WRAP53 is Downregulated in Acute Myeloid Leukemia Patients and Positively Correlates With HTERT Expression
Renan Brito Gadelha, Beatriz Maria Dias Nogueira, Caio Bezerra Machado, Flávia Melo Cunha de Pinho Pessoa, Anna Karolyna da Costa Machado, Germison Silva Lopes, Paulo Henrique Silva Rodrigues, Henrique Girão Martins, Deivide de Sousa Oliveira, Rodrigo Monteiro Ribeiro

TL;DR
This study found that WRAP53 gene expression is reduced in AML patients and is linked to hTERT, suggesting it could be a new biomarker for genomic stability in leukemia.
Contribution
The novel finding is the positive correlation between WRAP53 and hTERT expression in AML, suggesting WRAP53 as a potential new biomarker.
Findings
WRAP53 expression is significantly downregulated in AML patients compared to controls.
WRAP53 and hTERT gene expression levels are moderately positively correlated.
WRAP53 expression varies with patient sex and age but not overall survival.
Abstract
Acute myeloid leukemia (AML) is a prevalent hematologic malignancy in adults, marked by clonal disorders in hematopoietic cells, rapid progression, and genetic heterogeneity. The WRAP53 gene, which is associated with genomic stability due to its involvement in activities, such as DNA repair, TP53 regulation, and association with telomerase (hTERT), was the focus of this study. This study aimed to identify new potential molecular markers with prognostic value, based on specific targets, in order to contribute to a more accurate stratification of patients. We assessed WRAP53 and hTERT expression in 110 AML patients classified according to World Health Organization (WHO) guidelines. Using real‐time quantitative PCR, we investigated their expression and correlation with clinical outcome variables. WRAP53 expression was significantly decreased in AML patients compared to controls, whereas…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
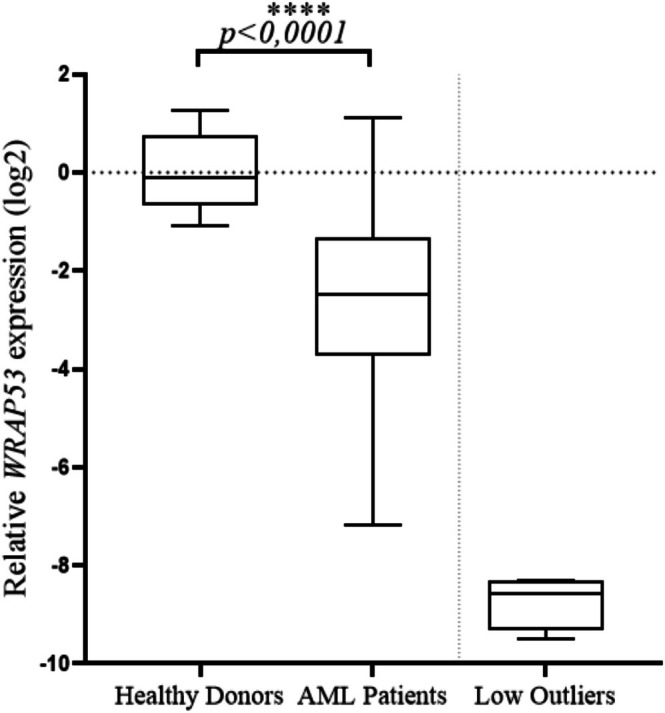 FIGURE 1
FIGURE 1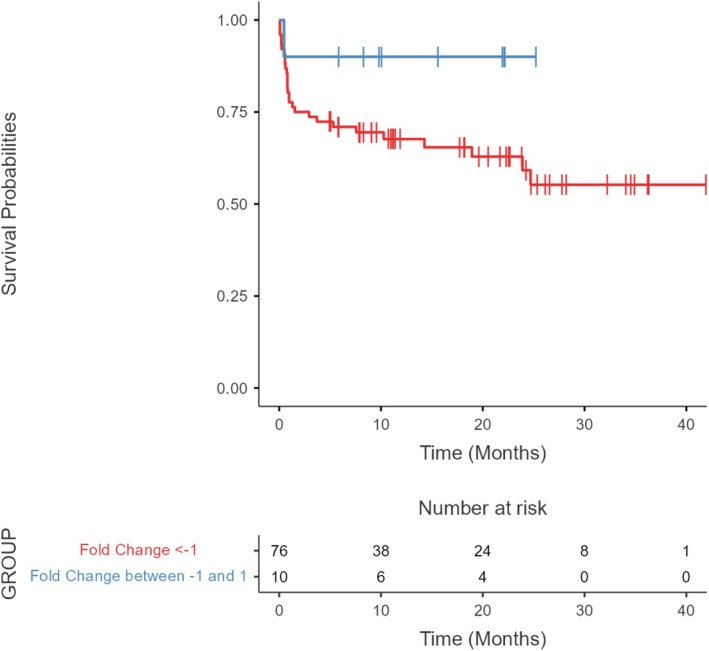 FIGURE 2
FIGURE 2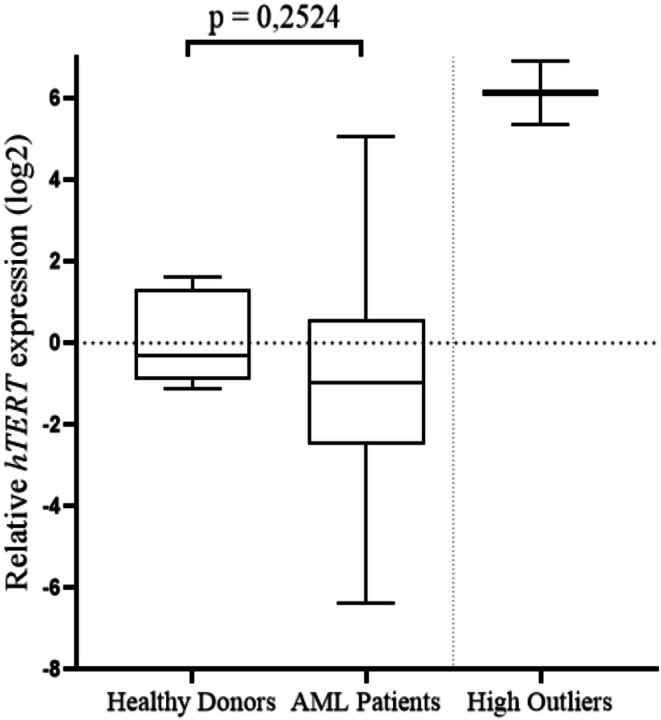 FIGURE 3
FIGURE 3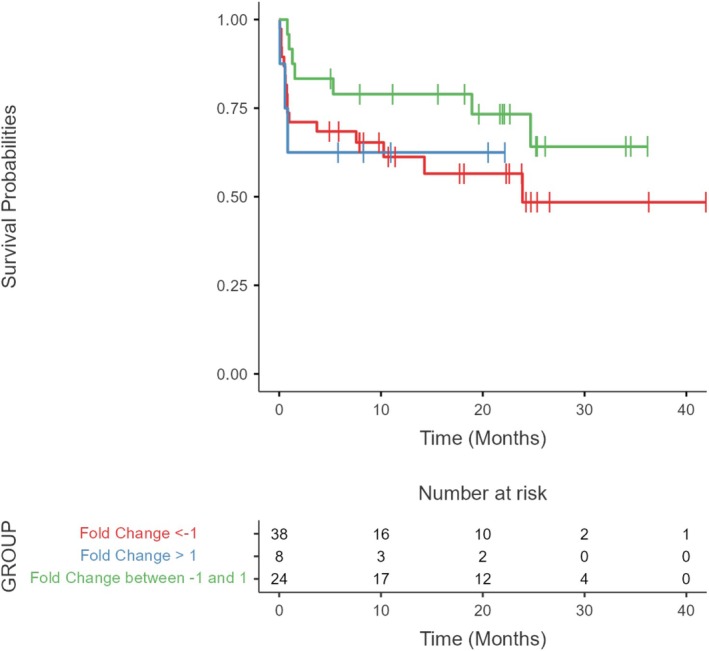 FIGURE 4
FIGURE 4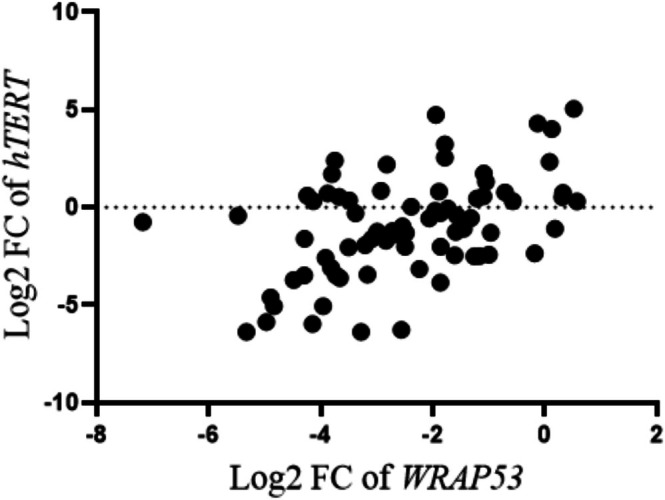 FIGURE 5
FIGURE 5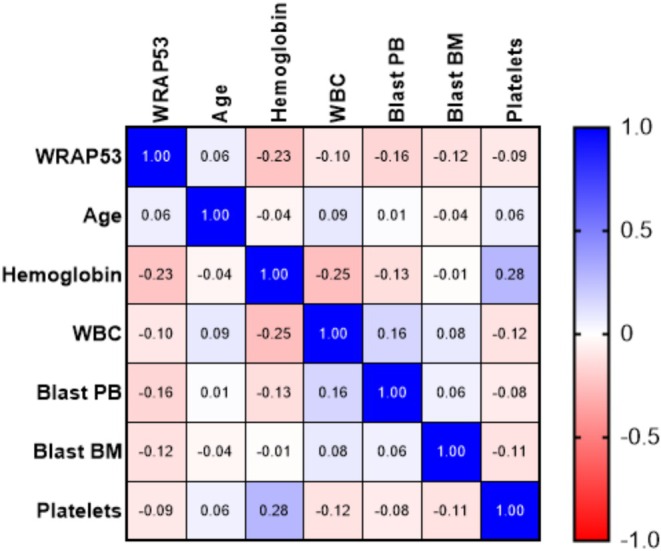 FIGURE 6
FIGURE 6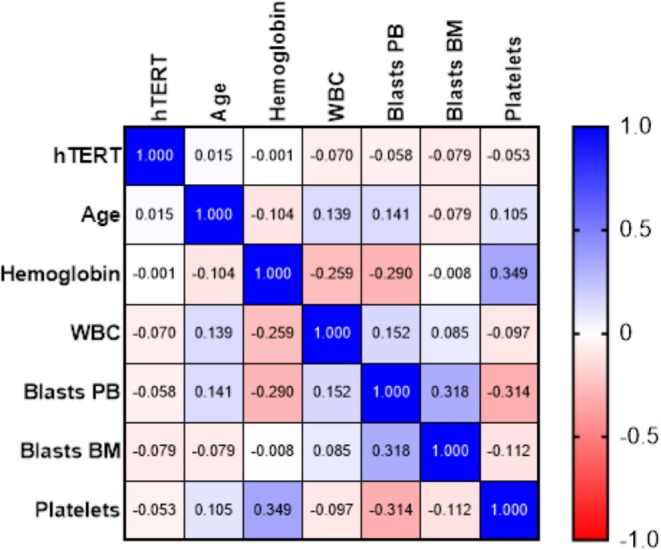 FIGURE 7
FIGURE 7| AML patients' clinical data | |
|---|---|
| Hemoglobin |
< 8 g/dL: 72 (65.4%) 8–10 g/dL: 29 (26.3%) > 10 g/dL: 9 (8.3%) |
| WBC |
≤ 10.000/mm3: 47 (42.7%) > 10.000/mm3: 46 (41%) > 100.000/mm3: 18 (16.3%) |
| Blasts in peripheral blood |
Yes: 65 (59%) No: 45 (41%) |
| Blasts in bone marrow |
Blasts ≤ 10%: Blasts ≤ 70%: Blasts > 70%: N.R: 3 |
| Platelets |
< 150.000/mm3: 93 (84.5%) > 150.000/mm3: 17 (15.5%) |
| LHD |
LDH ≤ 400 μL: 37 LDH > 400 μL: 32 LDH > 1.000 μL: 13 N.R: 28 |
| Immunophenotyping | CD33, CD117, CD45, CD34, CD13, HLA‐DR, MPO e CD64 |
| Karyotype |
Favorable: 9% Intermediary: 30% Adverse: 44% N.C: 17% |
| Parameter | Total ( |
|
|
|
|
|---|---|---|---|---|---|
