One‐Year Outcome of Japanese Patients With Atrial Fibrillation: Insights From APHRS‐AF Registry
Kenji Yodogawa, Yu‐ki Iwasaki, Yasuo Okumura, Koichi Nagashima, Koichi Inoue, Nobuaki Tanaka, Kengo Kusano, Koji Miyamoto, Masahiko Takagi, Kyoko Soejima, Yuichi Momose, Tomohiro Sakamoto, Hideharu Okamatsu, Toyoaki Murohara, Yasuya Inden, Keiichi Fukuda, Seiji Takatsuki

TL;DR
This study analyzed 1-year outcomes of 794 Japanese patients with atrial fibrillation and found low mortality and stroke rates, likely due to high use of anticoagulants.
Contribution
The study provides new insights into the clinical outcomes and treatment patterns of Japanese AF patients from a large, prospective registry.
Findings
One-year all-cause mortality and stroke/thromboembolic events were both 0.1%.
Major bleeding events occurred in 0.7% of patients, including 3 intracranial hemorrhages.
Most patients (57.8%) were planned for catheter ablation, and 81% used oral anticoagulants.
Abstract
The Asia‐Pacific Heart Rhythm Society Atrial Fibrillation (APHRS‐AF) Registry is a prospective study in Asian metropolitan cities, which provides important information on the baseline characteristics, therapeutic patterns, and 1‐year clinical outcomes in patients with atrial fibrillation (AF). This report describes data from Japanese patients recruited in this registry. A total of 4666 patients with AF were enrolled. Of these, 794 patients were recruited from 28 large cardiovascular centers in Japan between 2015 and 2017. We analyzed 1‐year follow‐up outcome of these patients. Mean age at recruitment was 65.7 years and 69.0% were males. Major comorbidities were hypertension (37.5%), lipid disorder (29.0%), heart failure (15.9%), and diabetes mellitus (15.0%). Mean CHADS2 score, CHA2DS2‐VASc score, and HAS‐BLED score were 1.0, 2.0, and 1.1, respectively. At baseline, use of oral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
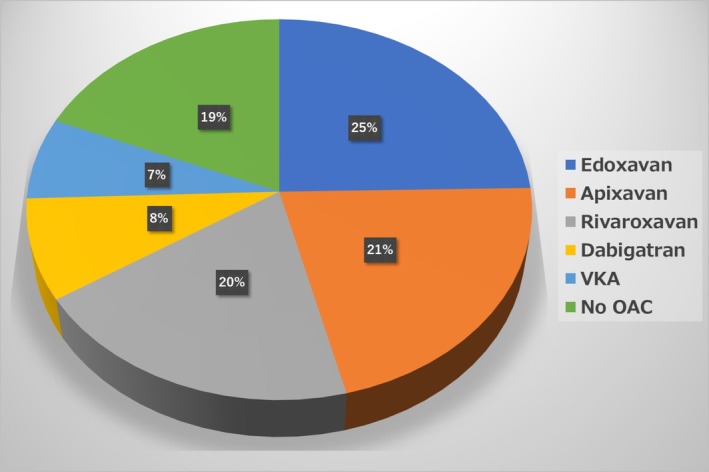 FIGURE 1
FIGURE 1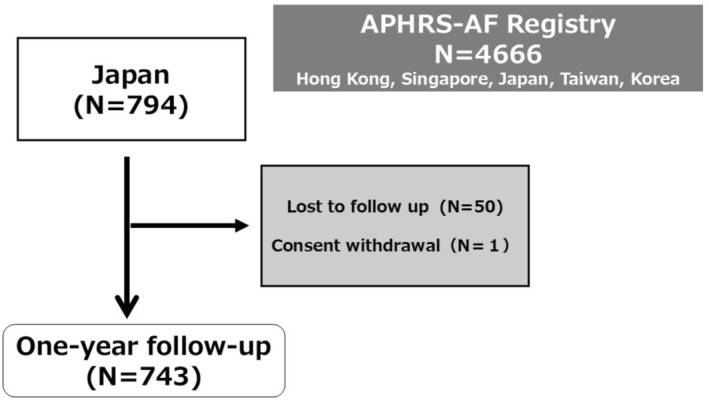 FIGURE 2
FIGURE 2| Baseline characteristics | |
|---|---|
| Age (years) | 65.7 ± 10.8 |
| Male | 548 (69.0%) |
| LAD (mm) | 40.4 ± 7.4 |
| LVEF (%) | 62.3 ± 10.6 |
| HF | 127 (16.0%) |
| HT | 298 (37.5%) |
| DM | 120 (15.1%) |
| Lipid disorder | 230 (29.0%) |
| Stroke/TIA | 46 (5.8%) |
| CAD | 47 (5.9%) |
| CKD | 71 (8.9%) |
| CHADS2 score | 1.0 ± 1.1 |
| CHA2DS2‐VASc score | 2.0 ± 1.6 |
| HAS‐BLED score | 1.1 ± 1.0 |
| First diagnosed AF | 32 (4.0%) |
| Paroxysmal AF | 464 (58.4%) |
