Prevalence and risk factors associated with adverse birth outcome in Ethiopia: systematic review and meta-analysis
Teka Girma, Dessalegn Wirtu, Gudina Egata, Jote Markos

TL;DR
This study finds that adverse birth outcomes are common in Ethiopia, with risk factors including lack of prenatal care and rural residency.
Contribution
The study provides a comprehensive meta-analysis of adverse birth outcomes and their risk factors in Ethiopia.
Findings
The overall pooled prevalence of adverse fetal outcomes in Ethiopia was 28%.
Low birth weight and preterm birth were the most common adverse outcomes.
Rural residency and lack of antenatal care were major risk factors.
Abstract
Adverse pregnancy outcomes represent a major public health challenge in developed and resource-limited countries. Globally, approximately 60–80% of neonatal deaths occur in low birth weight infants, and more than 2 million infants die before birth each year and the burden of the problem is significant in Ethiopia. Therefore, the aim of this study was to determine the combined incidence and risk factors for poor birth outcomes in Ethiopia. International databases (PubMed, Google scholar, web of science and scopus) were searched. A funnel plot and Begg test were used to see the publication bias. The heterogeneity of studies was checked using I-square statistics with a cut of point 75% and the Newcastle Ottawa (NCO) quality assessment tool was applied to ensure the quality of the included articles. A random-effect model was applied to pool the adverse birth outcome. The sub-group analysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
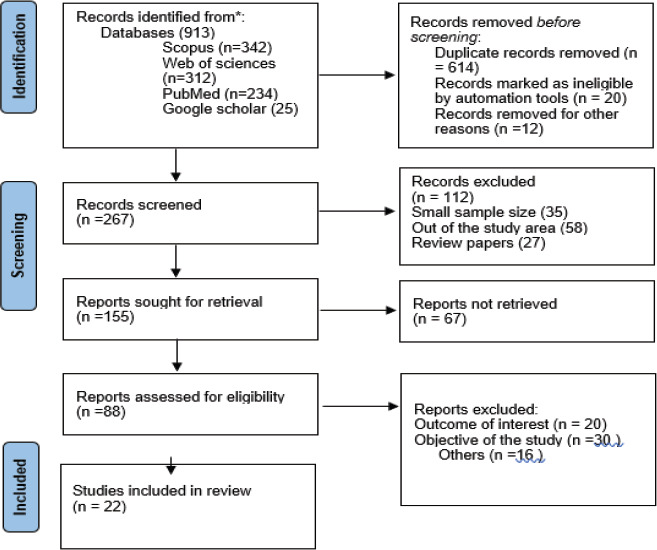 Figure 1
Figure 1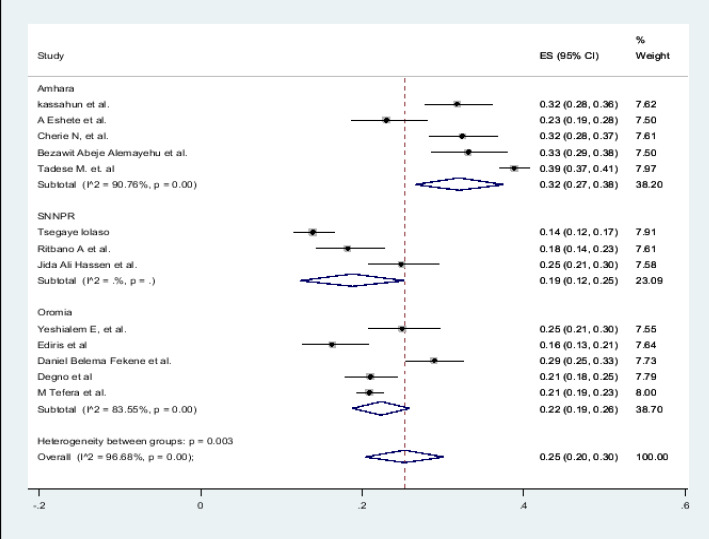 Figure 2
Figure 2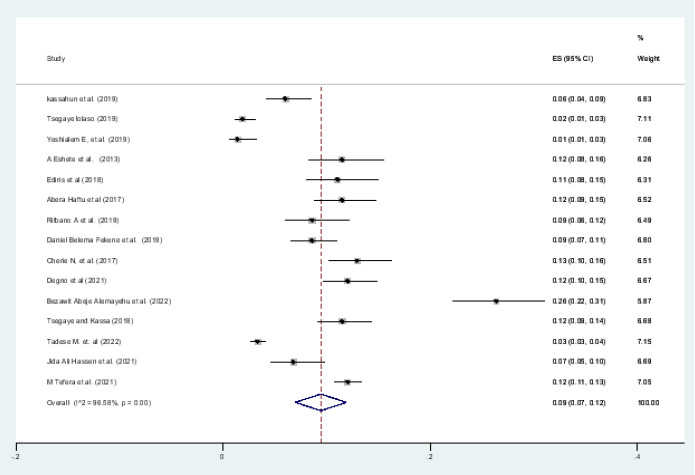 Figure 3
Figure 3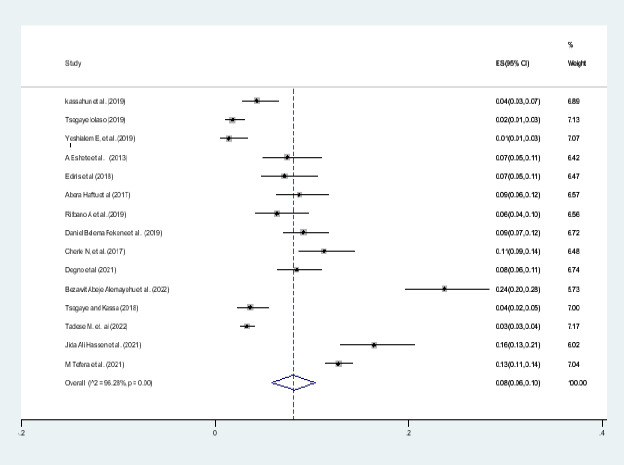 Figure 4
