Age-related changes of the tibial nerve cross-sectional area in the disabled elderly
Kholoud J. Sandougah, Mohamed A. Bedewi, Saeed M. Alamri, Nawaf A. Alzain, Abdulrahman A. Alharthi, Mohammed Ayesh Zayed, Mohamed Sherif El-Sharkawy, Saleh M. Alfawaz, Husain Alturkistani, Elsayed Abbas Beheri, Rasha Ali, Muneerah Al-Aqeel, Sitah F. Alanazi, Mohammad W. Marashdeh

TL;DR
This study examines how the cross-sectional area of the tibial nerve changes with age and disability in elderly individuals.
Contribution
The study provides empirical evidence on tibial nerve cross-sectional area differences in disabled versus non-disabled elderly populations.
Findings
The mean tibial nerve cross-sectional area was largest in disabled elderly patients (28.5 mm²).
Nerve ultrasound may be a useful tool for assessing tibial nerve changes in disabled elderly individuals.
Abstract
This study aims to assess changes in the cross-sectional area of the tibial nerve in the disabled elderly. The study sample included 124 tibial nerves in 62 participants; 16 of which were disabled elderly patients (13 males, 3 females), with a mean age of 66.6, a mean height of 167.1 cm, a mean weight of 83.9 kg, and a mean BMI of 29.9. Twenty-three young controls (6 males, 17 females), a mean age of 48.4, a mean height of 154.9 cm, a mean weight of 79.8 kg, a mean BMI of 32.7, and 23 elderly non-disabled participants (13 males, 10 females), a mean age of 63.6, a mean height of 161.9 cm, a mean weight of 80.56 kg, and a mean BMI of 30.88. The mean CSA of the TN in the elderly disabled group was 28.5 mm2. The mean CSA of the young control group’s TN was 20.45 mm2. The mean CSA of the TN in the elderly non-disabled group (both diabetic and non-diabetic) was 27.6 mm2. The mean CSA of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
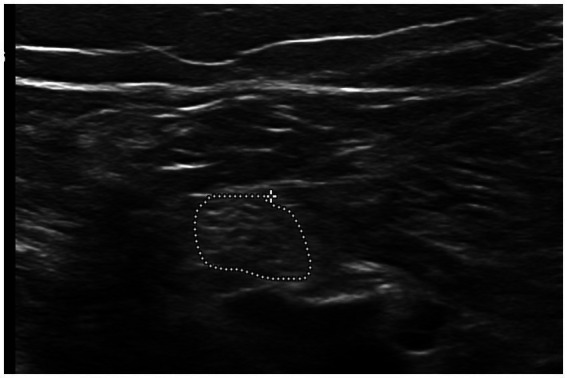 Figure 1
Figure 1| Variable | Control aged >60 ( | Control aged <60 ( | Elderly disabled ( | ||||
|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % | ||
| Gender | |||||||
| Male | 13 | 56.52% | 6 | 26.08% | 13 | 81.25% | |
| Female | 10 | 43.47% | 17 | 73.91 | 3 | 18.75% | |
| Age (years) | (63.60 ± 4.93) | (48.43 ± 5.85) | (66.62 ± 4.16) | <0.001 | |||
| Height (cm) | (161.91 ± 9.11) | (154.93 ± 6.48) | (167.12 ± 9.20) | <0.001 | |||
| Weight (kg) | (80.56 ± 15.88) | (79.80 ± 14.64) | (83.91 ± 14.15) | 0.306 | |||
| Body mass index (kg/m2) | (30.88 ± 5.36) | (32.70 ± 5.73) | (29.98 ± 4.25) | 0.211 | |||
| Variable | Control aged >60 ( | DM ( | Non-DM ( | Control aged <60 ( | Elderly disabled ( | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % |
| % |
| % | ||
| Mean± SD | Mean± SD | Mean± SD | Mean± SD | Mean± SD | |||||||
| Cross sectional area | (27.66 ± 8.00) | (29.99 ± 9.05) | (24.64 ± 5.18) | (20.45 ± 7.97) | (28.55 ± 9.92) | <0.001 | |||||
| Correlation | TIB nerve | Age | Height | Weight | BMI | |
|---|---|---|---|---|---|---|
| TIB nerve | Pearson correlation | 1 | 0.025 | −0.086 | −0.414 | −0.459 |
| Sig. (2-tailed) | 0.927 | 0.750 | 0.110 | 0.074 | ||
| Group | Mean difference | Sig. | 95% Confidence interval | ||
|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||
| G 1.00 | 2.00 | 7.19* | 0.000 | 2.83 | 11.55 |
| 3.00 | −0.88 | 1.000 | −5.73 | 3.96 | |
| G 2.00 | 1.00 | −7.19* | 0.000 | −11.55 | −2.83 |
| 3.00 | −8.07* | 0.000 | −12.97 | −3.18 | |
| G 3.00 | 1.00 | 0.88 | 1.000 | −3.96 | 5.73 |
| 2.00 | 8.07* | 0.000 | 3.18 | 12.97 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Nutrition and Health in Aging · Lower Extremity Biomechanics and Pathologies
Introduction
Disability in the elderly population is a complex, multidimensional subject. The disabled elderly population face long-term physical, mental problems, and sensorimotor difficulties, which could cause partial or full restriction of social engagement (1–4). Many of these patients suffer from neuromuscular symptoms with weakness/atrophy of the skeletal muscles and/or changes in the peripheral nerve morphology. The presence of polyneuropathies, especially those related to chronic disease, can be disabling for the elderly (5). In the past, the diagnosis of chronic polyneuropathies was mainly based on clinical assessment and nerve conduction studies (6). Recently, musculoskeletal ultrasound has emerged as an efficient imaging tool in the diagnosis of different neuromuscular disorders (7, 8). The tibial nerve is one of the two branches of the sciatic nerve and was successfully used for the assessment of chronic peripheral nerve disease (9–12). Ultrasound is a cheap imaging tool with dynamic capability, without risk of ionizing radiation, with shorter acquisition time compared to MRI, and with the capability of bilateral examination (13). The cross-sectional area (CSA) is an important sonographic parameter for differentiation of normal and abnormal nerves (14). This study aims to assess the CSA changes of the tibial nerve in disabled elderly patients.
