Different Patterns of Lichen Planus in Three Members of One Family
Bahareh Abtahi-Naeini, Maryam Khalili, Fahimeh Shirdel, Mahsa Pourmahdi-Boroujeni

TL;DR
Three siblings from one family presented with different forms of Lichen Planus, highlighting possible genetic and environmental influences.
Contribution
This case series reports a unique family with multiple LP variants, suggesting a potential genetic predisposition.
Findings
Three Iranian siblings presented with distinct LP variants: LPPigm, LPP, and FFA.
Histopathological confirmation was obtained for each case.
The family's case highlights the need for further research into LP's genetic and environmental causes.
Abstract
The pathogenesis of Lichen Planus (LP) and its variants, despite many investigative efforts, remains incompletely understood. The occurrence of the disease in siblings suggests a potential role for both genetic and shared environmental factors. Here, three Iranian siblings—one male and two females—who presented with various clinical forms of LP were introduced. Case No. 1 exhibited bilateral facial pigmentation and was diagnosed with Lichen Planus Pigmentosus (LPPigm). Case No. 2 presented with facial pigmentation accompanied by facial papules and was diagnosed with LPPigm and Lichen Planopilaris (LPP). Case No.3 had frontotemporal hairline recession and eyebrow sparsening and was diagnosed with Frontal Fibrosing Alopecia (FFA). Histopathological examination confirmed the diagnoses in all three patients. Patients were treated with an individualized plan that included sunscreen use,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
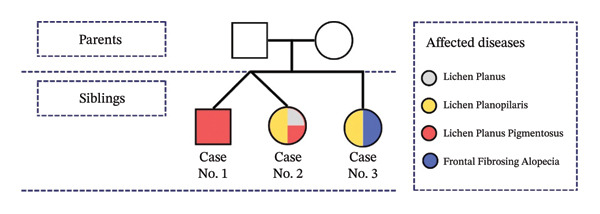 FIGURE 1
FIGURE 1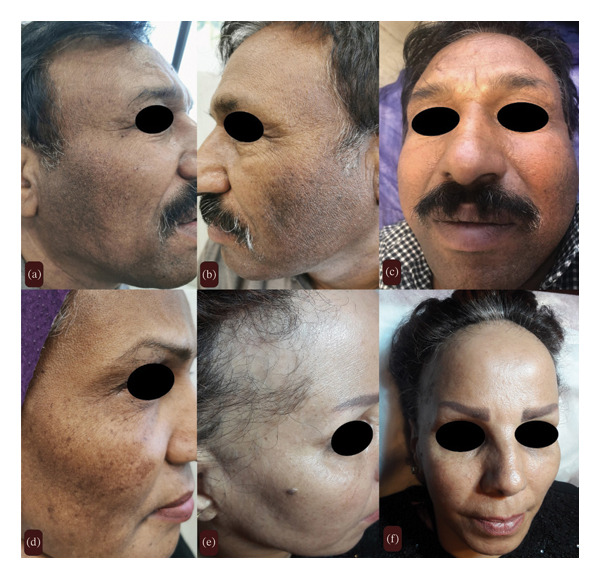 FIGURE 2
FIGURE 2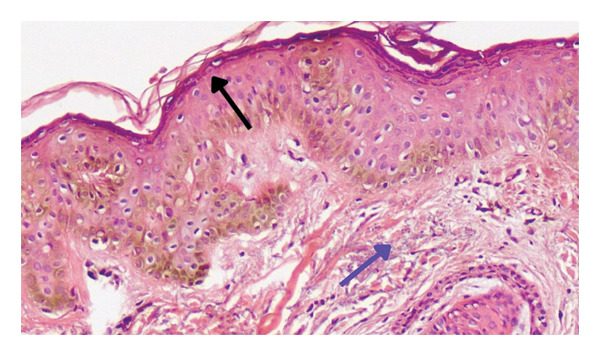 FIGURE 3
FIGURE 3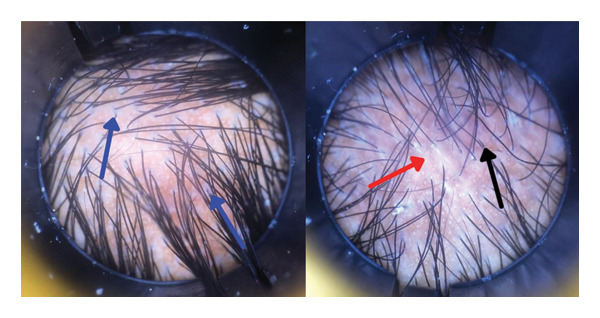 FIGURE 4
FIGURE 4| Author/year | Ethnicity | Gender–relativity | Age at diagnose | Clinical evaluation and underlying conditions | Diagnosis | HLA typing | Treatments |
|---|---|---|---|---|---|---|---|
|
Dlova et al. [ 2013 |
Italian Caucasian | M–Brother | 62 |
Eyebrow loss, body hair loss FFA |
Clinically + Biopsy Main histologic findings: erythema and scaling | Not Evaluated | NM |
| F–Sister | 59 |
Eyebrow Loss, Body Hair Loss FFA, LPP | NM | ||||
|
Rivas et al. [ 2015 | Spain | F–Mother | 67 |
Decreased hair density in male pattern, Slight eyebrows alopecia FFA Chronic Autoimmune Gastric Atrophy |
Clinically + Biopsy Main Histologic Findings: Follicular destruction, Perifollicular lymphoid cell infiltration |
HLA DR B1 ∗ 04, 13 HLA DQ B1 ∗ 03: 02, 06 | Minoxidil, Retinoic Acid, Betamethasone, Dipropionate |
| F–Daughter | 38 |
Partial Occipital Patches of Cicatricial Alopecia LPP |
Clinically + Biopsy Main Histologic Findings: Follicular destruction with fibrosis replacement, Laminated fibrotic rims around follicles, Perifollicular lymphoid cell infiltration | Tacrolimus Ointment | |||
|