Figure 4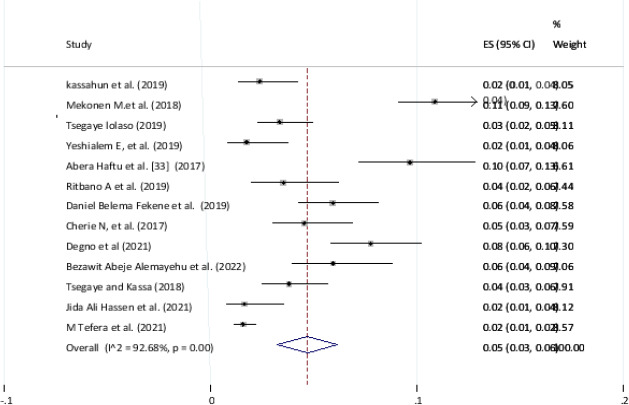 Figure 5
Figure 5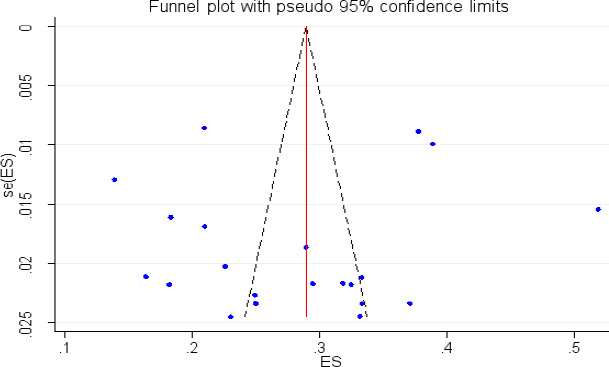 Figure 6
Figure 6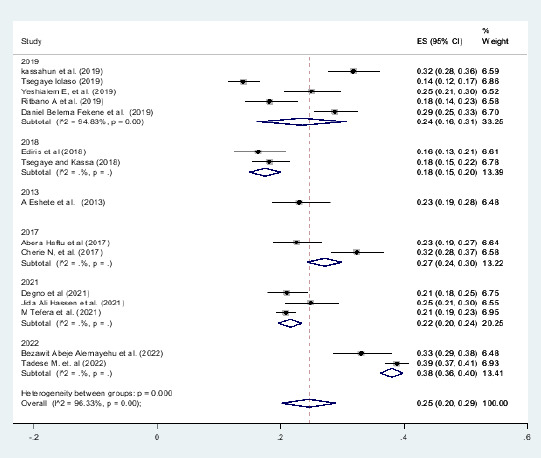 Figure 7
Figure 7| 3 | Mekonen M. et al. | 2018 | Somali | Fafan | 545 | crossectiona | 1050 | 51.9 | preterm birth, congenital defect |
|---|---|---|---|---|---|---|---|---|---|
|
| Tsegaye lolaso | 2019 | SNNPR | Kembata | 100 | crossectional | 718 | 13.928 | preterm, LBW, still birth |
|
| Yeshialem E, et al. | 2019 | Oromia | Jimma | 86 | case control | 344 | preterm, still birth, low birth weight | |
|
| A Eshete et al. | 2013 | Amhara | North wollo | 68 | cross sectional | 295 | 23.051 | Preterm birth, LBW, Stillbirth & congenital defect |
|
| Ediris et al | 2018 | Oromia | Shashemene | 50 | cross sectional | 306 | 34.967 | PPH, hypertensive disorder |
|
| Abera Haftu et al. |
| Tigray | Shire | 96 | cross sectional | 425 | 22.588 | Preterm birth, LBW, Stillbirth Low |
|
| Abebe Eyowas et al. | 2017 | Amhara | Bahirdar | 1135 | cross sectional | 3003 | 37.8 | Preterm birth, LBW, Stillbirth Low |
|
| Ritbano A et al. | 2019 | SNNPR | Butakira | 57 | Crosssectional | 313 | 18.2 | LBW, preterm, still birth, visible congenital anomalies |
|
| Daniel Belema F et al. | 2019 | Oromia | west shoa | 171 | case control | 591 | preterm, LBW, still birth | |
|
| Feleke G meskel | 2016 | SNNPR | Gamogofa | 158 | case control | 426 | preterm, LBW, still birth, congental anomalies | |
|
| Cherie N, et al. | 2017 | Amhara | Desse | 150 | crossectiona | 462 | 32.5 | preterm, LBW, still birth |
|
| Hailemichael et al | 2020 | Tigray | Tigray | 135 | case control | 405 | preterm, LBW, still birth | |
|
| Degno et al | 2021 | Oromia | Bale | 122 | crossectiona | 580 | 21 | preterm, low birth weight, still birth, congenital anormalies |