| Sex | |||||
| Male (%) | 49 (51) | −3222 ( | 0.0322* | −0.0305 ( | 0.6132 |
| Female (%) | 47 (49) | −2613 ( | −0.1975 ( | ||
| Age | |||||
| ≤ 60 | 68 | −3120 ( | 0.0469* | −0.3334 ( | 0.0795 |
| > 60 | 28 | −2490 ( | 0.218 7 ( | ||
| Parameter | Total ( |
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|
| Sex | |||||||
| Male (%) | 37 (49) | −2591 ( | 0.8192 | 0.0342 ( | 0.6049 |
3232 ( 3284 ( | 0.5338 |
| Female (%) | 40 (51) | −2419 ( | 0.4605 ( | ||||
| Age | |||||||
| ≤ 60 | 53 | −2458 ( | 0.3382 | 0.3651 ( | 0.8410 | 3232 ( | 0.8111 |
| > 60 | 24 | −2662 ( | 0.3173 ( | 3422 ( |
- —Conselho Nacional de Desenvolvimento Científico e Tecnológico10.13039/501100003593
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Telomeres, Telomerase, and Senescence · Cancer-related Molecular Pathways
Introduction
1
Cancers arise through a series of mutations or genetic alterations that give the cell the ability to override proapoptotic and antiproliferative signals, allowing it to reach hallmarks such as replicative immortality, invasion, and metastasis [1, 2, 3].
Acute myeloid leukemia (AML) is a heterogeneous group of hematopoietic neoplasms that affect myeloid precursor cells and is characterized by the clonal expansion of immature leukemic blasts, primarily in the bone marrow that may subsequently reach the peripheral blood. The disease is characterized by high molecular heterogeneity and is associated with a poor prognosis, with an aggressive clinical course, low remission rates, and high mortality rates [4, 5].
Owing to the high mutational burden present in leukemias resulting from telomere attrition, chromosomal translocations are among the most common genetic alterations reported in this disease and play crucial roles in progression and resistance to treatment. Telomerase (hTERT) is the enzyme responsible for preserving telomere length at the ends of chromosomes; mutations in genes related to telomeres and telomerase, such as dyskerin pseudouridine synthase 1 (DKC1), telomerase RNA component (TERC), telomerase reverse transcriptase (TERT), WRAP53, and NOP10 ribonucleoprotein (NOP10), among others, which play a role in telomerase function and telomere maintenance, may contribute not only to genomic instability but also to bone marrow failure, increasing the risk of developing AML [5, 6, 7, 8].
In AML, alterations in hTERT expression have been reported [9, 10]. However, low or absent hTERT expression has also been observed in some patients [11], which may reflect the presence of alternative telomere maintenance mechanisms, such as ALT (alternative lengthening of telomeres), or indicate distinct molecular profiles within the heterogeneous landscape of AML [12]. This variation in expression makes the study of hTERT relevant for both diagnostic and prognostic purposes, especially when associated with other genes involved in genomic stability.