Namazi et al. [ 2018 | Iranian | F–Mother & Sister | 50 |
Facial Papules, Vellus Hair LPP |
Clinically + Biopsy Main histologic findings: NM | Not Evaluated |
Hydroxychloroquine Isotretinoin |
| F–Sister | 41 |
Eyebrows alopecia, facial papules FFA, LPP |
Clinically + Biopsy main histologic findings: Perifollicular lymphoid cell infiltrate, Follicular destruction, Mild acanthosis, Focal dermal fibrosis perifollicular mucin deposition |
Hydroxychloroquine, cyclosporine, topical corticosteroids, mycophenolate mofetil, laser therapy, and finasteride Isotretinoin | |||
| F–Sister | 35 |
Facial papules, vellus hair LPP |
Clinically + Biopsy Main histologic findings: NM | Isotretinoin | |||
| M–Son | 30 |
Facial papules, bilateral beard alopecia LPP on the beard |
Clinically + Biopsy Main histologic findings: NM |
Hydroxychloroquine Isotretinoin | |||
|
Porriño‐Bustamante et al. [ 2019 | Caucasian | M–Brother | 44 |
Partial eyelashes alopecia, facial papules, total hair loss of beard, lower limbs, and forearms, Partial hair loss of axilla and pubis |
Clinically + Biopsy Main histologic findings: Perifollicular lymphoid cell infiltrate, interface dermatitis, concentric perifollicular fibrosis, follicular destruction, loss and atrophy of sebaceous glands | Not Evaluated | NM |
| M–Brother | 46 |
Partial eyelashes alopecia, facial papules, partial hair loss of beard, and all limbs, patches of scaring alopecia FFA, LPP | NM | ||||
|
Rocha et al. [ 2020 | Brazilian | F–Sister | 67 |
Eyebrow and eyelashes loss, body hair loss Diffused FFA, LPPigm | Clinically | Not Evaluated | NM |
| F–Sister | 64 |
Eyelashes and partial eyebrow loss Diffused and patchy FFA | Clinically | NM | |||
| F–Sister | 62 |
Eyelashes loss, body hair loss Diffused FFA | Clinically | NM | |||
| F–Sister | 61 |
Facial papules, eyelashes and partial eyebrow loss, body hair loss Diffused FFA Allergic rhinitis | Clinically | NM | |||
| F–Sister | 52 |
Facial papules, eyebrow loss, body hair loss Diffused FFA | Clinically | NM | |||
| F–Sister | 51 |
Facial papules, eyelashes and eyebrow loss Diffused FFA | Clinically | NM | |||
|
Ocampo‐Garza et al. [ 2021 | Spain | F–Mother | 72 |
Eyelashes and eyebrow loss, pubis hair loss, depressed frontal veins FFA Rheumatoid arthritis, surgical menopausal |
Clinically + Biopsy Main histologic findings: NM | Not Evaluated | NM |
| F–Daughter | 51 |
Facial papules, eyebrow loss, limb’s hair loss LPPigm |
Clinically + Biopsy Main histologic findings: NM | NM | |||
| Spain | F–Mother | 58 |
Facial papules, Retroauricular hairline recession, eyebrow loss, limbs and axilla hair loss, depressed frontal veins LPPigm, FFA DM, HTN, and postmenopausal |
Clinically + Biopsy Main histologic findings: NM | Not evaluated | NM | |
| F–Daughter | 39 |
Dermoscopic characteristic of FFA Autoimmune hypothyroidism |
Clinically + Biopsy Main histologic findings: NM | NM | |||
| Our cases | Iranian | M–Brother (Twin) | 56 |