| Persistent AF | 213 (26.8%) |
| Longstanding persistent AF | 53 (6.7%) |
| Permanent AF | 32 (4.0%) |
| DOAC | 591 (74.4%) |
| VKA | 55 (6.9%) |
| Antiplatelets | 53 (6.7%) |
| AAD | 123 (15.5%) |
| History of catheter ablation for AF | 200 (25.2%) |
| Planned catheter ablation for AF | 459 (57.8%) |
| Clinical events | Cumulative 1 year (/100 person years) |
|---|---|
| All cause death | 1 (0.1) |
| Cardiac | 1 |
| Others | 0 |
| Nonfatal hospitalization | 157 (21.1) |
| Stroke/thromboembolic events | 1 (0.1) |
| Intracranial bleeding | 3 (0.4) |
| GI bleeding | 1 (0.1) |
| Bleeding in soft tissue, muscle, skin | 1 (0.1) |
| Clinically relevant nonmajor bleeding | 5 (0.7) |
| AF/AFL/AT | 102 (13.7) |
| Arrhythmias other than AF/AFL/AT | 11 (1.5) |
| HF | 4 (0.5) |
| ACS | 2 (0.3) |
| Other cardiovascular events | 6 (0.8) |
| Noncardiovascular events | 21 (2.8) |
| Registry | Japanese APHRS‐AF | APHRS‐AF | Fushimi‐AF | SAKURA‐AF | RYOUMA |
|---|---|---|---|---|---|
| Year | 2015–2017 | 2015–2017 | 2011–2012 | 2013–2015 | 2017–2018 |
| Study population | 28 large cardiovascular centers in Japan | 52 centers in 5 countries with a broad mix oftertiary and general hospitals | 79 institutions including 67 primary‐care clinics in Japan | 2 cardiovascular centers, 13 affiliated or community hospitals, 48 private clinics | Patients with a planned first catheter ablation for AF in 62 institutions |
| Number of patients | 794 | 4664 | 3731 | 3266 | 3072 |
| Age (years) | 65.7 ± 10.8 | 68.5 ± 11.8 | 73.6 ± 11.0 | 72.0 ± 9.4 | 68.0 [60.0–74.0] |
| Male (%) | 69.0 | 65.5 | 59.3 | 74.3 | 71.1 |
| Paroxysmal AF (%) | 58.4 | 42.4 | 49.0 | 37.0 | 64.2 |
| Comorbidities | |||||
| HT (%) | 37.5 | 60.9 | 62.1 | 71.3 | 61.2 |
| Lipid disorder (%) | 29.0 | 37.8 | 43.2 | 38.7 | NA |
| HF (%) | 16.0 | 20.8 | 26.9 | 22.1 | NA |
| DM (%) | 15.1 | 24.2 | 22.9 | 22.8 | 17.3 |
| CKD (%) | 8.9 | 7.6 | 35.2 | 24.6 | 9.6 |
| Prior stroke/TIA (%) | 5.8 | 9.6 | 18.3 | 11.2 | NA |
| CHADS2 score | 1.0 ± 1.1 | NA | 2.0 ± 1.3 | 1.8 ± 1.2 | 1.0 [0.0–2.0] |
| CHA2DS2‐VASc score | 2.0 ± 1.6 | 2.2 ± 1.6 (Males) 3.6 ± 1.6 (Females) | 3.4 ± 1.7 | 2.7 ± 1.4 | 2.0 [1.0–3.0] |
| HAS‐BLED score | 1.1 ± 1.0 | 1.3 ± 1.0 (Males) 1.5 ± 1.0 (Females) | 1.6 ± 0.9 | 1.4 ± 0.9 | 2.0 [1.0–3.0] |
| Oral anticoagulants | |||||
| DOACs (%) | 74.4 | 79.8 | 7.2 | 51.7 | 92.6 |
| VKA (%) | 6.9 | 17.8 | 46.3 | 48.3 | 5.1 |
| Event rate per 100 patient‐years | |||||
| Death | 0.1 | 2.7 | 7.9 | 2.1 | 0.5 |
| Stroke/thromboembolic events | 0.1 | 0.7 | 2.3 | 1.4 | 0.3 |