|
| Bezawit Abeje Alem et al. | 2022 | Amhara | Bahirdar | 123 | crossectiona | 371 | 33.2 | LBW, preterm birth, stillbirth, and had visible birth defects |
|
| Tsegaye and Kassa |
| Sidama | Awassa | 106 | crossectiona | 580 | 18.3 | perinatal death, preterm birth, macrosmia, low birth weight |
|
| Tadese M. et. al | 2022 | Amhara | Debrebrihan | 941 | crossectiona | 2418 | 28.3 | perinatal death, stii birth, malpresentation, lowbirth weight |
|
| Jida Ali Hassen et al. | 2021 | SNNPR | 91 | case control | 365 | preterm, Low birth weight | ||
|
| D. Addisu et al. | 2021 | Amhara | south Gonder | 130 | case control | 441 | preterm, low birth weight | |
|
| Abadiga et al. | 22 | Oromia | west Ethiopia | 165 | case-control | 495 | Adverse birth outcome | |
|
| M Tefera et al. | 2021 | Dirre, oromia, harari | 471 | follow up | 2246 | 20.97 | Adverse birth outcome |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Preterm Birth and Chorioamnionitis · Maternal and Perinatal Health Interventions
Introduction
Adverse birth outcome which attributes to most perinatal deaths is an important indicator of child health and survival. Millions of newborns worldwide are affected by unfavourable birth outcomes. Each year, preterm delivery causes one million newborn deaths1,2. Every year, an estimated 15 million babies are born before 37 weeks of pregnancy. In Africa and South Asia, premature births account for more than 60% of all births3. Low birth weight (LBW), which is estimated to account for 15% to 20% of all births globally4, continues to be a critical public health issue, with the majority of these deaths taking place in sub-Saharan Africa1,5,6. Pregnancy and its related problems contribute to a significant proportion of reproductive mortality with maternal mortality is unacceptably high.