Bilateral facial pigmentation Multiple round‐to‐oval blue‐gray macules Facial erythema LPPigm |
Clinically + Biopsy Main histologic findings: Basket‐wave orthokeratosis, hypergranulosis, slight acanthosis, pigmentation of the basal layer, focal hydropic change, solar degeneration, melanin incontinence | Not evaluated |
Topical corticosteroids Topical pimecrolimus |
| F–Sister (Twin) | 56 |
Facial pigmentation (LPPigm) Facial papules (LP) LPP |
Clinically + Biopsy Main histologic findings: Perifollicular hyperkeratosis, perifollicular erythema, scar formation |
Topical corticosteroids Topical pimecrolimus | |||
| F–Sister | 52 |
FFA Eyebrow loss Negative hair pull test Facial papules (LP) |
Clinically + Biopsy Main histologic findings: Perifollicular erythema, perifollicular hyperkeratosis, follicular destruction |
Topical corticosteroids Topical pimecrolimus Finasteride Topical minoxidil | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Hair Growth and Disorders · Genetic and rare skin diseases.
1. Introduction
Lichen Planus (LP) encompasses several variants, including Lichen Planopilaris (LPP), Lichen Planus Pigmentosus (LPPigm), and Frontal Fibrosing Alopecia (FFA). Despite the increasing number of reported cases, the exact causes of FFA and LPP remain unclear, although both are believed to have an immune‐mediated component [1–4].
The occurrence of familial FFA cases and the fact that FFA usually affects older individuals suggest that both genetic and environmental factors contribute to disease pathogenesis. Recent genetic investigations have provided some insights into potential pathogenic mechanisms; however, further investigation is needed for a more comprehensive understanding [5, 6].
Herein, we present three siblings from an Iranian family with different LP variants. The patients were between 50 and 60 years and had no history of other underlying diseases (Figure 1).
Pedigree diagram of a family affected by different clinical types of Lichen Planus.
2. Case Presentation
2.1. Case 1
A 56‐year‐old male, Fitzpatrick skin Type 4, was referred to an outpatient dermatology clinic with a chief complaint of bilateral facial pigmentation. Pigmentation began about 2 years prior, without preceding facial erythema or pruritus. On facial examination, symmetrical round‐to‐oval blue‐gray macules and patches were observed on the lateral aspect of cheeks and beard (Figure 2). There was no other site of involvement or any facial papules.
Three siblings with multivariant forms of Lichen Planus: (a–c) 56‐year‐old man with bilateral facial pigmentation and multiple round‐to‐oval blue‐gray macules with the final diagnosis of Lichen Planus Pigmentosus. (d) 56‐year‐old woman with facial papules and facial pigmentation with the final diagnosis of Lichen Planus Pigmentosus and Lichen Planopilaris. (e, f) 52‐year‐old woman with frontotemporal hairline recession, eyebrow loss, and facial papules with the final diagnosis of frontal fibrosing alopecia and Lichen Planus.
