Melanotrichoblastoma misdiagnosed as basal cell carcinoma: a case report
Meng Zhang, Ruiqi Chu, Shengni Zhang, Chunmei Liu, Lihui Bian, Xiangxiang Ren

TL;DR
A rare skin tumor called melanotrichoblastoma was mistaken for a different type of cancer, but was correctly identified through detailed tissue analysis.
Contribution
This case report clarifies the diagnostic distinction between melanotrichoblastoma and basal cell carcinoma using histopathological features.
Findings
Melanotrichoblastoma can resemble basal cell carcinoma clinically and under dermoscopy.
Absence of retraction clefts in histopathology is a key feature distinguishing melanotrichoblastoma from basal cell carcinoma.
Complete excision of the tumor led to no recurrence after two years.
Abstract
Melanotrichoblastoma (MTB) is an exceptionally rare benign adnexal tumor with follicular differentiation. Its clinical and dermoscopic resemblance to pigmented basal cell carcinoma (BCC) often leads to misdiagnosis. A 51-year-old male presented with a slow-growing, blue-black nodule on the right canthus that had been present for five decades, with recent central ulceration. Dermoscopy revealed homogeneous pigmentation with atypical blue-white areas and dilated vessels, suggestive of BCC. Histopathological examination showed well-demarcated dermal nests of basaloid cells with peripheral palisading and stromal pigment deposition. Importantly, retraction clefts were absent, a key feature distinguishing MTB from BCC. The lesion was completely excised, with no recurrence after two years. This case highlights the diagnostic challenge of MTB. Histopathology remains the gold standard for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
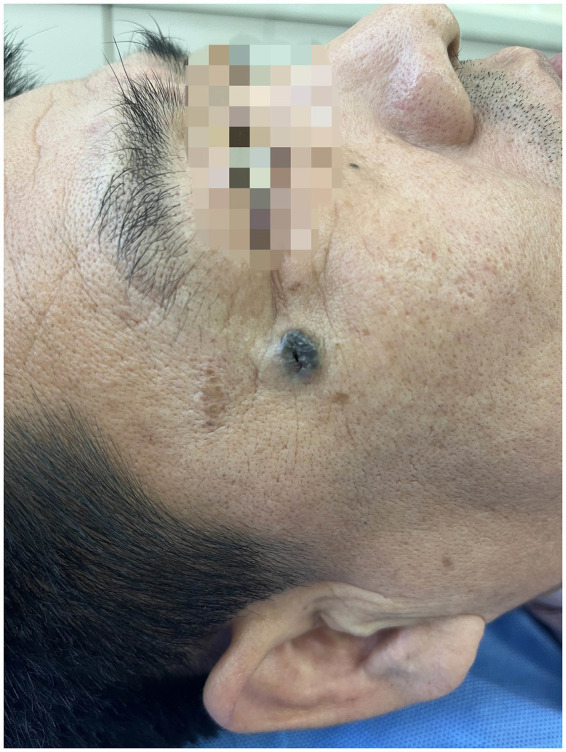 Figure 1
Figure 1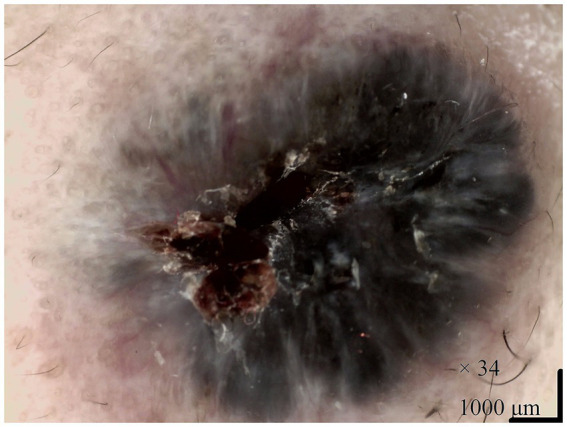 Figure 2
Figure 2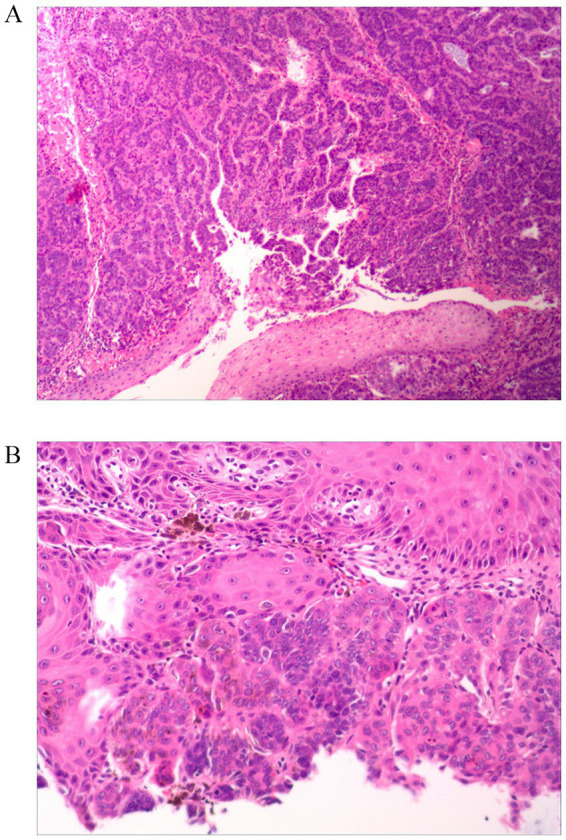 Figure 3
Figure 3| Case No. | Reference (Source document) | Age (years) | Sex | Tumor location | Size (cm) | Associated with Nevus Sebaceus? | Key characteristics |
|---|---|---|---|---|---|---|---|
| 1 | Kanitakis et al. ( | 32 | Female | Scalp | 2.0 | No | First reported case; heavy melanin deposits; dendritic melanocytes (S100+, tyrosinase+, MART-1/HMB45+); clinically mimicking blue nevus or melanoma |
| 2 | Kim et al. ( | 51 | Male | Back | 6.0 | No | Giant subcutaneous MTB; Melan-A+, HMB45+, S-100+; differential diagnosis from BCC emphasized |
| 3 | Hung et al. ( | 31 | Male | Scalp | 1.0 | Yes | Ripple-pattern MTB within nevus sebaceus; HMB45 + dendritic melanocytes; blue-black nodule |