In Ethiopia, the burden of poor birth outcomes is significant7. Every year, about 320,000 infants are delivered before 37 weeks of pregnancy1. In 2014, there were 27,243 fatalities attributable to LBW, making up 4.53 percent of all fatalities8. Recent researches from various regions of the nation indicate that between 18.2% and 32.5 percent of births in Ethiopia result in unfavourable outcomes. 15–18 LBW and stillbirth are the most typical types of poor delivery outcomes9,10. Induced labor, hypertensive disorders of pregnancy, antepartum hemorrhage, premature rupture of membranes, prior poor obstetric history, multiple pregnancies, multigravida, insufficient antenatal care (ANC), hemoglobin level 11 g/dL, rural residence, and malaria infection during pregnancy are all significantly linked to poor birth outcomes, according to a number of studies9-13.
Premature birth and low birth weight (LBW) are consequential factors that kick in to perinatal and neontal mortality and have negative longterm health backwash for survivors, especially in low- and middle-income countries (LMICs)14,15. Although adverse birth outcomes and their consequences are preventable14,16,17, they are particularly common in low- and middle-income countries. This means that a significant proportion of infant mortality is due to premature births. 15.4% of the 6 estimated. The three million children less than 59 months who died in 2013 were due to complications related to premature birth. The most common cause of death in newborns (death within the first 28 days of life) is premature birth14. Likewise, the risk of postnatal and perinatal mortality (stillbirths and newborns) is higher in children with low birth weight15.
Having the burden of adverse birth outcomes and key risk factors will provide policy makers and healthcare practitioners working in the region with evidence that can be used to inform strategies to achieve reductions in adverse birth outcomes and improve overall perinatal health. These research findings will help to design targeted interventions and better allocate resources to where they are needed. Additionally, findings of the review will inform future etiological research on the effect of risk factors of adverse birth outcomes in the region
Methods
This systematic review and meta-analysis was conducted to estimate the pooled prevalence of adverse fetal outcomes, the most common magnitude of adverse fetal outcomes and associated factors in Ethiopia using the standard PRISMA checklist guideline (Fig 1.)
PRISMA flow diagram on adverse pregnancy outcome in Ethiopia, 202214
Reporting
This systematic review and meta-analysis was designated to estimate the pooled prevalence of adverse birth outcomes and associated factors among pregnant women in Ethiopia. The result is reported based on standard Preferred Reporting Items for Systematic review and Meta-analysis (PRISMA) checklist15. The review protocol was submitted for registration in the international prospective register of systematic reviews (PROSPERO) and registered with PROSPERO registration number (PROSPERO 2022: CRD42022327072)
Database and search strategy
International databases which are Pub Med, Google Scholar, Web of Science, Scopus and different gray pieces of literature and articles published in the university online repository were included. Core searching terms were used using PICO formulating questions. These were: “newborn”, “adverse birth outcome”, “fetal outcome”, “stillbirth”, “low birth weight”, “neonate”, “prematurity”, and “congenital anomaly, congenital defect”, “preterm”, “preterm birth”. “Ethiopia”. The following Searching terms were applied: neonate OR newborn OR women OR infant OR child OR children AND “abnormal birth weight” OR “congenital defect” OR “congenital anomaly” OR “stillbirth” OR “prematurity” OR “preterm birth” OR “low birth weight” OR “perinatal” OR “neonatal death” OR “preterm” AND Ethiopia and related terms. The search strategy has been employed from June 3/2022-June30/2022.
