A Rare Case of Gastric Aberrant Pancreas Causing Bleeding from a Gastric Ulcer
Tsuyoshi Saito, Hirotaka Miyai, Ryutaro Kato, Ryosuke Niwamoto, Shuhei Ueno, Masahiro Kimura, Shuji Takiguchi

TL;DR
A rare case of gastric aberrant pancreas caused bleeding from a gastric ulcer and was successfully treated with laparoscopic surgery.
Contribution
This case report highlights a rare presentation of gastric aberrant pancreas with bleeding and its successful diagnosis and treatment.
Findings
A 34-year-old man presented with epigastric pain and melena due to a bleeding gastric ulcer caused by aberrant pancreatic tissue.
Endoscopic and histopathological findings confirmed the diagnosis of a Heinrich type I aberrant pancreas.
Laparoscopic partial gastrectomy effectively controlled the bleeding and resolved the condition.
Abstract
An aberrant pancreas is pancreatic tissue lacking anatomical and vascular continuity with the normal pancreas. It typically occurs in the gastrointestinal tract, especially in the stomach, duodenum, and small intestine. Most cases are asymptomatic and discovered incidentally during imaging or surgery. Gastric aberrant pancreas rarely presents with bleeding, making diagnosis and treatment decisions challenging. A 34-year-old man presented with epigastric pain and melena. Endoscopy at a local hospital revealed a submucosal tumor (SMT) with active bleeding at the greater curvature of the stomach. After admission, further imaging and endoscopic ultrasonography showed a 20-mm low-echo mass in the submucosa and muscularis propria with ulceration. Histopathology of a biopsy confirmed aberrant pancreatic tissue. Due to progressive anemia from ulcer bleeding, laparoscopic partial gastrectomy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
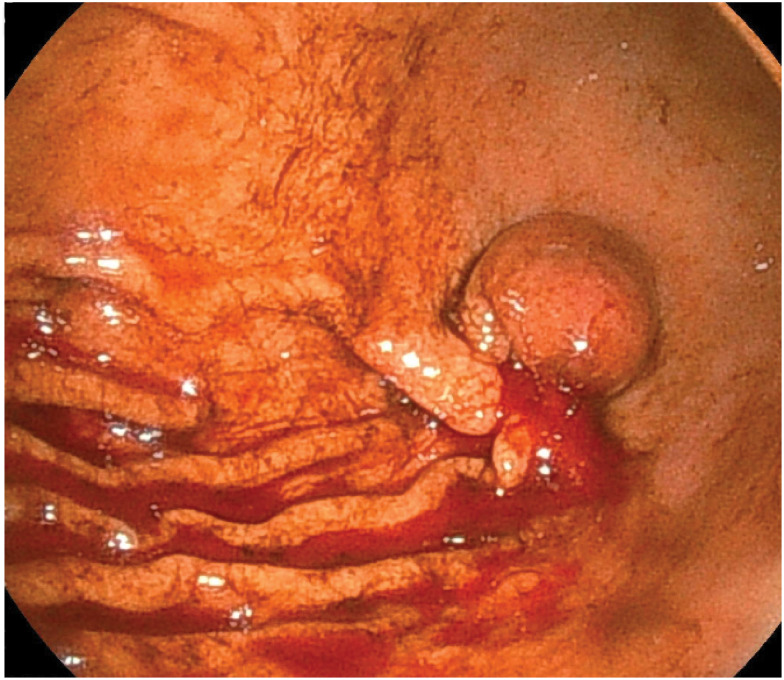 Fig. 1
Fig. 1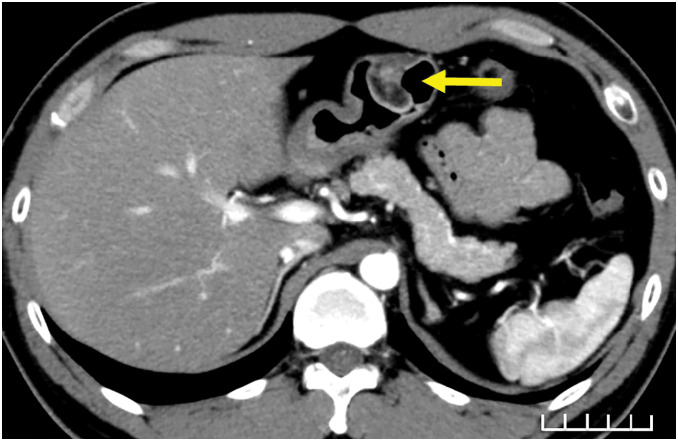 Fig. 2
Fig. 2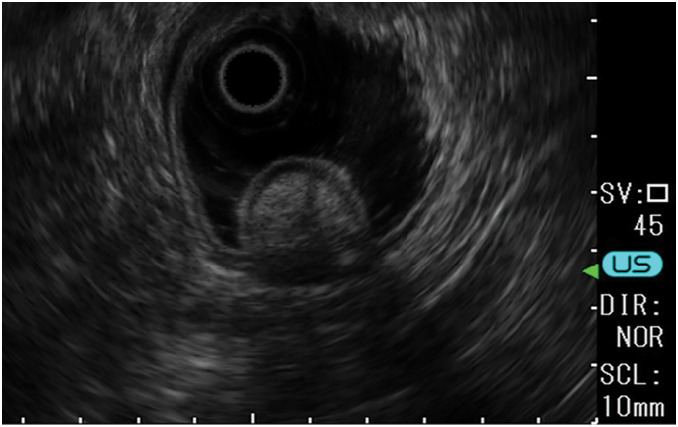 Fig. 3
Fig. 3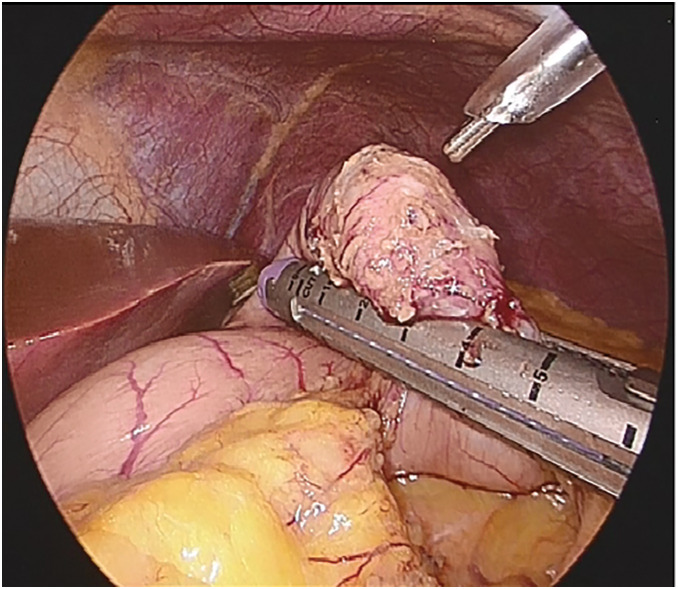 Fig. 4
Fig. 4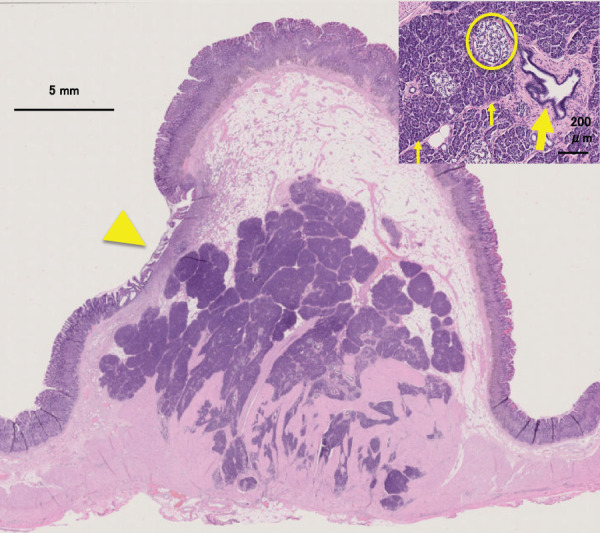 Fig. 5
Fig. 5| No | Author | Year | Age (years) | Sex | Location | Definitive diagnosis by EUS-FNA | Surgical method | Pathological type |
|---|---|---|---|---|---|---|---|---|