The WRAP53 gene, located on chromosome 17p13, has three distinct transcriptional start sites, which give rise to three main transcript variants: WRAP53‐α, WRAP53‐β, and WRAP53‐γ [13]. Alternative splicing is a crucial process in the regulation of gene expression and allows a single gene to encode multiple functionally distinct protein products with opposing roles in physiological and pathological contexts [14, 15, 16, 17, 18]. This molecular mechanism confers on the WRAP53 gene the ability to produce isoforms with specific subcellular locations and functions.
The isoforms: WRAP53α, WRAP53β, and WRAP53γ have different functions. WRAP53α is in charge of encoding a p53 regulatory RNA, whereas WRAP53β is a scaffold protein involved in the repair of DNA damage, the maintenance of nuclear bodies known as Cajal bodies, and the assembly of telomerase. There are still no studies reporting WRAP53γ function. WRAP53β cellular localization together with WRAP53 expression in solid tumors are factors that predict an effective response to radiotherapy, in addition to serving as a tumor biomarker [8, 19, 20, 21, 22, 23]. Although there are no articles in the literature elucidating the function of WRAP53 in leukemias, changes in its expression levels and alterations at the genetic level, such as mutations, have already been well reported in solid tumor neoplasms.
Therefore, the aim of this study was to evaluate the gene expression profiles of WRAP53 and hTERT in a cohort of AML patients, to evaluate their possible roles in the leukemogenesis pathway.
Materials and Methods
2
Biological Samples
2.1
A total of 110 adult patients diagnosed with acute myeloid leukemia treated at General Hospital of Fortaleza, Dr. César Cals General Hospital, and São Vicente de Paulo Maternity Hospital, reference centers for oncohematological treatment in the state of Ceará (Ceará, CE, Brazil) participated in this study. To categorize patients into different groups, the European LeukemiaNet (ELN) guidelines [24] were used, where patients were categorized according to age, white blood cell (WBC) count, hemoglobin levels, and sex. The cytogenetic risk assessment was carried out according to the World Health Organization (WHO) criteria [25]. Furthermore, previously, patients in this study were screened for genetic abnormalities, such as BCR::ABL1 p190, PML::RARA, RUNX1::RUX1T1, and CBF::MYH11, via reverse transcription polymerase chain reaction (RT–qPCR) [26]. Additionally, 10 peripheral blood samples were collected from healthy volunteers and employed as control samples. Although all patients in the study were adults, their legal guardians informed them about the informed consent in cases where the patient's condition or status prevented personal signature, after which the patients underwent a clinical evaluation for the collection of biological material. The methods were performed in accordance with the Helsinki guidelines and regulations. The study was approved by the Ethics Committee of the Federal University of Ceará and Dr. César Cals General Hospital with the following approval numbers: 4.339.719 and 5.823.921.