Research question
What is the pooled prevalence of adverse pregnancy out come in Ethiopia? Which adverse birth outcomes are common in Ethiopia? What are the factors affecting the adverse birth outcome in the area?
Study selection
Initially, all articles were exported into Endnote version 9 software and checked for duplication. The duplicated articles were removed. Two independent authors, TG and MB, have reviewed the title and abstract. Three authors; DW, GE, and TG have scanned the abstracts and full documents. The disagreement was handled based on established article selection criteria.
Inclusion and exclusion criteria
Twenty two Observational studies (case-control, cross-sectional and follow up study) which were previously published were included in this systematic review and meta-analysis. Articles reported the prevalence or/and a minimum of one contributing factor for adverse fetal outcomes is included. Only English language literature and research articles were included. Whereas, articles without full abstracts or texts and articles reported out of the outcome interest were excluded.
Quality assessment
Two authors (TG & GE) independently assessed the quality of each study using the Newcastle-Ottawa quality assessment (NOQA) form was used. Any disagreement was resolved by the hindrance of the third reviewer (MB). The following NOQA items used to appraise case-control studies were: [1] comparable groups, [2] appropriateness of cases and controls, [3] criteria to identify cases and controls, [4] standard measurement of exposure, [5] similarity in the measurement of exposure for cases and controls, [6] handling of confounder [7], strategies to handle confounder, [8] standard assessment of outcome, [9] appropriateness of duration for exposure, and [10] appropriateness of statistical analysis. Items used to appraise cross-sectional studies are: [1] inclusion criteria, [2] description of study subject and setting, [3] valid and reliable measurement of exposure, [4] objective and standard criteria used, [5] identification of confounder, [6] strategies to handle confounder, [7] outcome measurement, and [8] appropriate statistical analysis. Therefore to consider the studies have low risk, the value should be 50% and above the quality assessment indicators
Data extraction
After collecting findings from the entire database, the articles were transferred from Endnote version X9 software to the Microsoft Excel spreadsheet to remove duplicated studies. Two authors (TG and GE) independently extracted all the important data using a standardized Newcastle Ottawa data extraction format. Any disagreement between reviewers was resolved by the third reviewer (DW) through discussion and consensus. The name of the author, sample size, publication year, study area, region, the overall prevalence of ad outcome with its outcome categories with 95%CI and associated factors were collected. The reviewer contacted the corresponding author(s) for further information whenever pertinent data were missed from the included studies.
Statistical analysis
Publication bias was checked using the funnel plot and Egger's regression test16. The heterogeneity of studies also computed using the Cochrane Q-test and I-squared statistic17,18. Pooled analysis was conducted using a weighted inverse variance random-effects model19. Subgroup analysis was also conducted using the study region and year of publication. STATA version 14 statistical software. Forest plot format was used to present the pooled point prevalence with 95%Cl. For associations, a log odds ratio was used to decide the association between associated factors and adverse birth outcomes (Figure 1).