| 4 | Mizuta et al. ( | 72 | Female | Right lower leg | Approx. 11.0 | No (collision with SK) | Collision tumor with seborrheic keratosis; dermoscopy: blue-gray ovoid nest + white structures; no recurrence at 26 months |
| 5 | Ocanha-Xavier et al. ( | 59 | Female | Scalp | 0.8 | No | Sixth formally reported case; basaloid nests with pigment; CK AE1/AE3+, Melan-A+; asymptomatic |
| 6 | Stoyanov et al. ( | 51 | Female | Mons pubis | 2.0 | No | First reported on pelvic girdle; clinically resembled ingrown hair; IHC: CK AE1/AE3+, BerEP4+, Melan-A+, HMB45+ |
| 7 | Thekho et al. ( | 33 | Female | Scalp | 4.0 | Yes | Arising in nevus sebaceus; slow-growing pigmented tumor; IHC: S100+, HMB45 + dendritic melanocytes |
| 8 | Present case | 51 | Male | Right canthus | Approx. 1.0 | No | Ulcerated blue-black nodule; dermoscopy: blue-white structures + vessels; histology: basaloid nests with pigment, NO retraction clefts; confirmed MTB; no recurrence at 24 months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Hedgehog Signaling Pathway Studies · Nonmelanoma Skin Cancer Studies
Introduction
Cutaneous adnexal tumors comprise a diverse group of neoplasms with differentiation toward skin appendages. Among them, trichoblastoma (TB) is a rare, benign tumor thought to originate from follicular germinative cells. Melanotrichoblastoma (MTB) is an exceptionally uncommon pigmented variant. It typically presents as a slow-growing, firm nodule on the head or neck of middle-aged to older adults, though its clinical appearance is often non-specific. MTB poses a significant diagnostic challenge because its dark coloration and dermoscopic features frequently mimic the far more prevalent pigmented basal cell carcinoma (BCC) (1, 2). This overlap often leads to misdiagnosis. Accurate distinction is clinically paramount, given their differing biological behavior and management. BCC, a malignant neoplasm, may require extensive surgery with margin assessment, whereas MTB is benign and cured by simple, complete local excision. Histopathological examination is the definitive diagnostic tool, with key discriminators including the architectural pattern of basaloid cells, the presence or absence of stromal retraction clefts, and immunohistochemical profiles. This case report of an MTB initially misdiagnosed as BCC underscores the importance of considering this rare entity in the differential diagnosis of pigmented skin tumors.