RNA Extraction and cDNA Conversion
2.2
Total RNA was extracted from the peripheral blood buffy coats of AML patients via the TRIzol Reagent (InvitrogenTM) according to the manufacturer's instructions and quantified via absorbance using a NanoDrop spectrophotometer (Thermo Fisher Scientific).
Complementary DNA (cDNA) was synthesized from 20 ng of total RNA extracted via a high‐capacity cDNA reverse transcriptase kit (Thermo Fisher Scientific). The conversion step was carried out in a Veriti thermal cycler (Applied Biosystems). The cDNA samples were stored in a −20°C freezer to establish a cDNA library and remained frozen until analysis.
Validation of Gene Expression by Real‐Time Quantitative Polymerase Chain Reaction (qPCR)
2.3
The genes selected for evaluation of gene expression were WRAP53 (Hs_Hs00216360_m1), hTERT (Hs_00972650_m1), and the endogenous ABL1 gene (Hs01104728_m1), which was used as an internal control. The detection method was the TaqMan gene expression assay system (Applied Biosystems, Foster City, CA, USA), and qPCR was performed via the QuantStudio5 Real‐Time PCR system (Applied Biosystems, Foster City, CA, USA). The ABL1 reference gene used in this study was previously validated by RT–qPCR detection in AML patients and was determined to be one of the most appropriate endogenous genes for expression assay analysis [27]. Among the different transcripts of the WRAP53 gene, the one analyzed in this study was WRAP53β.
For each sample, the following were used: 1 μL of cDNA, 0.5 μL of each primer/probe, 5 μL of TaqMan Gene Expression Master Mix (Life Technologies, Carlsbad, CA, USA), and 3.5 μL of ultrapure water. Gene expression levels were based on absolute and relative analyses via the 2‐ΔΔCQ method, with samples from healthy donors used as calibrators/controls. Each sample was analyzed in replicate for experimental and technical validation, following international standards for evaluating gene expression via real‐time PCR [28]. Fold change (FC) criteria were defined to identify differentially expressed genes. For the WRAP53 gene, two groups were created: one with FC values < −1 (differentially expressed) and another with FC values between −1 and 1 (not differentially expressed). For hTERT, the categorization included three groups of values: FC < −1, between −1 and 1, and greater than 1 (differentially expressed).
Statistical Analysis
2.4
The data on the relative mRNA expression of WRAP53 and hTERT are expressed as the means to determine the potential associations between gene expression and variables. Normality was assessed by the Kolmogorov–Smirnov or Shapiro–Wilk test and was applied to each specific group. The outliers were removed on the basis of the upper and lower fences of the interquartile range. Differences in continuous variables were analyzed via the Mann–Whitney or unpaired t‐test to compare medians between two groups and the Kruskal–Wallis test or one‐way ANOVA to compare medians among variables with three or more groups. The correlation between two continuous variables was determined via the Pearson correlation coefficient. Furthermore, a multiple linear regression was performed to evaluate the association between WRAP53 and hTERT expression, simultaneously adjusting for clinical variables. Survival probabilities were estimated via the Kaplan–Meier method, and differences in survival distributions were assessed via the log‐rank test, where overall patient survival was determined from the date of diagnosis until death or the last follow‐up. Statistical analyses, along with graph generation, were carried out via GraphPad Prism (version 8.0) software. The LogRank test was performed with Jamovi software (version 2.3.28). Significant differences were considered with a 95% confidence interval (p < 0.05).
Results
3
Clinical Features of AML Patients
3.1
In total, samples were collected from 110 patients, 56 (50.9%) men and 54 (49.1%) women. The average age among patients was 50.3 years, with men averaging 49.3 years and women 51.4 years. The clinical characteristics of AML patients are detailed in (Table 1). Key findings include low hemoglobin levels in 65.4% of patients, circulating blasts in 59%, and thrombocytopenia in 84.5%. Immunophenotyping revealed predominant markers such as CD33, CD117, and CD45, while karyotype analysis classified 44% of patients as adverse. Patients for whom karyotype and fusion results were unavailable and not detected in previous screening were classified as not classifiable (NC).
Gene Expression of
WRAP53 in AML Patients
3.2
The analyzed data were normalized, and Log2 FC levels were used as a cutoff for the analysis of WRAP53 gene expression. Patients were divided into two main groups; the first group consisted of samples with FC ≤ −1 (n = 79), representing reduced WRAP53 gene expression, and the second group included samples with FC values between −1 and > 1 (n = 17), representing minimal variation or no significant change in WRAP53 expression. For analysis of the expression results, patients were classified into different groups based on the ELN guidelines [24], being, by age ≤ 60 and > 60, in the leukocyte count (WBC), separated into groups of < 10 × 10^3^/mm^3^, > 10 × 10^3^/mm^3^, and ≥ 100 × 10^3^/mm^3^, in sex (male or female), and by hemoglobin levels < 8 g/dL, 8–10 g/dL, and ≥ 10 g/dL. For the cytogenetic risk group, the classification of patients was based on the WHO guidelines [25].
In our cohort of AML patients, the mean expression level of WRAP53 was −2.490 and was lower than that in blood samples from 10 healthy donors (control group); the mean expression level in the control group was −0.1111 (p < 0.0001) and can be seen in Figure 1 where the entire studied sample is represented. WRAP53 was expressed in 100 of the 110 AML patients included in the study. In the 10 cases without WRAP53 detection, expression of the endogenous ABL gene was confirmed. The outliers were not considered in the statistical calculations (n = 4).