| 1 | Hudock | 1956 | 38 | M | Antrum | No | Distal subtotal gastrectomy | Unknown |
| 2 | Takebayashi | 1986 | 35 | M | Antrum | No | Distal gastrectomy | Heinrich type I |
| 3 | Shaked | 1989 | 30 | M | Antrum | No | Distal gastrectomy | Unknown |
| 4 | Yamasaki | 2003 | 47 | M | Lower body | No | Laparoscopic partial gastrectomy | Heinrich type I |
| 5 | Sanada | 2007 | 48 | M | Gastric angle | No | Laparoscopic partial gastrectomy | Heinrich type I |
| 6 | Teke | 2007 | 54 | F | Antrum | No | Distal subtotal gastrectomy | Heinrich type I |
| 7 | Tagata | 2014 | 22 | M | Antrum | No | Partial gastrectomy | Heinrich type I |
| 8 | Kuroda | 2015 | 50 | M | Antrum | No | LECS | Heinrich type III |
| 9 | Yagi | 2017 | 66 | M | Antrum | No | Laparoscopic distal gastrectomy | Heinrich type II |
| 10 | Chamberlain | 2019 | 47 | M | Gastric body | No | Laparoscopic gastric wedge resection | Heinrich type I |
| 11 | Nakajima | 2019 | 67 | M | Upper body | Yes | LECS | Unknown |
| 12 | Matsubara | 2020 | 43 | M | Gastric angle | Yes | Open partial gastrectomy | Heinrich type I |
| 13 | Obana | 2021 | 59 | M | Antrum | Yes | CLEAN-NET | Heinrich type II |
| 14 | LeCompte | 2022 | 37 | M | Unknown | No | Laparoscopic gastric wedge resection | Unknown |
| 15 | Raghavendra | 2025 | 62 | M | Gastric body | No | Robotic local excision | Heinrich type II |
| 16 | Present case | 2025 | 34 | M | Gastric angle | Yes | Laparoscopic partial gastrectomy | Heinrich type I |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Bariatric Surgery and Outcomes · Gastrointestinal Bleeding Diagnosis and Treatment
Abbreviations
EUS-FNA endoscopic ultrasound-guided fine-needle aspiration SMT submucosal tumor
INTRODUCTION
An aberrant pancreas is the pancreatic tissue that lacks anatomical continuity with the pancreas and has blood circulation that is separate from that of the normal pancreas. Its mechanism of development is thought to be by the ectopic migration of part of the dorsal pancreatic rudiment of the duodenum during the fetal period in areas such as the gastrointestinal tract, biliary duct, liver, spleen, or mediastinum. However, the majority of such tissues are located in the stomach, duodenum, or small intestine.^1)^ Patients with an aberrant pancreas are usually asymptomatic; therefore, such an entity is typically discovered incidentally during endoscopy, surgery, or autopsy.
