Headache and Papilledema Unmasking an Underlying Myeloproliferative Neoplasm: A Case of Chronic Recanalized Cerebral Venous Sinus Thrombosis
Shamera Hossain, Tameem Tawfiq

TL;DR
A woman with headache and eye swelling was found to have a rare blood disorder after imaging revealed a brain vein clot.
Contribution
This case highlights the diagnostic importance of venous imaging and thrombocyte evaluation in patients with headache and papilledema.
Findings
Chronic, partially recanalized cerebral venous sinus thrombosis was identified in a patient with headache and papilledema.
Thrombocytosis led to the diagnosis of a JAK2-positive myeloproliferative neoplasm.
The case emphasizes the need for venous imaging and hematological evaluation in similar presentations.
Abstract
Cerebral venous sinus thrombosis (CVST) is a potentially life-threatening condition that can present with clinical features mimicking idiopathic intracranial hypertension (IIH), as both may present with headache and bilateral papilledema, leading to diagnostic uncertainty. We report a case of a 50-year-old woman referred for suspected IIH in whom venous neuroimaging revealed chronic, partially recanalized CVST. Thrombocytosis on full blood count, previously uninvestigated, prompted hematological assessment and led to the diagnosis of a JAK2-positive myeloproliferative neoplasm, for which cytoreductive therapy was initiated alongside anticoagulation. This case underscores the importance of performing venous imaging in patients with headache and papilledema, even when features suggest IIH, and highlights that thrombocytosis should prompt evaluation for an underlying myeloproliferative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
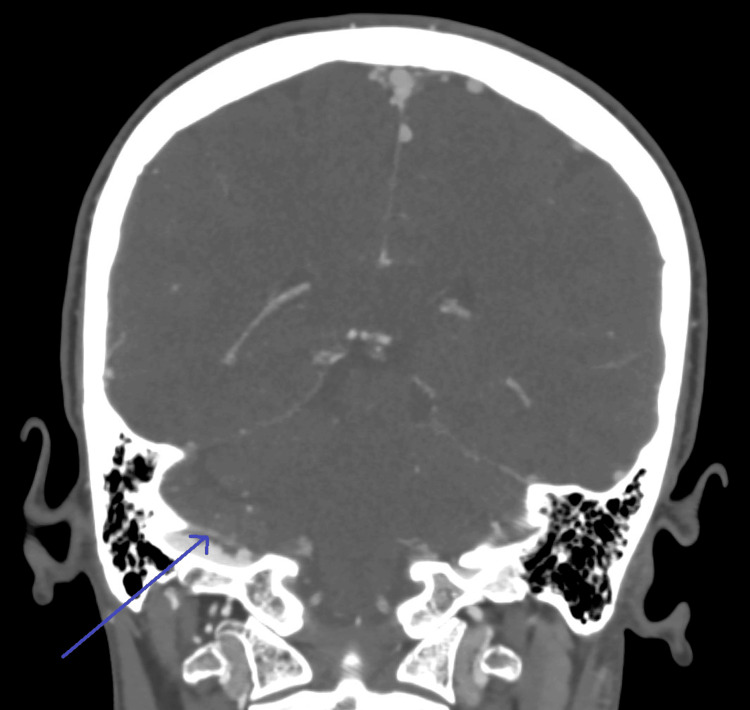 Figure 1
Figure 1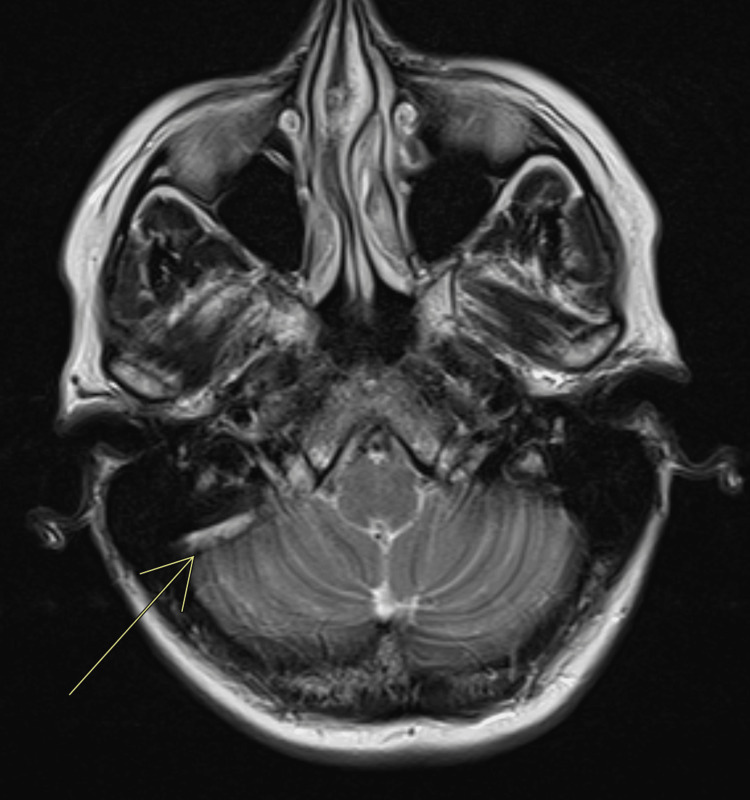 Figure 2
Figure 2| Investigation (units) | Reference range | Patient values | ||
| 26-09-2025 | 13-10-2025 | 3-12-2025 (after treatment) | ||
| Hb (g/L) | 120-160 | 134 | 148 | 133 |
| WBC (× 109/L) | 4-11 | 7.54 | 12.28 | 4.13 |
| PLT (× 109/L) | 150-400 | 796 | 796 | 367 |
| Blood film | — | Thrombocytosis | Thrombocytosis | — |
| Prothrombin time (s) | 9.5-12.5 | 11.2 | 11 | — |
| INR | 0.8-1.2 | 1 | 0.9 | — |
| Serum iron (umol/L) | 10-30 | 16.1 | — | — |
| TIBC (ug/dL) | 240-450 | 61.3 | — | — |
| %TSAT | 20-50% | 26% | — | — |
| Ferritin (ng/mL) | 15-150 | 205 | — | — |
| Sodium (mmol/L) | 135-145 | 138 | 138 | 137 |
| Potassium (mmol/L) | 3.5-4.5 | 4.6 | 4.7 | 4.8 |
| CRP (mg/dl) | <1 | — | 2.6 | — |
| LDH (U/L) | 140-280 | — | 331 | — |
| Uric acid (mg/dL) | 2.5-6.0 | — | 2.6 | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Venous Sinus Thrombosis · Myeloproliferative Neoplasms: Diagnosis and Treatment · Neurosurgical Procedures and Complications
Introduction
Cerebral venous sinus thrombosis (CVST) is a rare but potentially life-threatening cerebrovascular disorder that occurs more commonly in young adults [1]. Thrombosis may develop within the dural venous sinuses or one or more cerebral veins, leading to impaired venous drainage and increased intracranial pressure. Patients may present with nonspecific symptoms such as headache, vomiting, dizziness, seizures, or altered consciousness.
