330 Ω. At 2 months, the thresholds further improved (0.5 V/1.5 ms; 1.0 V/0.4 ms) with impedance stabilizing at 280 Ω (Figure 3). The device was programmed to AAI mode at 50 beats per minute with VVI backup at 40 beats per minute. The patient predominantly maintained sinus rhythm with pacing support during occasional bradycardic episodes (Figure 4). Throughout the 4‐month follow‐up period, she has remained asymptomatic without recurrence of syncope or dyspnea.
This case suggests that even in the absence of acute atrial capture, clearly defined indices based on current of injury and impedance may help predict subsequent chronic improvement. Although acute threshold variations have been reported in leadless systems, this case provides specific insight into the threshold dynamics in ATTR amyloidosis, where initial capture failure may still result in favorable long‐term outcomes when guided by appropriate electrophysiological markers. In atrial leadless systems, acute threshold elevation is common and often improves within 24 h, with further decline over subsequent weeks. Avoiding unnecessary repositioning may reduce procedural risk without compromising long‐term performance. The right atrial appendage has complex and delicate anatomy. Repeated device manipulation in this region carries significant risk, including pericardial effusion and cardiac tamponade. Accurate intraoperative identification of adequate fixation is paramount to minimize unnecessary intervention. In our experience, a minimum observation period of 30 min with stable COI and impedance may be reasonable before considering device retrieval, though the optimal waiting time remains undefined. Criteria that might mandate device retrieval could include absence of COI, declining impedance, or inability to achieve any degree of capture despite repositioning attempts, although standardized guidelines for these decisions are needed. The mechanism underlying the initial absence of capture with subsequent chronic threshold improvement in this patient merits discussion. In cardiac amyloidosis, extracellular amyloid deposition at the electrode‐tissue interface can significantly elevate pacing thresholds. Previous case reports have documented dynamic threshold changes in AL amyloidosis, where threshold elevation correlated with disease activity and improved following systemic chemotherapy [5]. Our patient, however, had ATTR amyloidosis—a progressive condition without definitive treatment. The initial failure to capture likely resulted from acute inflammatory changes at the fixation site superimposed on underlying amyloid infiltration. The subsequent threshold decline over weeks suggests resolution of the acute inflammatory component, despite ongoing amyloid deposition. Whether this improvement will be sustained in the setting of progressive amyloid accumulation remains uncertain, emphasizing the importance of continued threshold surveillance. Development of additional electrophysiological markers predictive of long‐term device performance would strengthen the rationale for deferring acute repositioning in similar cases. Implantation of an atrial leadless pacemaker in patients with ATTR amyloidosis remains controversial, given the potential for elevated atrial pacing thresholds related to atrial myopathy and the additional health care–economic considerations associated with dual‐chamber leadless systems. Although our case suggests that the Aveir DR system can be feasible in carefully selected patients, evidence in this population remains limited. Therefore, further accumulation of similar cases and larger multicenter experience are essential to better define patient selection, expected atrial threshold behavior, and clinical and economic outcomes.
Funding
The authors have nothing to report.
Ethics Statement
The authors have nothing to report.
Consent
Written informed consent for publication was obtained.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1G. Hindricks , R. N. Doshi , P. Defaye , et al., “Six‐Month Electrical Performance of the First Dual‐Chamber Leadless Pacemaker,” Heart Rhythm 21, no. 10 (2024): 1929–1938, 10.1016/j.hrthm.2024.04.091.38697271 · doi ↗ · pubmed ↗
- 2H. R. Andersen , J. C. Nielsen , P. E. Thomsen , et al., “Long‐Term Follow‐Up of Patients From a Randomised Trial of Atrial Versus Ventricular Pacing for Sick‐Sinus Syndrome,” Lancet 350, no. 9086 (1997): 1210–1216, 10.1016/S 0140-6736(97)03425-9.9652562 · doi ↗ · pubmed ↗
- 3P. Neuzil , C. Hubbard , R. N. Doshi , et al., “Implantation Techniques for a Helix‐Fixation Dual‐Chamber Leadless Pacemaker,” Heart Rhythm 21, no. 12 (2024): 2552–2562, 10.1016/j.hrthm.2024.09.053.39343120 · doi ↗ · pubmed ↗
- 4D. P. Redfearn , L. J. Gula , A. D. Krahn , A. C. Skanes , G. J. Klein , and R. Yee , “Current of Injury Predicts Acute Performance of Catheter‐Delivered Active Fixation Pacing Leads,” Pacing and Clinical Electrophysiology 30, no. 12 (2007): 1438–1444, 10.1111/j.1540-8159.2007.00889.x.18070296 · doi ↗ · pubmed ↗
- 5J. C. Martinez , B. Khiatah , S. Jazayeri , K. Z. Oregel , and J. W. Dukes , “Increased Device Thresholds With Subsequent Improvement Status Post‐Systemic Therapy in a Patient With Multiple Myeloma,” Heart Rhythm Case Reports 7, no. 11 (2021): 717–721, 10.1016/j.hrcr.2021.05.005.34820265 PMC 8602117 · doi ↗ · pubmed ↗