Result
Characteristics of the included studies
A search approach that considered adverse pregnancy outcomes and related factors in Ethiopia yielded 913 publications in PubMed, Google Scholar, Scopus, an academic website, and other gray literature sources. After removing duplicates, two hundred sixty seven (267) studies remained. As a result, 155 full-text publications were retrieved and the inclusion criteria checked, leading to the removal of a further 88 articles, mainly for pragmatic reasons. Twenty-two studies eventually qualified for inclusion in the final systematic review and meta-analysis (Table 1)
The included researches were from Oromia, Amhara, sidama, SNNPR (South Nation Nationalities people and representatives), Tigray, Somali, and Addis Ababa, among other regions of Ethiopia. Finally, this systematic review and meta-analysis included 22 papers, with a total of 16636 study participants. Among the included researches fifteen (15) were cross-sectional studies and 6 case-control studies and one study was follow up study design.
The author's name, year of publication, outcome of interest, total number of study participants, prevalence/proportion, and study area from the original studies were all included (Table 1). Amhara region was the one that report the high number of research papers, whereas the Somali and Sidama regions had the fewest that included in this systematic review and meta-analysis. Sidama is the newly emerged region in the country which was previously part of South Nation Nationalities people and representatives.
Prevalence of Adverse pregnancy outcomes in Ethiopia
In the present systematic review and Meta-analysis drew on 22 studies, totaling 16636 study populations. A forest plot depicts the overall pooled prevalence of adverse fetal outcomes (Fig. 2). Despite the fact that the pooled estimated prevalence of adverse birth outcomes in Ethiopia was 25 percent (95 percent CI; 20-29; I2 = 96.00 percent, Pv= 0.001), the magnitude of each adverse neonatal outcome is as follows: low birth weight (9 percent), preterm birth (8 percent) and stillbirth (5 percent).
Forest pilot of the pooled prevalence of adverse birth outcome in Ethiopia, 2022
Pooled meta-analysis of different adverse fetal outcomes categories in Ethiopia
Pooled prevalence of low birth weight
A forest plot depicts the quantified prevalence of low birth weight (Fig. 3). The overall pooled prevalence of low birth weight was 9 percent (95 percent CI: 7.0-12.0; I2= 96.58 percent, pv= 0.001). The included studies in this systematic review and meta-analysis were markedly heterogeneous since I2 was 96.66%
Forest pilot of the pooled prevalence of adverse birth outcome (Low birth weight) in Ethiopia, 2022
Pooled prevalence of preterm birth
A forest plot depicts the quantified prevalence of preterm birth (Fig. 4). The overall pooled prevalence of preterm was 8 percent (95 percent confidence interval: 6.0-10; I2= 96. percent, pv= 0.001). The included studies in this systematic review and meta-analysis were markedly heterogeneous.
Forest pilot of the pooled prevalence of adverse birth outcome (preterm) in Ethiopia, 2022
Pooled prevalence of still birth in Ethiopia
The estimated prevalence of fetal death is presented in a forest plot (Fig. 5). The overall pooled prevalence of fetal death was 5 (95% CI; 3–6; I2 = 92.68%, p < 0.001). In this systematic review and meta-analysis, the included studies were characterized by marked heterogeneity (I2 = 92.68%, p < 0.001).
Forest pilot of the pooled prevalence of adverse birth outcome (still birth) in Ethiopia, 2022
Publication bias
A funnel plot was assessed for asymmetry distribution of adverse fetal outcomes by visual inspection and it was difficult to decide he presence of publication bias (Fig. 6). Unfortunately the Egger's regression test showed with a p-value of 0.35 showed that the presence of publication bias. Furthermore, low publication bias was detected using Egger's tests with a p-value of 0.03.
Funnel plot to show publication bias on adverse birth outcome in Ethiopia, 2022
Factors associated with adverse birth pregnancy outcome in Ethiopia
Multiple pregnancies, being anemic/Hgb level less than 11g/dl, having pregnancy complication during the current pregnancy, rural residency, lack of antenatal care follow-up, and advanced maternal age (greater than 35 years) were factors for adverse fetal outcomes in this systematic review and meta-analysis.