Gastric aberrant pancreas is the 2nd most common type of aberrant pancreas after the duodenum; however, it is rarely detected due to bleeding. Here, we describe a case of laparoscopic local gastrectomy after endoscopic hemostasis of a gastric aberrant pancreas that caused bleeding from a gastric ulcer.
CASE PRESENTATION
A 34-year-old man with no remarkable medical history presented with epigastralgia and melena. At a local hospital, esophagogastroduodenoscopy revealed an SMT with an active bleeding ulcer at the greater curvature of the stomach (Fig. 1). The patient was then referred to our hospital and admitted.
Esophagogastroduodenoscopy findings. A submucosal tumor is found in the greater curvature of the gastric angle, and bleeding is observed from an ulcer at the rise of the oral hilum (esophagogastroduodenoscopy performed at a local hospital).
Laboratory examinations revealed mild anemia but no other significant findings. On esophagogastroduodenoscopy, active bleeding from the peptic ulcer stopped. CT showed a 20-mm nodule with early contrast in the greater curvature of the stomach (Fig. 2). During the follow-up period, endoscopic ultrasonography revealed that the tumor was a low-echo mass located in the submucosa and muscularis propria (3rd and 4th layers). Thickening of the muscularis propria surrounding the mass was also observed. The tumor measured 20 mm, and a peptic ulcer was located at the base of the SMT (Fig. 3). Histopathological examination after biopsy of the peptic ulcer revealed gastric aberrant pancreas.
Axial CT scan of the abdomen. A 20-mm-sized nodule is observed in the greater curvature of the gastric horn, which is contrast-enhanced from the early stage, and a low-absorption area is observed inside the nodule. A mucosal defect is observed, which is suspected to be an ulcer (arrow).
Endoscopic ultrasonography image. The lesion appears as a well-defined hypoechoic mass with the 3rd and 4th layers as the main parts. The lesion is a well-demarcated, hypoechoic mass with 3rd and 4th layers, internal dots of hyperechoic and duct-like echoes, and thickening of the 4th layer.