Evaluation of the expression of the WRAP53 gene in peripheral blood samples from patients with AML compared with the control group. AML patients demonstrate a low expression of WRAP53 compared to the control group (n = 10) (p < 0.0001), low outliers removed (n = 4). Data are presented as mean. For statistical analysis, normal distribution was assessed by the Kolmogorov–Smirnov normality test and was followed by the unpaired t‐test.
When clinical variables such as sex, age, hemoglobin, leukocyte count, or cytogenetics were analyzed, statistically significant differences were observed across the sex and age groups. Furthermore, a slight trend was observed in some parameters, such as a greater percentage of men, a greater number of patients aged < 60, patients with hemoglobin below 8 g/dL, and a greater number of patients classified as having adverse risk in the FC < −1 groups.
In the male group (49 patients), the mean expression of WRAP53 was significantly lower in cases with differential expression (FC ≤ −1) compared to the female group (47 patients), with values of −3.222 and −2.613, respectively (p = 0.0322). There was no significant difference in the group without differential expression (FC between −1 and 1). Regarding age, patients over 60 years old showed higher mean expression of WRAP53 in the FC ≤ −1 group (p = 0.0496), but there was no significant difference in the FC between −1 and 1 group (p = 0.0795). (Table 2).
For white blood cells (WBC), there was no statistically significant difference in WRAP53 expression between the FC ≤ −1 and FC between −1 and 1 groups, regardless of WBC count (p = 0.3683 and 0.1953). Regarding hemoglobin levels, no significant association was observed between hemoglobin ranges and WRAP53 expression (p = 0.1205 and 0.2637). In risk stratification, there was no significant difference in WRAP53 expression among favorable, intermediate, adverse, and unclassified risk groups (p = 0.6198 and 0.4586).
Kaplan–Meier Survival Analysis for
WRAP53
3.3
We performed a survival analysis to evaluate the association of WRAP53 gene expression levels and their potential association with prognosis in hematologic malignancies. The analysis included all patients with complete clinical and epidemiologic data and who had WRAP53 expression (n = 86). A The mean follow‐up time was 13.4 months. We used the same expression data, divided into two groups: patients with FC ≤ −1 and FC between −1 and 1 of WRAP53 on the hypothesis that altered expression of this gene may influence the survival of patients with AML. The analysis showed that WRAP53 expression levels did not present significant changes between the groups above or below the median Log‐Rank (p = 0.150), as shown in Figure 2.
Survival analysis in patients with different levels of WRAP53 expression. A Survival analysis of patients with different levels of WRAP53 expression. There were no statistical differences between groups Log‐Rank (p = 0.150). The data shown in the risk table that is presented in the image shows the probability of the event (death) over time in the studied sample with information on the number of individuals at risk of experiencing the event at each time interval.
Gene Expression of
hTERT in AML Patients
3.4
As previously described, the data analyzed here were normalized, assuming that Log2 FC levels were used as a cutoff point, where patients were divided into three groups representing the variation in gene expression. The first group included samples with FC ≤ −1 (n = 38), indicating a reduction in hTERT gene expression; the second group included those with FCs between −1 and 1 (n = 26), representing minimal variation or no significant change in expression; and the third group consisted of those with FC > 1 (n = 13), indicating a variation in increased hTERT gene expression. For analysis of the expression results, patients were classified as in the previous analysis considering age, leukocyte count, sex, hemoglobin level, and cytogenetic risk group [24, 25].
In this study, we did not identify differences in hTERT expression in our cohort of AML patients (mean hTERT: −0.9658) compared with blood samples from 10 healthy donors (control group, mean control group: −0.2942), p = 0.2524. Figure 3, which represents the entire sample studied, shows the expression level of the entire sample. hTERT expression was identified in 79 of the 110 patients with AML included in the study. In the 31 cases without hTERT detection, the expression of the endogenous ABL gene was confirmed. The outliers were not considered in the statistical calculations (n = 2).
Evaluation of hTERT expression in the peripheral blood of patients with AML compared with the control group. In this study, we did not identify differences in hTERT expression (p = 0.2524) in our cohort compared with the control group, high outliers removed (n = 2). Data are presented as mean. For statistical analysis, normal distribution was assessed by the Kolmogorov–Smirnov normality test and was followed by the unpaired t‐test.
The evaluation of clinical variables did not show statistical significance. Regarding risk stratification, patients classified as adverse risk were more likely to have a lower hTERT expression, although no significant difference was found for favorable or intermediate risk groups. Overall, although some trends were observed, these findings did not reveal statistical significance against clinical parameters.
The expression of the hTERT gene was compared between men and women with AML in the groups with FC ≤ −1, FC between −1 and 1, and FC > 1. In the male group (n = 38), the mean expression values were −2.591, 0.0342, and 3.232, respectively, while in the female group (n = 41), the mean values were −2.419, 0.4605, and 3.284, respectively. The p values were 0.8192, 0.6049, and 0.5338, indicating no statistically significant difference between sexes in the analyzed groups. Regarding age, there was also no significant difference in hTERT expression between individuals ≤ 60 years and > 60 years (p = 0.3382, 0.8410, and 0.8111 for FC ≤ −1, FC between −1 and 1, and FC > 1, respectively) (Table 3).
For the clinical variables analyzed regarding the hTERT gene, no significant differences in expression were observed between the groups with FC ≤ −1, FC between −1 and 1, and FC > 1. Regarding white blood cell (WBC) count, the p‐values were 0.1688, 0.7441, and 0.7308, respectively, indicating no statistical difference between the groups. For hemoglobin levels, there were also no significant differences in the ranges < 8, 8–10, and ≥ 10 g/dL (p = 0.3131, 0.1098, and 0.8678, respectively). In cytogenetic risk stratification, no significant differences were found between the groups (p = 0.0549, 0.4628, and 0.4628, respectively).
Kaplan–Meier Survival Analysis for
hTERT
3.5
We performed a survival analysis to assess the association of hTERT gene expression levels and their potential association with prognosis. The analysis included all patients with complete clinical and epidemiologic data and who had hTERT expression (n = 70). The median follow‐up time was 13.4 months. We used the same expression data, divided into three groups by FC values, namely: FC < −1, FC between −1 and 1, and FC > 1 on the hypothesis that altered expression of this gene may influence the survival of patients with AML. The analysis showed that hTERT expression levels did not present significant changes between the Log‐Rank groups (p = 0.316), as shown in Figure 4.