Since childhood, he has had frequent sun exposure without sufficient sun protection. He was a smoker but had no other specific underlying condition. The medication history was unremarkable. Initially, with a diagnosis of melasma, multiple topical whitening treatments, such as hydroquinone, were prescribed. However, there was no significant clinical response, and the pigmentation worsened.
Therefore, with clinical differential diagnoses of LPPigm, melasma, drug‐induced hyperpigmentation, postinflammatory hyperpigmentation, and pigmented contact dermatitis, a 4‐mm punch biopsy was obtained from the face. Histopathological evaluation showed basket‐wave orthokeratosis, hypergranulosis, slight acanthosis, pigmentation of the basal layer, focal hydropic change, solar degeneration, and melanin incontinence, compatible with the diagnosis of facial LPPigm (Figure 3).
Skin biopsy of a 56‐year‐old man with Lichen Planus Pigmentosa: hyperpigmentation of the basal layer (black arrow), focal hydropic change, basket‐wave orthokeratosis, hypergranulosis, slight acanthosis, solar degeneration (blue arrow), and melanin incontinent (hematoxylin and eosin; magnification: × 10).
According to the diagnosis, treatment with topical potent corticosteroids was started and continued periodically. Pimecrolimus cream was also prescribed twice daily for application to the pigmented area. The patient was also reminded of the importance of frequent sunscreen use. At the 9‐month follow‐up, the pigmentation area remained stable, and disease progression had stopped.
2.2. Case 2
A 56‐year‐old postmenopausal female patient with Fitzpatrick Type 4 skin, who was the twin sister of Case No. 1, presented with a chief complaint of facial pigmentation. Pigmentation began about 5 years prior, and despite using multiple topical bleaching agents and undergoing laser‐assisted melasma treatment, no clinical response was observed, similar to her brother. Additionally, she had scalp erythema and pruritus, which began 2 years prior and were associated with facial monomorphic papules (Figure 1).
Trichoscopy examination revealed perifollicular hyperkeratosis, perifollicular erythema, and a small area of scar formation (Figure 4). There was no eyelash or eyebrow involvement. The histopathological examination of the facial pigmentation was compatible with the diagnosis of LPPigm. Therefore, the patient was considered LPPigm, associated with LPP (based on the scalp involvement) and a facial LP papule. The treatment was similar to his brother’s, with potent topical corticosteroids and pimecrolimus cream. During follow‐up, perifollicular hyperkeratosis and erythema gradually decreased, and the facial papules resolved. For the pigmented areas, tranexamic acid injections were administered, resulting in approximately 50% improvement in pigmentation. At the 9‐month follow‐up, the condition had entered remission.
Trichoscopy examination of a 56‐year‐old woman with Lichen Planus Pigmentosus and Lichen Planopilaris: perifollicular hyperkeratosis and white scale (blue arrow), perifollicular erythema (black arrow), and a small area of scar formation (red arrow).
2.3. Case 3
A 52‐year‐old postmenopausal woman with Fitzpatrick Type 3 skin, and the sister of the other two patients, presented with a 5‐year history of symmetric, band‐like frontotemporal hairline recession and partial eyebrow sparsening. The affected scalp appeared shiny and smooth, and the hair pull test was negative. Dermoscopic examination of the frontotemporal region revealed a marked reduction in follicular ostia along with perifollicular erythema, scaling, and hyperkeratosis (Figure 2). She also had facial papules; however, examination of the oral and genital mucosae, nails, and the rest of the body showed no abnormalities.
A skin biopsy confirmed the diagnosis of LPP. Based on the clinical presentation, trichoscopic findings, and histopathology, the patient was diagnosed with FFA associated with LPP. She was treated with finasteride (5 mg/day) and topical minoxidil. Periodic topical clobetasol and pimecrolimus cream were also prescribed for the facial papules. At the 9‐month follow‐up, alopecia progression had stopped with no hair growth in the frontotemporal region, and the condition had entered remission.
Notably, both parents passed away years ago. Given the absence of detailed medical examinations, their health status and the presence of any lichenoid mucocutaneous condition cannot be definitively determined. Additionally, there were no more siblings in their family.