| Major bleeding | 0.7 | 1.1 | 1.8 | 1.3 | 1.2 |
- —Pfizer10.13039/100004319
- —Bristol‐Myers Squibb10.13039/100002491
- —Heart Rhythm Society10.13039/100005859
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiovascular Disease and Adiposity · Folate and B Vitamins Research
Introduction
1
Atrial fibrillation (AF) is the most common arrhythmia in clinical practice and has been reported to be associated with high morbidity and mortality [1].
However, the management of AF has markedly changed after the introduction of direct oral anticoagulant drugs (DOACs) and catheter ablation as a rhythm control strategy [2].
The Asia‐Pacific Heart Rhythm Society Atrial Fibrillation (APHRS‐AF) Registry is a prospective study in Asian metropolitan cities, which provides important information on the baseline characteristics, therapeutic patterns, and 1‐year clinical outcomes in patients with atrial fibrillation (AF) in the modern era of DOACs and catheter ablation [3]. This report describes data from Japanese patients recruited in this registry.
Methods
2
This is a multicenter prospective observational study. A total of consecutive 4666 in‐ and out‐ patients who presented with AF to a cardiologist were enrolled in five Asian metropolitan cities (Hong Kong, South Korea, Japan, Singapore, and Taiwan). All patients enrolled had an electrocardiogram (ECG) of AF, including Holter, event monitor or implantable loop recorder within the 12 months prior to enrollment. Of these, 794 patients were recruited from 28 large cardiovascular centers in Japan between 2015 and 2017. After baseline assessment at enrolment, 1‐year follow‐up was performed by the local cardiologist investigator. We evaluated mortality, incidence of stroke/thromboembolism, major bleeding, cardiovascular comorbidities, and hospital readmission within 1 year in these Japanese patients. Major bleeding was defined as bleeding causing a drop of Hemoglobin (Hb) > 2 g/L, requiring blood transfusion and/or (lengthening of) hospital admission. This study was approved by our local Ethical Committee (28–06‐594), and informed consent was obtained from all patients.
Statistical Analysis
2.1
Continuous variables were presented as mean value ± standard deviation (SD), and categorical variables were summarized as count and percentage. Kaplan–Meier analysis was used to determine 1‐year all‐cause mortality, stroke/thromboembolic events rate, and major bleeding events rate. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan) [4].