Case presentation
A 51-year-old male presented to our outpatient department with a long-standing skin lesion on the posterior aspect of the right canthus. The lesion, present for 50 years, had recently ulcerated. The patient reported that a millet-sized black papule had appeared during childhood and had gradually enlarged over decades without treatment. In recent months, central ulceration developed without significant pain or pruritus. His past medical and family history were unremarkable.
Physical examination revealed the patient to be in good general condition. Dermatological examination showed a well-defined, firm, blue-black nodule, approximately 1.0 cm × 1.0 cm in size, located posterior to the right canthus. The center was darker and exhibited a depressed ulceration (Figure 1). The nodule was mobile and non-tender. Dermoscopy revealed a largely symmetrical, black raised structure with relatively regular borders. It displayed homogeneous pigmentation with atypical blue-white structures, a central blood crust, and surrounding dilated vessels (Figure 2). We made a preliminary diagnosis of “Basal Cell Carcinoma?” and performed a skin biopsy.
Clinical presentation of the lesion. A well-circumscribed, firm, blue-black nodule located posterior to the right canthus. Note the central ulceration and darker coloration in the center compared to the edges.
Dermoscopic examination of the lesion. The image shows a symmetrical, black raised structure with relatively regular borders. Key features include homogeneous pigmentation, atypical blue-white structures, a central blood crust, and surrounding dilated vessels.
Histopathological examination revealed well-defined nests and cords of basaloid cells within the dermis. The cells showed no significant atypia and had oval or cuboidal shapes with basophilic nuclei. Peripheral palisading was observed at the nests’ periphery. The tumor nests were separated by collagen fibers with prominent pigment deposition. Notably, retraction clefts between the tumor nests and the surrounding stroma were absent (Figure 3). These histopathological findings, particularly the lack of retraction clefts, were inconsistent with the initial clinical and dermoscopic impression of BCC and confirmed the diagnosis of melanotrichoblastoma. The lesion was completely excised via superficial mass resection. The postoperative wound healed well, and no recurrence was observed during a two-year follow-up period.
Histopathological findings (hematoxylin and eosin staining). (A) Low-power view (40x) showing well-demarcated nests and cords of basaloid cells within the dermis, separated by fibrous stroma. The epidermis is uninvolved. (B) High-power view (200x) of a tumor nest demonstrating basaloid cells with peripheral palisading and abundant stromal pigment deposition. Critically, there is an absence of retraction clefts between the tumor nests and the surrounding stroma.
Discussion
We report a case of melanotrichoblastoma initially misdiagnosed as pigmented basal cell carcinoma due to its prolonged history, ulcerated nature, and suspicious dermoscopic features. This case epitomizes a well-recognized diagnostic challenge in dermatology and dermatopathology. Although MTB is a benign tumor, its clinical and dermoscopic presentation can strikingly mimic the more common and malignant BCC (1, 3). To the best of our knowledge, only seven cases of MTB have been previously reported in the English literature (Table 1), making our case the eighth documented instance and further underscoring its rarity.