3. Discussion
Here, we presented three siblings who were diagnosed with various forms of LP, including FFA, LPP, and LPPigm. In Case No. 1, LPPigm manifested as bilateral, symmetrical blue‐gray macules and patches confined to the face, without papules or scalp involvement. In Case No. 2, LPPigm manifested as bilateral facial pigmentation. Also, Case No. 2 presented facial papules compatible with the diagnosis of LP, as well as LPP of the scalp, characterized by perifollicular erythema, hyperkeratosis, and scarring alopecia on trichoscopy. Case No. 3 presented with the features of FFA, including band‐like frontotemporal hairline recession and scalp LPP, similar to Case No. 2. Although the coexistence of these diseases has been reported in one patient [7], a family with such variants of LP has not been reported so far.
The occurrence of familial LP with multivariant forms suggests a possible role for both genetic and environmental factors in the etiopathogenesis of the LP spectrum. Upon the literature search, reports of eight families with multivariant forms of LP, emphasizing FFA and LPP, were noted. Table 1 presents clinical evaluations, diagnoses, other underlying diseases, HLA typing, and treatments of these families (Table 1).
FFA presents with a gradual frontotemporal hairline recession accompanied by eyebrow alopecia. In contrast, classic LPP shows irregular areas of alopecia in the vertex region without a characteristic band‐like distribution seen in FFA [2]. FFA and LPP are generally considered different clinical presentations within the same disease spectrum. The findings in both conditions demonstrate follicular destruction with a lymphocytic infiltrate targeting the isthmus and infundibulum of the hair follicles, apoptotic cells within the external root sheath, and concentric perifollicular fibrosis resulting in scarring alopecia. Notably, FFA tends to show less follicular inflammation and a higher rate of apoptotic cells. On the other hand, in some LPP cases, the inflammatory infiltrate may extend into the interfollicular epidermis. Direct immunofluorescence (DIF) study of the FFA biopsies typically shows no specific findings. In contrast, LPP biopsies demonstrate globular deposits, cytoid bodies (usually IgM), as well as irregular fibrinogen and complement deposition within the papillary dermis adjacent to the follicular epithelium [8].
LPPigm presents as acquired asymmetric pigmented macules, predominantly affecting sun‐exposed areas. It commonly affects dark‐skinned patients, particularly those from India and the Middle East. In Table 1, the majority of the described cases were Caucasian patients (Table 1). Further investigations are needed to clarify the role of ethnicity as a whole genetic component. Key histopathological features include hyperkeratosis, basal cell vacuolar degeneration, epidermal thinning, perivascular infiltrates, pigment incontinence, and band‐like lichenoid infiltrates [7, 9]. In the current study, Cases No. 1 and No. 2—both with relatively darker skin—had LPPigm, and Case No. 2 also presented with LPP and LP. Case No. 3 exhibited FFA without the features of LPPigm. Nevertheless, the coexistence of FFA and LPPigm has been reported previously [2].
Studies show that HLA‐DR1 plays a significant role in the pathogenesis of LP and Lassueur–Graham–Little–Piccardi syndrome. Nevertheless, such concurrency is not reported in FFA. HLA B^∗^07:02 is one of the most prevalent alleles in FFA cases [6]. Table 1 represents the HLA findings of the included families with multivariant forms of LP (Table 1). Unfortunately, due to resource limitations, our cases did not undergo any genome typing.
Hormonal factors are other predisposing factors that may contribute to the pathogenesis of FFA [10]. The predominance of FFA among elderly postmenopausal women, as demonstrated in Table 1, supports this hypothesis (Table 1). In our cases, Cases No.2 and No.3 were postmenopausal women. Moreover, finasteride—a 5‐alpha‐reductase inhibitor—has been shown in some cases to stop disease progression [11]. Therefore, Case No. 3 planned to receive finasteride, which successfully stopped disease progression.
There are reports of autoimmune diseases occurring concurrently with FFA and LPP, including vitiligo, autoimmune thyroid disorders, and autoimmune gastritis. Chronic diseases associated with immune dysregulation may also play an important role [3, 10]. In addition, several exogenous factors have been proposed to play a role in the pathogenesis of LP and its variants, including Hepatitis C virus, human immunodeficiency virus, herpes simplex Virus 2*, Helicobacter pylori*, human papillomavirus, and syphilis [9, 12, 13]. In our cases, the coexistence of LP variants and no other autoimmune or underlying systemic disease was identified.