Results
3
Baseline Characteristics
3.1
Mean age at recruitment was 65.7 years and 69.0% were males. Major comorbidities were hypertension (37.5%), lipid disorder (29.0%), heart failure (16.0%) and diabetes mellitus (15.0%). Mean CHADS2 score, CHA2DS2‐VASc score, and HAS‐BLED score was 1.0, 2.0, and 1.1, respectively. Paroxysmal AF was detected in 464 patients (58.4%), persistent AF in 213 (26.8%), long‐standing AF in 53 (6.7%), permanent AF in 32 (4.0%), and first diagnosed AF in 32 (4.0%) (Table 1). Notably, majority of the patients (N = 459, 57.8%) were planned to undergo catheter ablation, and it was performed during the hospitalization following enrollment in 362 (45.6%) patients. At baseline, use of oral anticoagulants was 81%, including 7% prescribed a vitamin K antagonist (VKA) and 74% a direct oral anticoagulant (DOAC) (Figure 1).
Distribution of oral anticoagulants (OACs) in the study population. VKA, vitamin K antagonist.
One‐Year Follow‐Up Outcome
3.2
One‐year follow‐up was conducted in 743 patients (lost to follow up; N = 50, consent withdrawal; N = 1, Figure 2). One‐year all‐cause mortality was 0.1% (n = 1, heart failure), and the incidence of stroke/thromboembolic events was also 0.1% (n = 1, pulmonary embolism). The patient with pulmonary embolism was not taking anticoagulation at the time of the event. Major bleeding event rates were 0.7% (n = 5, 3 intracranial hemorrhages, 1 lower gastrointestinal bleeding, 1 soft tissue bleeding). One patient with major bleeding was not taking anticoagulation at the time of the event, and the remaining 4 patients were taking DOAC. Clinically relevant nonmajor bleeding was observed in 5 (0.7%) patients. A total of 157 (21.1%) nonfatal hospitalizations were observed. The major causes of hospitalizations were AF, atrial flutter (AFL), or atrial tachycardia (AT) (n = 102, 13.7%) (Table 2).
Patient flow of the study.
Discussion
4
The present study demonstrated an extremely low mortality rate in patients with AF recruited in this registry. The incidence of stroke/thromboembolic events was also extremely low. In addition, a low incidence of major bleeding was observed.
Comparison With the Other Japanese Registries
4.1
The present registry demonstrated lower mortality (0.1%/year), lower incidence of stroke/thromboembolic events and bleeding events (0.1%, 0.7%, respectively) compared to those in previous Japanese AF registries. The Fushimi AF Registry, the large database of Japanese AF patients, showed 7.9% annual mortality rate. Annual incidence of stroke or systemic embolism and major bleeding were 2.7%, 1.5%, respectively. However, The Fushimi AF Registry is a community‐based cohort, whereas the Japanese APHRS‐AF Registry is cardiovascular center‐based cohort. Discrepancies in the mortality rate, incidence rates are assumed to be derived from differences in patient background. Mean age was higher than that of the present registry (73.6 vs. 65.7 years). Notably, nearly half of the patients were not taking oral anticoagulants (Table 3) [5, 6].
SAKURA AF Registry is a recent prospective observational registry in patients with documented AF being treated with anticoagulants. In total, 3266 patients were enrolled at 2 university hospitals, 13 affiliated or community hospitals, and 48 private clinics between September 2013 and December 2015. In this registry, annual mortality rate was 0.64%, and annual incidence of stroke or systemic embolism and major bleeding were 1.17%, 1.21%, respectively [7, 8]. These incidences were higher than those in our registry, and this may also be due to differences in patient background. Mean age was higher than that of the present registry (72.0 vs. 65.7 years), and a higher proportion of patients had hypertension compared with our study (71.3% vs. 37.5%) (Table 3).
On the other hand, in Japanese patient cohorts like those in the APHRS‐AF registry—who were relatively young, had low CHADS2 scores, and few comorbidities such as hypertension and were scheduled for catheter ablation at large cardiovascular centers—short‐term prognosis was found to be extremely favorable.