Methods
Participants
After institutional review board approval, participants for the study were recruited between February 2025 and May 2025, and written consent was obtained. A total of 16 elderly patients with different types of motor disability were recruited to a teaching university hospital. Inclusion criteria included elderly patients at least 60 years old with motor disabilities (DE). This group of four cases is due to motor disability due to cerebrovascular disease, four cases due to spinal acquired and congenital causes, five cases due to chronic peripheral vascular causes, two cases due to muscular degenerative and dystrophic diseases, and one case due to chronic peripheral nerve disease. Patients with temporary disability were excluded.
A second group included elderly patients at least 60 years old without motor disability, non-disabled elderly (NDE); these were subdivided into diabetic (type II) and non-diabetic. A nerve conduction study was performed on a quarter of the participants. The third group included healthy subjects below 60 years old. For each participant, data including age, sex, BMI, weight, and height were recorded.
Technique
We used an L12–5 MHz linear transducer (Epic 7 version 1.5, Ultrasound system: Philips, Bothell, WA, USA). All participants were scanned by a radiologist (M.B.) with 13 years’ experience in neuromuscular ultrasonography. Each nerve was scanned three times, with the ultrasound probe removed from the skin in between. The tibial nerve was scanned in the popliteal fossa after division from the sciatic nerve and posterior to the popliteal artery and vein, and then the CSA was measured in mm^2^. The CSA of the TN was measured inside the hyperechoic epineurium using the tracer method; minimal pressure was exerted on the probe to optimize image quality (Figure 1).
Short axis scan of the tibial nerve at the popliteal fossa, with measurement taken using the tracer method.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 27 software (SPSS Inc., Chicago, IL, USA). All data were presented as mean, standard deviation (SD), and range. The Shapiro–Wilk test was used to assess the normality of the data distribution. The correlations between the CSA of the scanned nerves, age, weight, height, and BMI were evaluated using Pearson’s correlation coefficient (r). A p-value of <0.05 was considered significant. The ANOVA test was used to compare CSA between different groups. An ANCOVA test was performed to control for confounding variables.
Results
The study sample included 124 tibial nerves in 62 participants; 16 of them were disabled elderly patients (13 males, 3 females), mean age 66.6 ± 4.16, mean height 167.1 cm ± 9.2, mean weight 83.9 kg ± 13.1, mean BMI 29.9 ± 4.2; 23 young controls (6 males, 17 females), mean age 48.4 ± 5.8, mean height 154.9 cm ± 6.48, mean weight 79.8 kg ± 13.1, mean BMI 32.7 ± 4.2; and 23 elderly non-disabled participants (13 males, 10 females), mean age 63.6 ± 4.93, mean height 161.9 cm ± 9.11, mean weight 80.56 kg ± 15.88, and mean BMI 30.88 ± 5.3 (Table 1). The intra-observer reliability calculations resulted in an overall intra-class correlation coefficient of 0.88. The mean CSA of the TN in the elderly disabled group was 28.5 mm^2^ ± 9.9. The mean CSA of the young control group TN was 20.45 mm^2^ ± 7.9. The mean CSA of the TN in the elderly non-disabled group (both diabetic and non-diabetic) was 27.6 mm^2^ ± 8. The mean CSA of the TN in the elderly diabetic non-disabled group was 29.9 mm^2^ ± 9. The mean CSA of the TN in the elderly (non-diabetic) non-disabled group was 24.6 mm^2^ ± 5.1 (Table 2). The TN CSA in the non-disabled elderly group (NDE) showed moderate negative correlation with weight (p = 0.110) and BMI (p = 0.074). Otherwise, all three groups showed no significant statistical correlation with all other demographic factors (Table 3). One-way ANOVA and post-hoc Bonferroni test results are presented in Table 4.