In conclusion, this report highlights the possibility of familial LP with multivariant forms, suggesting the involvement of genetic and environmental factors in the etiopathogenesis of the disease.
Author Contributions
Bahareh Abtahi‐Naeini: conceptualization, supervision, project administration, and writing–review and editing.
Maryam Khalili: conceptualization, resources, validation, and writing–review and editing.
Fahimeh Shirdel: methodology, investigation, and writing–review and editing.
Mahsa Pourmahdi‐Boroujeni: investigation, visualization, writing–original draft, and writing–review and editing.
All authors have revised the manuscript critically for important intellectual content and confirmed the accuracy or integrity of any parts of the work.
Funding
The authors received no specific funding for this work.
Disclosure
We declare that none of the authors are employed by a government agency that has a primary function other than research and/or education. None of the authors have an official representative on behalf of the government. All authors have read and approved the content of the manuscript.
Ethics Statement
The Ethics Committee of the Isfahan University of Medical Sciences in Isfahan, Iran, approved this report’s ethical content (IR.ARI.MUI.REC.1402.195). Participation in the study was contingent upon signing a written informed consent form signed by all the patients. Written informed consent was obtained from all three patients for publication of the details of their medical case and any accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dlova N. , Goh C. L. , and Tosti A. , Familial Frontal Fibrosing Alopecia, British Journal of Dermatology. (2013) 168, no. 1, 220–222, 10.1111/j.1365-2133.2012.11101.x, 2-s 2.0-84872837948.22716508 · doi ↗ · pubmed ↗
- 2Fechine C. O. C. , Valente N. Y. S. , and Romiti R. , Lichen Planopilaris and Frontal Fibrosing Alopecia: Review and Update of Diagnostic and Therapeutic Features, Anais Brasileiros de Dermatologia. (2022) 97, no. 3, 348–357, 10.1016/j.abd.2021.08.008.35379508 PMC 9133245 · doi ↗ · pubmed ↗
- 3Ocampo-Garza S. S. , Orizaga Y. Q. T. L. , Olvera-Rodríguez V. et al., Frontal Fibrosing Alopecia: Is There a Link in Relatives?, Skin Appendage Disorders. (2021) 7, no. 3, 206–211, 10.1159/000512039.34055909 PMC 8138245 · doi ↗ · pubmed ↗
- 4Robles-Méndez J. C. , Rizo-Frías P. , Herz-Ruelas M. E. , Pandya A. G. , and Ocampo Candiani J. , Lichen planus Pigmentosus and Its Variants: Review and Update, International Journal of Dermatology. (2018) 57, no. 5, 505–514.29076159 10.1111/ijd.13806 · doi ↗ · pubmed ↗
- 5Porriño-Bustamante M. L. , López-Nevot M. , Aneiros-Fernández J. , García-Lora E. , Fernández-Pugnaire M. A. , and Arias-Santiago S. , Familial Frontal Fibrosing Alopecia: A Cross-Sectional Study of 20 Cases From Nine Families, Australasian Journal of Dermatology. (2019) 60, no. 2, e 113–e 118.30430555 10.1111/ajd.12951 · doi ↗ · pubmed ↗
- 6Rocha V. B. , Pires M. C. , and Contin L. A. , Familial Fibrosing Frontal Alopecia in Six Sisters, Anais Brasileiros de Dermatologia. (2020) 95, no. 1, 125–128, 10.1016/j.abd.2019.02.009.31932160 PMC 7058864 · doi ↗ · pubmed ↗
- 7Walker J. L. , Robinson-Bostom L. , and Landow S. , Four Diseases, Two Associations, One Patient: A Case of Frontal Fibrosing Alopecia, Lichen planus Pigmentosus, Acne Rosacea, and Morbihan Disease, Skinmed. (2016) 14, no. 3, 225–228.27502265 · pubmed ↗
- 8Poblet E. , Jiménez F. , Pascual A. , and Piqué E. , Frontal Fibrosing Alopecia Versus Lichen Planopilaris: A Clinicopathological Study, International Journal of Dermatology. (2006) 45, no. 4, 375–380, 10.1111/j.1365-4632.2006.02507.x, 2-s 2.0-33645540135.16650161 · doi ↗ · pubmed ↗