Women who had multiple pregnancies were about 5.8 times more likely to have an adverse birth outcome than mothers who had a single pregnancy (AOR 5.79 percent CI 1.11-10.48)
When compared to those who had a full ANC visit, pregnant women who did not have antenatal care follow-up to a health facility were 2.6 times more likely to have a negative fetal outcome (AOR=2.63; 95 percent CI: 1.44-3.81). Women who had current pregnancy complications (AOR=2.52; 95 percent CI:1.62-3.42) were nearly 2.5 times more likely to have an adverse fetal outcome than women who did not have current pregnancy complications.
Women in rural residency (AOR=2.09; 95 percent CI: 1.43-2.65), Women who lived in rural area were 2.3 times more likely to have a negative fetal outcome. The probability of developing adverse birth outcome for women whose their age was greater than 35 was about 2 times more when compared to their counter parts age less than 35.
Subgroup analysis
Subgroup analysis was employed with the evidence of heterogeneity. Therefore subgroup analysis was done by publication year and by region of Ethiopia and determinant factor. Hence the Cochrane I2 statistic =96.68%, P < 0.003) with evidence of marked heterogeneity between regions and Cochrane I2 statistic =96.33%, P < 0.001) with evidence of marked heterogeneity between years of publications (Fig 7).
subgroup analysis by time on adverse birth outcome in Ethiopia, 2022
Discussion
Adverse birth outcomes such as low birth weight, stillbirth, and preterm birth constituted the highest rates of all the adverse pregnancy outcomes and are common in developing countries. In this systematic review and Meta-analysis, the pooled prevalence of adverse fetal outcomes in Ethiopia was 25 (95% CI; 20-39; I2 = 97.44, Pv= 0.001). The most common adverse birth outcome categories were low birth weight of 9 %7–12, and preterm birth 8%3–6 and still birth was 5%.
Birth weight is an important determinant of perinatal, neonatal and post neonatal outcomes. Poor intra-uterine growth would increase the risks of perinatal, infant and child mortality and morbidity. Consequently, addressing the burden of low birth weight would contribute significantly towards the achievement of sustainable development Goals. In the present study the magnitude of low birth weight was lower than study conducted on regional and global estimate by UNICEF20. This might be due to different socio cultural, socio economic and time difference. The current study mainly focused on one country and whereas the second studied on global.
This review was estimated the overall prevalence of preterm (prematurity) among adverse fetal outcomes in Ethiopia. Hence, the overall pooled prevalence of preterm was 8 %. This study finding was less than the study done in Asia 10.4, North America 11.2, Sub-Saharan Africa 12%, and Nigeria 11.4 but in line with study done South Korea 7.1% and Indonesia 10.4%21-23. This result is consistent with Asian and African countries as the health care system for maternal and newborn health are almost similar. In addition, Low income countries are implementing various prevention strategies and modalities for preterm births in collaboration with governmental and non-governmental organizations from African countries, including our country. This result made being lower compared to the global target for preterm births for the contribution of neonatal mortality and - morbidity.
This meta-analysis was estimated the national prevalence of stillbirth among adverse fetal outcomes in Ethiopia. Hence, the overall pooled prevalence of stillbirth was 7.09% (4.93–9.26). This review finding is lower than the study conducted in India which was 25.3, Pakistan which was 56.9% and Guatemala 19.95,24. This discrepancy may be due to the fact that the study participants included in this systematic review and meta-analysis assessed multiple original studies in a single country; could be not global representative compared to studies that are conducted worldwide and consist of many countries at the same time.
Having pregnancy complications was more than two times more likely to develop adverse fetal outcomes. This study finding is in line with the study done in Kenya25, Bangladesh26, and China27. The possible reason could be due to women who have current pregnancy complications such as: Premature rupture of membranes, antepartum hemorrhage, and abnormal labor and pregnancy are the most common complications of pregnancy and childbirth, leading to preterm birth, stillbirth, and low birth weight.