Discussion
In our study, the tibial nerve CSA in the disabled elderly group (28.5 mm^2^) was larger compared to the control young population group (20.45 mm^2^), and was also increased compared to other studies in the literature, such as Kerasnoudis et al. (8.43 mm^2^), Soek et al. (24.4 mm^2^), Fisse et al. (25.9 mm^2^) (15–17). The TN CSA in the elderly disabled group was also larger than the elderly non-disabled non-diabetic group (24.6 mm^2^); however, the elderly disabled group showed slightly lower values than the elderly diabetic non-disabled group (29.9 mm^2^). Analyzing our data with the ANOVA test and the ANCOVA model revealed that the difference in CSA between the disabled elderly group and the control young group was not statistically significant, and that none of the covariates (age, weight, height, BMI) could be significant predictors of tibial nerve CSA. This means that after controlling for confounding variables, the difference between these two was attenuated. Our results suggest an increase in CSA of the TN in disabled elderly patients in comparison to the control groups, except diabetic patients. The CSA of the TN in diabetic patients is reported in the literature to be increased in comparison to healthy controls. Diabetic patients with polyneuropathy are also reported to have higher CSA compared to both healthy controls and diabetic patients without polyneuropathy (18). The similarity in CSA (p < 0.05) between the elderly disabled group and the elderly diabetic non-disabled group could suggest a more influential role of aging and diabetes on CSA enlargement rather than disability itself as a sole factor. This study has several limitations. First, it is the small sample size. Second, a major limitation is the heterogeneity of the sample of the disabled elderly group, including a variety of patients with uneven distribution of nerve involvement. Third, examining the TN was challenging in some cases of disability due to the body habitus of some patients. In conclusion, although our study suggested that nerve ultrasound could be a helpful tool for assessment of the tibial nerve in disabled elderly patients, disability status was not an independent predictor of tibial nerve CSA. Future studies with a larger sample size and a homogenous group are suggested.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Azevedo GA Sampaio RR Filho ASN Moret MA Murari TB. Sustainable urban mobility analysis for elderly and disabled people in São Paulo. Sci Rep. (2021) 11:791. doi: 10.1038/s 41598-020-80906-w 33436990 PMC 7804089 · doi ↗ · pubmed ↗
- 2Chen Y Sloan FA. Explaining disability trends in the U.S. elderly and near-elderly population. Health Serv Res. (2015) 50:1528–49. doi: 10.1111/1475-6773.12284, 25655273 PMC 4600360 · doi ↗ · pubmed ↗
- 3Hanewinckel R van Oijen M Ikram MA van Doorn PA. The epidemiology and risk factors of chronic polyneuropathy. Eur J Epidemiol. (2016) 31:5–20. doi: 10.1007/s 10654-015-0094-6, 26700499 PMC 4756033 · doi ↗ · pubmed ↗
- 4Widerström-Noga E Finlayson ML. Aging with a disability: physical impairment, pain, and fatigue. Phys Med Rehabil Clin N Am. (2010) 21:321–37. doi: 10.1016/j.pmr.2009.12.010, 20494280 · doi ↗ · pubmed ↗
- 5Granger A Zakin E. Immunotherapy for peripheral nerve disorders. Clin Geriatr Med. (2021) 37:347–59. doi: 10.1016/j.cger.2021.01.007, 33858615 · doi ↗ · pubmed ↗
- 6Taams NE Drenthen J Hanewinckel R Ikram MA van Doorn PA. Age-related changes in neurologic examination and sensory nerve amplitude in the general population: aging of the peripheral nervous system. Neurology. (2023) 101:e 1351–8. doi: 10.1212/WNL.0000000000207665, 37541844 PMC 10558170 · doi ↗ · pubmed ↗
- 7Baute Penry V Cartwright MS. Neuromuscular ultrasound for peripheral neuropathies. Semin Neurol. (2019) 39:542–8. doi: 10.1055/s-0039-1688987, 31639837 · doi ↗ · pubmed ↗
- 8Le Corroller T. High-resolution ultrasound of peripheral nerve disorders. Semin Musculoskelet Radiol. (2024) 28:708–17. doi: 10.1055/s-0044-1790528, 39561752 · doi ↗ · pubmed ↗