In addition to pigmented basal cell carcinoma, the preoperative differential diagnosis included melanoma, pigmented trichoblastoma, pigmented seborrheic keratosis, and vascular lesions such as traumatic angiokeratoma. Although the lesion appeared blue-black with ulceration clinically, melanoma was considered. However, it was not the primary diagnostic consideration based on the following: dermoscopy revealed none of the typical structures of melanoma (such as an irregular pigment network, pseudopods, or radial streaming), and the lesion demonstrated an extremely slow growth pattern over 50 years—a clinical course more suggestive of a benign or low-grade malignant process. Nevertheless, melanoma should always be considered in the differential diagnosis of any pigmented nodule, with definitive diagnosis relying on histopathological examination. Traumatic angiokeratoma often presents as a blue-black papule or nodule, typically located in trauma-prone areas such as the extremities, and may appear dark due to hemorrhage. Dermoscopy usually reveals red to blue-black lacunar structures, which differ from the homogeneous pigmentation and vascular patterns observed here. The final histopathological diagnosis was melanotrichoblastoma. Key distinguishing features from other conditions include the presence of stromal retraction clefts, degree of cellular atypia, and the immunohistochemical expression profile.
The diagnostic dilemma in our patient was compounded by ulceration, an uncommon feature in TB/MTB that typically raises suspicion for malignancy (4–9). Furthermore, the dermoscopic findings—including homogeneous pigmentation, atypical blue-white structures, and dilated vessels (Figure 2)—are highly characteristic of pigmented BCC (5, 10). This aligns with previous reports describing non-specific, BCC-like dermoscopic patterns in MTB, where features such as blue-gray ovoid nests and arborizing vessels can also be observed (1, 6, 11). In contrast, classic benign trichoblastomas more frequently display a white background and fine, short telangiectasias (2). The overlap in dermoscopic features between these entities necessitates a low threshold for histopathological confirmation. Additionally, in patients with darker skin tones, the dermoscopic features of pigmented basal cell carcinoma often present as ovoid nests and black dots, which were not observed here, further supporting differentiation from typical pigmented BCC. Literature suggests that dermoscopic presentations of adnexal tumors in patients with skin of color may vary, necessitating comprehensive analysis in conjunction with histopathology (12). Ultraviolet dermoscopy may offer greater diagnostic value in such patients. Although not utilized in this case, future studies may consider incorporating it to enhance diagnostic accuracy.
Histopathological examination remains the unequivocal gold standard for differentiating MTB from BCC. Our case exhibited hallmark features of MTB: well-demarcated nests and cords of basaloid cells within the dermis, demonstrating peripheral palisading and set in a fibrous stroma with prominent melanin deposition. Several critical histological distinctions secure the diagnosis: Architectural and Stromal Relationship: MTB typically presents as a well-circumscribed dermal tumor without connection to the epidermis. The most pivotal differentiating feature is the absence of retraction clefts between the tumor cell nests and the surrounding stroma (13), a finding conspicuously present in our case (Figure 3B). In contrast, BCC frequently exhibits epidermal connection and characteristic stromal retraction artifacts. Cytological Features: The basaloid cells in MTB typically lack significant nuclear atypia or mitotic activity, helping distinguish it from more aggressive basal cell carcinomas. Immunohistochemical Profile: While not always necessary, immunohistochemistry can provide decisive evidence. The immunophenotype of MTB often shows patchy or peripheral staining for Bcl-2, CD10 positivity predominantly in the peritumoral stroma, and general negativity for Androgen Receptor (AR) (14, 15). This profile contrasts with BCC, which typically shows diffuse Bcl-2 positivity within tumor islands, CD10 positivity in the tumor cells themselves, and frequent AR positivity (14, 15).