RYOUMA registry is a prospective multicenter observational study of Japanese patients who underwent catheter ablation for AF in 2017–2018. The incidence of thromboembolic and major bleeding events for 1 year was 0.3% and 1.2%, which were nearly consistent with those in the present study [9].
Comparison With the APHRS AF Registry Including 5 Countries
4.2
In comparison with the whole APHRS‐AF Registry [3], we observed an overall lower mortality rate (0.1% vs. 2.7%). The reasons remain unclear because non cardiovascular rather than cardiovascular events were the most common causes of mortality in the whole APHRS‐AF Registry. However, it might be partially attributed to the younger population (65.7 ± 10.8 vs. 68.5 ± 11.8 years) in Japanese APHRS‐AF Registry. Moreover, Japanese APHRS‐AF Registry showed lower proportion of heart failure (16.0% vs. 21.2%) and coronary artery disease (5.9% vs. 19.5%) compared to those in whole APHRS‐AF Registry [10], which also might attribute to the lower mortality. Furthermore, Bucci et al. recently reported that diabetes mellitus (DM) was independently associated with a higher risk of all‐cause death, cardiovascular death, and major bleeding in the whole APHRS‐AF Registry. Our registry showed lower proportion of DM compared to those in the whole APHRS‐AF Registry (15.1% vs. 24.6%), which might affect the mortality [11]. The Japanese APHRS‐AF Registry demonstrated lower incidence of stroke/thromboembolic events and bleeding events compared to those in whole APHRS‐AF Registry (0.1% vs. 0.7%, 0.7% vs. 1.7%, respectively). While the reasons remain unclear, it is possibly influenced by the lower CHA2DS2‐VAScscore and HAS‐BLED score in the Japanese APHRS‐AF Registry compared to those in whole APHRS‐AF Registry [11].
Recently, Chao TF et al. described that significant differences of clinical features were noted between countries in APHRS‐AF Registry. The mean age of AF patients in Hong Kong was 73.59 years compared to 65.80 years in Japan. In addition, the comorbidities were diverse, with the highest CHA2DS2‐VASc scores reported from Hong Kong (mean 3.5) and lowest in Japan (mean 2.0). The HAS‐BLED score showed significant variation, with the highest mean in Hong Kong (1.8) and the lowest in Japan (1.1) [12]. These differences in profiles of patients enrolled by cardiologists at medical centers may contribute to the low mortality and low incidence of stroke/thromboembolic events in Japan.
Study Limitations
5
There are limitations in this study. First, this cohort was followed by electrophysiologists with a high proportion of patients undergoing catheter ablation (57.8%), which limits generalizability to the broader Japanese AF population. This might partly account for the low mortality and low incidence of stroke/thromboembolic events and bleeding events. Second, about 6% of our patients were lost to follow‐up. However, this value is lower than the 12% observed in the whole APHRS‐AF Registry [3]. Third, similar to the whole APHRS‐AF Registry, we did not have data on International Normalized Ratio (INR) control in our patients treated with VKA [3]. Therefore, it remains unclear whether the INR control in patients treated with VKA affected their outcomes. However, we did not observe any significant thromboembolic or bleeding events among those treated with VKA.
Conclusions
6
In this registry from large cardiovascular centers, the majority of the patients were planned to undergo catheter ablation, and a high prevalence of oral anticoagulant use was recorded. A low mortality rate and low incidence of stroke/thromboembolic events were observed in Japanese patients of the APHRS‐AF Registry. However, the findings are limited by focusing on large cardiovascular centers, which may not fully reflect the broader Japanese AF population. Future studies with extended follow‐up durations including both private and public sector patients are warranted to validate these insights into AF management in Japan.
Funding
This study was an independent research grant by Pfizer and Bristol Myers Squibb (BMS) to Asia‐Pacific Heart Rhythm Society.
Ethics Statement
This study was approved by the institutional ethics committee of Nippon Medical School (Approval No. 28‐06‐594). Informed consent was taken from patients.