Comparison of survival time in patients with different levels of hTERT expression. Survival time was not statistically significant between expression groups (p = 0.316). The data in the risk table presented in the image show the probability of the event (death) over time in the studied sample with information on the number of individuals at risk of experiencing the event at each time interval.
WRAP53
Expression Is Correlated With hTERT
4
A Pearson correlation analysis revealed a moderate positive relationship between WRAP53 and hTERT expression levels, with a correlation coefficient of r = 0.475 and a p value < 0.0001, indicating a statistically significant positive association (Figure 5).
Correlation between WRAP53 and hTERT gene expression in AML patients. The scatter plot shows the relationship between the log2 FC values of WRAP53 and hTERT. Each point represents expression data. The analysis suggested a positive correlation between WRAP53 and hTERT expression (r = 0.475, p < 0.0001).
Among the variables analyzed, WRAP53 showed no correlation with variables, with the most negative values in relation to hemoglobin (−0.23). The other variables analyzed here presented weak correlations with each other, showing limited or independent interactions in the sample analyzed (Figure 6).
Correlation analysis between WRAP53 levels and clinical and laboratory parameters in patients with acute leukemia. The color intensity reflects the magnitude of the correlation and the associations between the variables WRAP53, age, hemoglobin, WBC, peripheral blood blasts, bone marrow blasts, and platelet count. The values range from −1 (negative correlation) to 1 (positive correlation), with 0 indicating no association between the variables. The _observed variations have correlations ranging from weak to moderate. BM, Bone morrow; PB, Peripheral blood; WBC, White blood cell.
hTERT showed very weak correlations with all variables, indicating that this variable is practically independent of the others analyzed. Other variables also showed weak correlations with each other, such as WBC and peripheral blood (PB) blasts (0.15) and Blast Bone marrow (BM) and Blast PB (0.32), indicating a moderate relationship between the latter. On the other hand, it was possible to observe a positive correlation between hemoglobin and platelets (0.35), revealing a moderate association. Hemoglobin also correlated negatively with WBC (−0.26) and Blast PB (−0.29) (Figure 7).
Correlation analysis between hTERT levels, clinical and laboratory parameters in patients with acute leukemias. The color intensity reflects the magnitude of the correlation and the associations between the variables hTERT, age, hemoglobin, white blood cell, peripheral blood blasts, bone marrow blasts, and platelet count. The values range from −1 (negative correlation) to 1 (positive correlation), with 0 indicating no association between the variables. hTERT showed weak correlations with the other variables, while the most notable correlations include the relationship between hemoglobin and platelets (0.35) and between Blast BM and Blast PB (0.32). BM, Bone morrow; PB, Peripheral blood; WBC, White blood cell.
Multiple linear regression analysis revealed a reciprocal association between WRAP53 and hTERT gene expression. When hTERT expression was considered as the dependent variable, only WRAP53 maintained a robust independent effect (β = 0.709; p < 0.001), explaining approximately 27% of its variability. In contrast, when WRAP53 was modeled as the outcome, only hTERT was significantly positively associated (β = 0.282; p < 0.001), accounting for approximately 26% of the gene's variability. In both models, clinical variables showed no statistically significant association. The linear regression assumptions were verified and adequately met in both analyses.
Discussion
5
AML is the most common acute leukemia in adults and is characterized by high genetic heterogeneity both in diagnosis and in disease progression. Despite advances, treatment still consists of complex chemotherapy regimens combined with bone marrow transplantation for eligible patients. The identification of new biomarkers is essential because, in addition to contributing to a better understanding of the molecular basis of the disease, it may aid in the diagnosis, prognosis, and monitoring of AML [29, 30]. Recent studies indicate that structural alterations or changes in the expression levels of WRAP53 transcripts may be associated with genomic instability and impaired DNA repair, mechanisms that may contribute to disease progression [8].
In this study, a slightly greater frequency of AML was observed in men, and a greater incidence was observed among individuals aged 55 years or older. Clinical characteristics, such as hemoglobin values, leukocyte counts, the presence of blasts in peripheral blood, and platelet counts, revealed the presence of anemia, thrombocytopenia, and leukocytosis with the presence of circulating blast cells in our patients. These findings are similar to those reported in the literature for patients with AML [31, 32, 33, 34, 35].
The WRAP53 gene has three transcriptional start sites, from which the transcript variants WRAP53‐α, WRAP53‐β, and WRAP53‐γ are generated, whose expression levels are generally increased in cancer. The α and β isoforms are the most frequently studied in different tumor types. WRAP53α acts as an antisense RNA for the TP53 gene, while WRAP53β encodes a protein that can be localized in both the nucleus and cytoplasm of tumor cells. WRAP53β has been widely investigated due to its potential as a biomarker of both radiotherapy resistance and as a predictor of poor prognosis in several cancers, including colorectal [19], ovarian [22], breast [36], head and neck [37], and lung carcinomas [38, 39, 40]. To date, there are no studies in the literature that have clearly elucidated the biological importance and function of the WRAP53‐γ variant. Furthermore, dyskeratosis congenita, a disease characterized by rapid and progressive shortening of telomeres with a high probability of developing bone marrow failure and cancer, is due to the presence of mutations in the WRAP53 gene [41]. WRAP53β action is independent of WRAP53α‐mediated p53 regulation [13].
On the other hand, for Bergstrand, Obrien, and Farnebo (2019) [42], the frequently observed high expression of WRAP53β in cancer is related to its involvement in the DNA damage response (DDR) that arises due to precancerous lesions. The authors argue that in response to replication stress and DDR signaling, WRAP53β overexpression occurs, which helps recruit factors that act in DNA repair to maintain genomic integrity. However, cells that accumulate mutations that impair the DDR, such as reduced WRAP53β expression, are able to escape cellular control mechanisms, thus contributing to genomic instability and cancer progression. The main reason for this argument is that most studies reporting WRAP53β overexpression did not observe an association with survival.