Laparoscopic partial gastrectomy was performed as it was necessary for gastric SMT resection because of progressive anemia due to bleeding from the peptic ulcer. Observation of the abdominal cavity revealed an SMT in the greater curvature of the stomach, without exposure to the serosal surface. To identify the full extent of the tumor, the greater omentum was divided along the gastric wall to open the omental bursa. The tumor contour was easily recognized by gentle grasping with forceps; therefore, intraoperative endoscopy was not utilized. The tumor was resected using a linear stapler. The specimen was retrieved in a specimen bag, opened intraoperatively, and macroscopically confirmed to have been completely resected before concluding the procedure (Fig. 4). The postoperative course was uneventful, and the patient was discharged on the 5th POD. The SMT measured 25 × 18 × 20 mm and showed severe ulcerative changes. The pathological diagnosis was aberrant pancreas with islets of Langerhans, acinar cells, and excretory ducts (Fig. 5).
Operative findings The tumor was carefully resected with adequate surgical margins by sandwiching the lesion between normal tissues, using 2 firings of a 60-mm linear stapler.
Histopathological findings. The pancreatic lobules and ducts differentiated from the submucosa to the muscularis propria are enlarged, and ulceration is observed in some areas (arrowhead). Fibrosis is observed immediately below the ulcer; however, hemorrhage or disrupted blood vessels are not observed. No malignancies are observed. Abundant adipose tissue is distributed in the submucosal layer above the tumor. Growth of acinar cells (thin arrow), excretory ducts (thick arrow), and islets of Langerhans (circle).Stain: hematoxylin and eosin
DISCUSSION
Aberrant pancreas is found at a site where the pancreatic tissue is anatomically different from the pancreas, and was first reported by Schultz et al. in 1727 (as cited in Elfving and Hästbacka).^2)^ According to a report by De Castro Barbosa et al., of the 471 cases of aberrant pancreas, 27.7% were in the duodenum, 25.5% in the stomach, and 15% in the jejunum.^3)^ The submucosa, muscularis mucosa, and serosa of the stomach account for 73%, 17%, and 10% of cases, respectively, with the submucosa accounting for the largest proportion.^4)^
In pathology, Heinrich’s classification is used for aberrant pancreas. Type I is composed of acinar cells, conduits, and islets of Langerhans; Type II is composed of acinar cells and conduits; and Type III is composed of conduits only.^5)^ In the present case, the aberrant pancreas consisted of acinar cells, conduits, and islets of Langerhans, and was diagnosed as Heinrich type I.
CT and ultrasonography are often used to diagnose aberrant pancreas; however, Zhang et al. reported that only 14% of 184 cases of aberrant pancreas could be diagnosed using ultrasonography before surgery or biopsy.^6)^ However, some reports state that the diagnosis of aberrant pancreas using ultrasound endoscopy with puncture aspiration cytology is useful, with a positive diagnosis rate ranging from 50% to 80%.^7)^ In our case, we performed ultrasonographic endoscopic puncture aspiration cytology and collected the pancreatic adenohypophysis from the gastric submucosa before surgery, allowing us to make a histological diagnosis.
Among aberrant pancreatic lesions, those with symptoms are extremely rare (approximately 6%), and even if symptoms are present, there is no specific relationship with the localization site.^8)^ It has been reported that 20.9% of aberrant pancreatic lesions are symptomatic when limited to the upper gastrointestinal tract.^9)^ Symptomatic aberrant pancreas localized in the upper gastrointestinal tract has been reported to cause abdominal pain in more than half of the cases, as well as gastric discomfort, abdominal distention, vomiting, and bleeding. It has been reported that the percentage of patients with aberrant pancreas and bleeding symptoms is only 8%–9%.^9)^ To identify surgically treated cases of bleeding gastric aberrant pancreas, we performed a comprehensive literature search using the Ichushi-Web database with the Japanese keywords “gastric aberrant pancreas,” “gastric ectopic pancreas,” and “bleeding,” as well as PubMed using the keywords “gastric heterotopic pancreas,” “gastric aberrant pancreas,” “gastric ectopic pancreas,” “bleeding,” and “hemorrhage.” Based on this search, including the present case, a total of 16 cases in patients aged ≥20 years were identified in the literature as far as could be ascertained. The patients ranged in age from 22 to 67 years, with a marked male predominance. Most lesions were located in the gastric antrum or gastric horn (Table 1).^9–23)^ Preoperative definitive diagnosis by EUS-FNA was achieved in only a few recent cases, whereas the majority were diagnosed postoperatively. Surgical procedures varied from partial gastrectomy to distal subtotal gastrectomy, with minimally invasive approaches increasingly adopted in recent years. Histopathologically, Heinrich type I was the most common subtype, followed by types II and III. The present case represents one of the few cases in which a definitive preoperative diagnosis was established by EUS-FNA and successful treatment was achieved with laparoscopic partial gastrectomy. In the present case, the lesion consisted of normal Heinrich type I pancreatic tissue, and ulceration was observed in the overlying gastric mucosa. Several mechanisms have been proposed to explain gastric mucosal injury associated with aberrant pancreas. Alkaline secretion from the pancreatic tissue may stimulate gastrin release, resulting in increased gastric acid and pepsin secretion and subsequent development of mucosal lesions, such as ulcers.^24)^ Alternatively, chronic inflammation arising from aberrant pancreatic tissue may induce edema and congestion in the gastric submucosa, with congestion of fragile submucosal vessels potentially leading to bleeding and diapedesis into the gastric lumen.^25)^ In this case, the bleeding is presumed to have occurred in association with these mechanisms.