The odds of living in rural were two times more likely to develop adverse fetal outcomes. This study finding is in line with the study done in China27, and urban Brazil28. This might be due to women who live in rural areas aren't getting health care services comprehensively and they are less likely to be informed about the danger sign and complication of pregnancy, labor, and delivery. Furthermore, cultural practices and norm in rural areas have a great effect on the nutritional status of women through the prevention of essential foods and or drinks29.
This review was estimated the overall prevalence of low birth weight among adverse birth outcomes in Ethiopia. Hence, the overall pooled prevalence of low birth weight was 10.06% (7.21–12.91). This study finding is in line with the study done in Indonesia 12.9], Armenia [9.0%, higher than the study conducted in Nigeria 6.3% and lower than the study done in Kenya 12.3], Tanzania (13.9%), South Africa 38.54%(30, 31). Low birth weight has different known and idiopathic risk factors; such as environmental and lifestyle risk factors, fetal risk factors, obstetric related factors, medical related factors, and maternal & family sociodemographic risk factors. Having the supremacof the above-motioned risk factors in each country may be increasing the magnitude of the preterm birth even death may have happened secondary to prematurity of the baby.
Having no ANC follow up was 2.6 times more likely to develop adverse birth outcomes. This study finding is in line with the study done in united republic of Tanzania32, and retrospective cross sectional study conducted in Gambia33. This might be due to During ANC follow up women will have a chance to access information related to danger signs of pregnancy. Having regular ANC follow up will also help a pregnant woman seek early treatment for her potential pregnancy-related problems.
Publication bias is one or more of the following has existed: selection bias, true heterogeneity, artifact, and chances are the main sources of publication bias. Large studies are likely to be published regardless of statistical significance because these studies involve large commitments of time and resources whereas Small studies are at greatest risk for being lost, because of the small sample size. In this study publication bias was not detected (Eggers, p value = 0.522) of the polled estimated prevalence of adverse fetal outcomes.
Conclusion
The overall pooled estimate of adverse fetal outcomes in Ethiopia was high. Being resided in rural, not attending ANC, age ≥ 35, and developing complication during pregnancy and child birth were identified predictors for adverse fetal outcomes in Ethiopia. Therefore, based on the study findings, the authors recommend particular emphasis shall be given to have regular antenatal care follow up eight visits as per national recommendation, health education, early detection, and intervention of obstetric complications. Creating awareness of women on the effect of pregnancy at an advanced age, and providing timely and focused antenatal care (ANC) follow up to all pregnant women are very crucial to reduce the magnitude of the problem
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Csa IJCSA Central Statistical Agency (CSA)[Ethiopia] and ICF 2016 Addis Ababa Ethiopia Demographic and Health Survey
- 2Behrman RE Butler AS Mortality and acute complications in preterm infants. Preterm Birth: Causes, consequences, and prevention 2007 US National Academies Press 20669423 · pubmed ↗
- 3Soon BTJGWHO The global action report on preterm birth 2012
- 4Targets WWGNJWHO 2025: Low birth weight policy brief 20147
- 5Blencowe H Cousens S Jassir FB Say L Chou D Mathers C National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis 201642 e 98e 10810.1016/S 2214-109X(15)00275-226795602 · doi ↗ · pubmed ↗
- 6Vogel JP Chawanpaiboon S Watananirun K Lumbiganon P Petzold M Moller A-B Global, regional and national levels and trends of preterm birth rates for 1990 to 2014: protocol for development of World Health Organization estimates 20161311910.1186/s 12978-016-0193-1PMC 491275427317125 · doi ↗ · pubmed ↗
- 7Gedefaw G Alemnew B Demis AJ Bp Adverse fetal outcomes and its associated factors in Ethiopia: a systematic review and meta-analysis 202020111210.1186/s 12887-020-02176-9PMC 726848832493464 · doi ↗ · pubmed ↗
- 8Bililign N Legesse M Akibu M Ji JA Review of Low Birth Weight in Ethiopia: Socio-Demographic and Obstetric Risk Factors Abstract Magnitude of low birth weight 2018515