In this study, we demonstrated that WRAP53 expression was lower in the AML patient cohort than in the control cohort (p < 0.0001). Studies show that low levels of WRAP53 associate with downregulation of factors involved in DDR due to downregulation of WRAP53β; moreover, WRAP53α may also be downregulated, which in turn will result in the inactivation of p53 at the mRNA level, thus impairing p53 action after DNA damage [13, 43, 44, 45]. In ovarian cancer, downregulation of WRAP53β or the presence of genetic variations in WRAP53 is associated with increased mortality and increased risk of ovarian development [22, 46], whereas in metastatic rectal and head and neck cancer, it is related to resistance to radiotherapy [19, 20, 37, 47, 48]. In breast cancer, low nucleolar levels are associated with increased recurrence, death, and resistance to radiotherapy [23, 36]. Moreover, the high presence of nuclear WRAP53β is related to faster and more effective DNA repair due to the rapid recruitment of DDR factors [49]. The action of WRAP53β is independent of and does not influence the regulation of p53 mediated by WRAP53α [13]. The DDR is essential for leukemic cells, but this function is often abnormal in AML, which may contribute to leukemogenesis and treatment resistance, resulting in an unfavorable prognosis [50, 51].
Here, we evaluated the expression of the WRAP53 gene in combination with clinical factors, such as hematological parameters, risk classification, age and sex, where among these factors, only sex and age presented statistical significance, specifically in the FC < −1 group, where it was observed that females presented a higher mean expression of WRAP53 (p = 0.0322) than males did. A difference in expression was also found in patients over 60 years of age, where this group presented a greater mean than did the ≤ 60 years of age group (p = 0.0496). In studies with solid tumors, WRAP53 expression was not independently analyzed in correlation with all the parameters analyzed here, as it was only paired with age or sex, where no correlations with WRAP53 expression were observed [36, 38, 40]. The clinicopathological characteristics analyzed in most studies were the degree of tumor differentiation, tumor size, the presence of invasion or lymph node metastasis, and clinical stage (I, II, III, IV, or V), all of which are not applicable for our nonsolid tumor patient cohort and were not analyzed in this work [19, 38, 40, 52].
Regarding the analysis of hTERT, in this study, the analysis of gene expression in peripheral blood did not reveal a difference in expression when compared with patients in the control group (p = 0.2524). Calvello et al., (2017) [11], when analyzing the expression of hTERT in patients with AML, reported a lower total expression of hTERT, which was attributed to the presence of the transdominant variant –α + β of hTERT, where patients with AML presented a lower percentage of the active isoform of hTERT (+α + β) than did the control group. However, other studies indicate that the presence of the active isoform of telomerase in the patients analyzed was greater than 20% [53]. The main hTERT isoform described by Kilian et al., 1997 [54] is +α + β, which produces the complete transcript capable of producing the active telomerase enzyme. The deletion of α (−α), which is present in exon 6, acts as a dominant inhibitor of telomerase, and the deletion of ‐β leads to degradation of the mRNA transcript due to the presence of a premature stop codon (nonsense codon). Finally, the deletion of both leads to the isoform ‐α‐β, which also results in mRNA degradation due to the presence of nonsense codons. The presence of deletions in α or β generates inactive products to avoid the presence of a truncated and nonfunctional protein [55, 56, 57, 58].
In the present study, we observed three distinct hTERT expression profiles among AML patients when compared to healthy donors. While some patients showed reduced or unaltered expression, others displayed moderate expression. This variability may reflect the molecular heterogeneity of AML and suggests differential regulation of telomerase activity across subgroups. Overexpression of hTERT may be linked to a greater proliferative potential of leukemic cells, contributing to disease progression and possible treatment resistance [59, 60, 61, 62, 63, 64, 65, 66], while low expression may indicate the activation of alternative telomere maintenance pathways or reflect differentiated stages of leukemogenesis, potentially associated with poor survival [12, 67, 68].
Capraro et al. (2011) [66] reported that hTERT expression and telomerase activity follow the order of B‐ALL > T‐ALL > AML, where acute lymphoblastic leukemia (ALL) presents both higher telomerase activity and higher expression of hTERT expression than AML does. In addition, telomere length was shorter in AML, T‐ALL, and B‐ALL, respectively. Furthermore, among the subtypes reported for AML, the M0, M3, and M5 subtypes are often mentioned as those with the shortest telomeres and the lowest telomerase expression/activity [10, 66, 67]. These results show how complex the hTERT regulatory system can be in acute leukemias [69].
hTERT activation is commonly found in hematopoietic cells, germ cells, embryonic stem cells, and cancer cells because of its high replicative power. Altered hTERT expression in humans leads to immortality, one of the main hallmarks of cancer [1]. Like many human malignancies, leukemias may exhibit increased telomerase activation, accompanied by elevated hTERT expression. Its dysregulation is a common alteration in leukemogenesis, being present from diagnosis to remission, and is found in the 4 main types of leukemia: acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), chronic myeloid leukemia (CML), and chronic lymphocytic leukemia (CLL), which are associated with the development and progression of the disease [61, 62, 70, 71, 72, 73, 74, 75]. However, the prevalence of hTERT dysregulation is highly variable and dependent on the population of each study [69].
hTERT expression was not correlated with WBC count, age, sex, hemoglobin, or risk groups. These findings are in line with other studies that found no association with these parameters [9, 11, 62, 76]. However, its frequent overexpression at diagnosis and relapse reinforces its biological relevance in AML, particularly in association with complex karyotypes and extramedullary disease [9, 53, 61, 62, 64, 65, 77]. In ALL, high telomerase activity and hTERT expression are associated with disease progression, treatment resistance, shorter survival, and cytogenetic abnormalities, indicating its potential as a biomarker in adult and pediatric patients [67, 75]. While in CLL, high telomerase expression and activity were able to identify patients with different outcomes and were associated with the presence of short telomeres [73, 74]. In CML, high activity is related to the presence of cytogenetic alterations [78].