Conflicts of Interest
Yasuo Okumura has received research funding from Medtronic Japan Co. Ltd., MicroPort CRM Japan, and Bayer Healthcare; and has accepted remuneration from AstraZeneca K.K. and Johnson & Johnson K.K. He is affiliated with endowed departments supported by Abbott Japan LLC, Boston Scientific Japan K.K., Medtronic Japan Co. Ltd., Japan Lifeline Co. Ltd., and Biotronik Japan. Koichi Nagashima has received speaker honoraria from Johnson & Johnson and Medtronic Japan. Koichi Inoue has received remuneration from DAIICHI SANKYO COMPANY Ltd., Medtronic, Boston Scientific, and Bristol Myers Squibb. K. Nobuaki Tanaka has received Honorarium from Bayer, Johnson & Johnson K.K., Nippon Boehringer Ingelheim Co. Ltd., AstraZeneca K.K. and Medtronic Japan Co. Ltd. Kengo Kusano has received speaker honoraria from DAIICHI SANKYO COMPANY Ltd., and Medtronic Japan, and research grants from Medtronic Japan, Abott Japan, Boston Scientific Japan, Biotronik Japan, GE Precision Healthcare LLC, Johnson & Johnson K.K. and JSR. Koji Miyamoto has received funding/grants from Bristol‐Myers Squibb, Medtronic, Biosense Webster, Abbott, and Boston and honoraria/speakers' bureaus from Medtronic, Biosense Webster, Abbott and Boston outside the submitted work, and is affiliated with a department endowed by Medtronic outside the submitted work. Masahiko Takagi has received speaker honoraria from DAIICHI SANKYO COMPANY Ltd., Biotronik Japan, Japan Lifeline Co. Ltd., and Medtronic Japan, and research grants from Japan Lifeline Co. Ltd. and Abott Japan. Kyoko Soejima has received speaker honoraria from Abott Japan and Medtronic Japan. Toyoaki Murohara received lecture fee from Boehringer Ingelheim Japan, AstraZeneca, Viatris, Kowa, Novartis Pharma. He is a member of Circulation Journal's Editorial Board. Seiji Takatsuki belongs to Advanced Cardiac Arrhythmia Therapeutics Endowed Research Course, which is supported by Medtronic Japan, Japan Lifeline, Boston Scientific Japan, Abbott Japan and Biotronik Japan. He has received lecture fees from Medtronic Japan, Japan Lifeline, DAIICHI SANKYO COMPANY Ltd., Boston Scientific Japan, Abbott Japan. Keiichi Fukuda holds shares of Heartseed Inc., and has received remuneration from the company. Yukiko Nakano is a member of Circulation Journal's Editorial Board. Teiichi Yamane has received speaker honoraria from Medtronic Japan and BEG company, and research grants from Japan Lifeline. Michifumi Tokuda has received honoraria from Medtronic Japan, and research grants from Japan Lifeline. Hiroyuki Osanai has received honoraria from DAIICHI SANKYO COMPANY Ltd. Kazuhiro Satomi has received lecture fee from DAIICHI SANKYO COMPANY Ltd. Eiichi Watanabe has received consulting fee from Fukuda Denshi. Naohiko Takahashi has received remuneration from DAIICHI SANKYO COMPANY Ltd., AstraZeneca, Bayer, Boehringer Ingelheim Japan, TOA EIYO LTD., Otsuka Pharmaceutical Co. Ltd., Novartis Pharma, Bristol‐Myers Squibb, Pfizer Inc., and Medtronic. He is a member of Circulation Journal's Editorial Board. Hirofumi Tomita is a concurrent professor of an endowment department supported by Medtronic Japan Co. Ltd. and Boston Scientific Japan Co. Ltd. He has received a speakers' bureau/honorarium from Bayer, Daiichi‐Sankyo, and