In line with previously reported cases (Table 1), our patient demonstrates typical features of MTB, such as a pigmented nodular presentation on the head and neck, occurrence in middle age, and the clear absence of stromal retraction clefts on histopathology. However, ulceration introduces an unusual clinical characteristic, further highlighting the potential for misdiagnosis. Most reported cases present as pigmented nodules on the head and neck, with colors ranging from light brown to dark blue-black. Ulceration is relatively uncommon; its occurrence here may be related to the lesion’s prolonged duration and local friction. Although MTB has been documented in association with nevus sebaceus (6, 8), the vast majority of cases are sporadic, as in this instance.
As a benign neoplasm with negligible malignant potential, MTB is managed conservatively. Complete surgical excision is the treatment of choice and is curative. Long-term follow-up in our patient and in other reported cases (1, 7) confirms an excellent prognosis with no recurrence, provided the lesion is entirely removed.
Conclusion
This case underscores the critical importance of considering melanotrichoblastoma in the differential diagnosis of pigmented nodular lesions, particularly on the head and neck. The significant clinical and dermoscopic overlap with pigmented basal cell carcinoma can readily lead to misdiagnosis and potential overtreatment. Histopathology is indispensable for definitive diagnosis, with key discriminators being well-defined dermal nests of basaloid cells, abundant stromal pigment, and, most critically, the absence of retraction clefts. Increased awareness of this rare entity among clinicians and pathologists is essential to ensure accurate diagnosis, guide appropriate conservative surgical management, and prevent unnecessary extensive procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ocanha-Xavier JP Xavier-Júnior JCC. Melanotrichoblastoma: sixth case report in the literature. An Bras Dermatol. (2023) 98:871–4. doi: 10.1016/j.abd.2022.07.011, 37393139 PMC 10589488 · doi ↗ · pubmed ↗
- 2Sławińska M Płaszczyńska A Lakomy J Pastuszak K Biernat W Sikorska M . Significance of Dermoscopy in association with clinical features in differentiation of basal cell carcinoma and benign Trichoblastic tumours. Cancers (Basel). (2022) 14:3964. doi: 10.3390/cancers 14163964, 36010957 PMC 9406107 · doi ↗ · pubmed ↗
- 3Stoyanov GS Balabanov I Zhivkova S Popov H. Melanotrichoblastoma: a histopathological case report of a rare pigmented variant of Trichoblastoma. Reports (MDPI). (2025) 8:130. doi: 10.3390/reports 8030130, 40843871 PMC 12372001 · doi ↗ · pubmed ↗
- 4Kanitakis J Brutzkus A Butnaru AC Claudy A. Melanotrichoblastoma: immunohistochemical study of a variant of pigmented trichoblastoma. Am J Dermatopathol. (2002) 24:498–501. doi: 10.1097/00000372-200212000-00008, 12454603 · doi ↗ · pubmed ↗
- 5Kim DW Lee JH Kim I. Giant melanotrichoblastoma. Am J Dermatopathol. (2011) 33:e 37–40. doi: 10.1097/DAD.0b 013e 3181 dfd 120, 20940620 · doi ↗ · pubmed ↗
- 6Hung CT Chiang CP Gao HW Wang WM. Ripple-pattern melanotrichoblastoma arising within nevus sebaceus. Indian J Dermatol Venereol Leprol. (2012) 78:665. doi: 10.4103/0378-6323.100544, 22960841 · doi ↗ · pubmed ↗
- 7Mizuta H Namikawa K Takahashi A Ogata D Muto Y Jinnai S . The first case of a collision tumor of melanotrichoblastoma and seborrheic keratosis. Int J Dermatol. (2021) 60:e 54–6. doi: 10.1111/ijd.15042, 32643154 · doi ↗ · pubmed ↗
- 8Thekho AJ Uikey D Passi S Ramesh V. Melanotrichoblastoma arising on nevus sebaceous: a rare Occurence. Indian J Dermatol. (2025) 70:105–6. doi: 10.4103/ijd.ijd_1197_23, 40162351 PMC 11952701 · doi ↗ · pubmed ↗