The overall survival analysis conducted here revealed no significant difference between the WRAP53 and hTERT Log‐Rank groups: p = 0.150; and p = 0.316 respectively. This is contrary to what is reported in studies on solid tumors, where high expression levels related to the cytoplasmic presence of WRAP53β or its low nuclear presence are correlated to low overall survival rates [22, 23, 36, 47]. The same is found for hTERT, where telomerase expression levels or activity were shown as independent prognostic factors for survival in adults with acute or pediatric leukemia [67, 75].
Pearson correlation analysis between WRAP53 and hTERT genes revealed a positive and moderate correlation coefficient r = 0.4374 (p < 0.0001). WRAP53 has previously been correlated with increased telomere length or telomerase activity, but it has not been reported whether telomerase activity was related to prognosis [20, 79, 80]. On the other hand, hTERT expression is correlated with telomerase activity and telomere maintenance [66, 81]. This correlation is relevant since high telomerase activity and high hTERT expression have been observed in AML patients [61, 65, 82]. Furthermore, chromosomal instability due to progressive telomere shortening has been associated with extremely low telomerase activity in AML and impacts treatment response and survival [66].
Importantly, future studies should explore the molecular mechanisms that regulate the interaction of WRAP53 with telomerase and other DNA repair components in AML. Furthermore, investigating the subcellular localization of the WRAP53β protein is essential, as it may provide valuable insights into its activity in the cell nucleus or cytoplasm of AML patients. Analyzing these aspects will allow us to better understand the mechanisms by which WRAP53 may contribute to the development and progression of AML.
Conclusion
6
The results presented demonstrate a downregulation of WRAP53 in the sample of patients studied, indicating that this gene may be involved in other mechanisms related to AML, in addition to its correlation with hTERT identified in this study. The reported low expression of WRAP53 may negatively influence crucial mechanisms that maintain genomic stability, such as the DNA damage response (DDR), which may impact both progression and treatment efficacy in AML due to the accumulation of mutations that confer survival advantages to leukemic cells. Such further investigations may clarify the role of WRAP53 in the context of AML and its clinical impact, suggesting its potential as a promising molecular biomarker for genomic stability in AML. Furthermore, in this study, hTERT expression could not be correlated with the clinical features analyzed.
Author Contributions
R.B.G., B.M.D.N. and C.A.M.‐N. collected and analyzed data and wrote the manuscript. C.B.M., B.M.D.N., F.M.C.d.P.P., A.K.d.C.M., M.O.d.M.F., M.E.A.d.M., G.S.L., P.H.S.R., H.G.M., D.d.S.O., R.M.R., R.P.G.V., A.S.K. and C.A.M.‐N. provision of data and sub‐sequent analysis and interpretation. Writing – original draft preparation, R.B.G., B.M.D.N. and C.A.M.‐N. writing – review and editing, R.B.G., C.B.M., B.M.D.N., F.M.C.d.P.P. and C.A.M.‐N. All authors have read and agreed to published version of the manuscript.
Funding
This study was supported by Brazilian funding agencies: Coordination for the Improvement of Higher Education Personnel (CAPES; to B.M.D.N, C.B.M, F.M.C.d.P.P, I.V.B and A.K.C.M), National Council of Technological and Scientific Development (CNPq—PQ scholarships to M.O.d.M.F, A.S.K. and C.A.M.‐N.), Cearense Foundation of Scientific and Technological Support (FUNCAP; to R.B.G).
Ethics Statement
The study was approved by the ethics committee of the Federal University of Ceará and Dr. César Cals General Hospital with the following approval numbers: 4.339.719 and 5.823.921. The methods were performed in accordance with Helsinki guidelines and regulations.
Consent
Study patients provided written consent.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. Hanahan , “Hallmarks of Cancer: New Dimensions,” Cancer Discovery 12, no. 1 (2022): 31–46, 10.1158/2159-8290.CD-21-1059.35022204 · doi ↗ · pubmed ↗
- 2D. Hanahan and R. A. Weinberg , “Hallmarks of Cancer: The Next Generation,” Cell 144, no. 5 (2011): 646–674, 10.1016/j.cell.2011.02.013.21376230 · doi ↗ · pubmed ↗
- 3D. Hanahan and R. A. Weinberg , “The Hallmarks of Cancer,” Cell 100, no. 1 (2000): 57–70, 10.1016/S 0092-8674(00)81683-9.10647931 · doi ↗ · pubmed ↗
- 4M. Z. Mohamed Jiffry , R. Kloss , M. Ahmed‐khan , et al., “A Review of Treatment Options Employed in Relapsed/Refractory AML,” Hematology 28, no. 1 (2023): 1–13, 10.1080/16078454.2023.2196482.37036019 · doi ↗ · pubmed ↗
- 5E. S. Winer and R. M. Stone , “Novel Therapy in Acute Myeloid Leukemia (AML): Moving Toward Targeted Approaches,” Therapeutic Advances in Hematology 10 (2019): 204062071986064, 10.1177/2040620719860645.PMC 662491031321011 · doi ↗ · pubmed ↗
- 6M. de Oliveira Lisboa , P. R. S. Brofman , A. T. Schmid‐Braz , A. Rangel‐Pozzo , and S. Mai , “Chromosomal Instability in Acute Myeloid Leukemia,” Cancers (Basel) 13, no. 11 (2021): 2655, 10.3390/cancers 13112655.34071283 PMC 8198625 · doi ↗ · pubmed ↗
- 7E. Bulaeva , D. Pellacani , N. Nakamichi , et al., “MYC‐Induced Human Acute Myeloid Leukemia Requires a Continuing IL‐3/GM‐CSF Costimulus,” Blood 136, no. 24 (2020): 2764–2773, 10.1182/blood.2020006374.33301029 · doi ↗ · pubmed ↗
- 8R. B. Gadelha , C. B. Machado , F. M. C. d. P. Pessoa , et al., “The Role of WRAP 53 in Cell Homeostasis and Carcinogenesis Onset,” Current Issues in Molecular Biology 44, no. 11 (2022): 5498–5515, 10.3390/cimb 44110372.36354684 PMC 9688736 · doi ↗ · pubmed ↗