Bristol‐Myers Squibb. Hiroshi Tada received honoraria for lectures or speakers bureaus from DAIICHI SANKYO COMPANY Ltd.; Novartis Pharma K.K.; Medtronic Japan Co. Ltd., BIOTRONIK Japan Inc., Bristol Myers Squibb, Boston Scientific Japan K.K. He has received grants (Investigator‐initiated study unrelated to the manuscript topic) from Abbott Medical Japan LLC, DAIICHI SANKYO COMPANY Ltd., Nippon Boehringer Ingelheim Co. Ltd.; Otsuka Pharmaceutical Co. Ltd.; Eli Lilly Japan K.K.; Marubun Tsusyo K.K. He is a member of Circulation Journal's Editorial Board. Yukihiro Koretsune has received speaker honoraria from DAIICHI SANKYO COMPANY Ltd. Masahiko Goya has received lecture fee from Johnson & Johnson, Japan Lifeline and Abbott Medical Japan. Wataru Shimizu has received remuneration from Daiichi Sankyo, Boehringer‐Ingelheim, Pfizer, Bristol‐Myers Squibb, Janssen, Johnson & Johnson, Boston Scientific, Japan Life Line, Abbott Japan, and Medtronic Japan. He is a member of Circulation Journal's Editorial Board.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1E. J. Benjamin , P. A. Wolf , R. B. D'Agostino , H. Silbershatz , W. B. Kannel , and D. Levy , “Impact of Atrial Fibrillation on the Risk of Death: The Framingham Heart Study,” Circulation 98 (1998): 946–952.9737513 10.1161/01.cir.98.10.946 · doi ↗ · pubmed ↗
- 2G. Hindricks , T. Potpara , N. Dagres , et al., “2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration With the European Association for Cardio‐Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed With the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC,” European Heart Journal 42 (2021): 373–498.32860505 10.1093/eurh · doi ↗ · pubmed ↗
- 3H. F. Tse , W. S. Teo , C. W. Siu , et al., “Prognosis and Treatment of Atrial Fibrillation in Asian Cities: 1‐Year Review of the Asia‐Pacific Heart Rhythm Society Atrial Fibrillation Registry,” Europace 24 (2022): 1889–1898.35025986 10.1093/europace/euab 327 · doi ↗ · pubmed ↗
- 4Y. Kanda , “Investigation of the Freely Available Easy‐Touse Software ‘EZR’ for Medical Statistics,” Bone Marrow Transplantation 48 (2013): 452–458.23208313 10.1038/bmt.2012.244PMC 3590441 · doi ↗ · pubmed ↗
- 5M. Akao , Y. H. Chun , M. Esato , et al., “Inappropriate Use of Oral Anticoagulants for Patients With Atrial Fibrillation,” Circulation Journal 78 (2014): 2166–2172.24976391 10.1253/circj.cj-14-0344 · doi ↗ · pubmed ↗
- 6Y. Yamashita , R. Uozumi , Y. Hamatani , et al., “Current Status and Outcomes of Direct Oral Anticoagulant Use in Real‐World Atrial Fibrillation Patients—Fushimi AF Registry,” Circulation Journal 81 (2017): 1278–1285.28428449 10.1253/circj.CJ-16-1337 · doi ↗ · pubmed ↗
- 7Y. Okumura , K. Yokoyama , N. Matsumoto , et al., “Current Use of Direct Oral Anticoagulants for Atrial Fibrillation in Japan: Findings From the SAKURA AF Registry,” Journal of Arrhythmia 33 (2017): 289–296.28765759 10.1016/j.joa.2016.11.003PMC 5529323 · doi ↗ · pubmed ↗
- 8Y. Yuzawa , K. Kuronuma , Y. Okumura , et al., “Relationship Between the Renal Function and Adverse Clinical Events in Patients With Atrial Fibrillation: A Japanese Multicenter Registry Substudy,” Journal of Clinical Medicine 9 (2020): 167.31936260 10.3390/jcm 9010167 PMC 7019418 · doi ↗ · pubmed ↗