Since an aberrant pancreas is usually seen incidentally and is often asymptomatic, the indications for surgery should be carefully considered. However, in 85% of symptomatic aberrant pancreas cases, surgical or endoscopic resection has been reported to eliminate or improve symptoms.^9)^ Therefore, we conclude that surgical treatment is necessary to prevent bleeding. However, even if the patient is asymptomatic, resection may be indicated if gastric cancer, gastric submucosal tumor, or malignant aberrant pancreas cannot be ruled out as differential diseases.^26)^
CONCLUSIONS
Most cases of aberrant pancreas are asymptomatic; however, in the present case, the patient presented with the relatively rare symptom of bleeding, and a preoperative diagnosis of gastric submucosal aberrant pancreas was established using endoscopic examination and fine-needle aspiration cytology. Laparoscopic partial gastrectomy was performed to control the bleeding. Given that gastric aberrant pancreas generally has a lower malignant potential compared with gastrointestinal stromal tumor, preoperative diagnosis is clinically valuable as it allows for appropriate surgical planning. Specifically, it helps to minimize the risk of tumor dissemination associated with gastric content spillage during tumor manipulation and avoids the selection of excessively invasive procedures that would be justified only for malignant lesions. Therefore, accurate preoperative identification of aberrant pancreas can guide the choice of an appropriately tailored, minimally invasive surgical approach while maintaining patient safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Watanabe T, Aoyagi K, Tomioka Y, et al. Endoscopic ultrasonography of duodenal aberrant pancreas: comparison with histology after endoscopic resection. J Med Ultrason (2001) 2015; 42: 277–80.26576585 10.1007/s 10396-014-0592-2 · doi ↗ · pubmed ↗
- 2Elfving G, Hästbacka J. Pancreatic heterotopia and its clinical importance. Acta Chir Scand 1965; 130: 593–602.5865465 · pubmed ↗
- 3De Castro Barbosa JJ, Dockerty MB, Waugh JM. Pancreatic heterotopia; review of the literature and report of 41 authenticated surgical cases, of which 25 were clinically significant. Surg Gynecol Obstet 1946; 82: 527–42.21024692 · pubmed ↗
- 4De Bord JR, Majarakis JD, Nyhus LM. An unusual case of heterotopic pancreas of the stomach. Am J Surg 1981; 141: 269–73.7457747 10.1016/0002-9610(81)90172-0 · doi ↗ · pubmed ↗
- 5Heinrich HV. Ein Beitrag zur Histologie des sogen. akzessorischen Pankreas (in German). Virchows Arch 1909; 198: 392–401.
- 6Zhang Y, Sun X, Gold JS, et al. Heterotopic pancreas: a clinicopathological study of 184 cases from a single high-volume medical center in China. Hum Pathol 2016; 55: 135–42.27195908 10.1016/j.humpath.2016.05.004 · doi ↗ · pubmed ↗
- 7Wiersema MJ, Vilmann P, Giovannini M, et al. Endosonography-guided fine-needle aspiration biopsy: diagnostic accuracy and complication assessment. Gastroenterology 1997; 112: 1087–95.9097990 10.1016/s 0016-5085(97)70164-1 · doi ↗ · pubmed ↗
- 8Dolan RV, Re Mine WH, Dockerty MB. The fate of heterotopic pancreatic tissue. A study of 212 cases. Arch Surg 1974; 109: 762–5.4420439 10.1001/archsurg.1974.01360060032010 · doi ↗ · pubmed ↗