The risk factors for CVST are broadly divided into congenital and acquired causes. Congenital or genetic risk factors include inherited thrombophilias, such as the Factor V Leiden mutation, and deficiencies of protein C or protein S. Acquired risk factors include pregnancy, postpartum period, head trauma, infection, and recent surgery [2].
Thrombocytosis is a well-recognized risk factor for thromboembolic events. It is defined as a platelet count above 450 × 10^9^/L and can be classified as primary or secondary [3]. Primary thrombocytosis results from clonal proliferation of hematopoietic stem cells, as seen in myeloproliferative neoplasms (MPNs) such as essential thrombocythemia. Secondary or reactive thrombocytosis occurs in association with chronic inflammation, infection, malignancy, iron deficiency, or post-splenectomy states. While reactive thrombocytosis resolves with management of the underlying cause, primary thrombocytosis may predispose to both thrombosis and bleeding complications [3].
Idiopathic intracranial hypertension (IIH) is characterized by features of raised intracranial pressure in the absence of hydrocephalus, mass lesion, or abnormal cerebrospinal fluid composition [4]. CVST can mimic IIH, as both conditions share similar clinical manifestations, including headache, visual blurring, tinnitus, and diplopia. However, in cases of chronic or recanalized CVST, symptoms may persist despite partial restoration of venous flow, posing a diagnostic challenge.
We present a case of a middle-aged woman who initially presented with symptoms suggestive of IIH but was ultimately found to have chronic recanalized CVST secondary to JAK2-positive myeloproliferative disease, highlighting the importance of thorough evaluation in patients with raised intracranial pressure.
Case presentation
A 50-year-old woman was referred by the ophthalmology department following the incidental finding of grade 1 bilateral papilledema in the context of a history of headache. On further review, she reported a long-standing history of headaches, including one episode of loss of consciousness approximately five years earlier. This episode had been associated with nausea, and raised platelet counts had been noted since that time. She had initially been diagnosed with cluster headaches in 2021. In 2023, she sustained a head injury, after which her headaches, light-headedness, and tinnitus recurred. She was treated with various analgesics without significant improvement. For the six weeks prior to presentation, she had experienced continuous right-sided headache, particularly in the mornings, with associated periorbital pain that worsened on bending forward. A CT scan of the head was unremarkable. Her general practitioner referred her to the Minor Eye Conditions Service (MECS) and subsequently to ophthalmology, where papilledema was detected.
Ophthalmologic examination showed a normal optical coherence tomography (OCT) macula bilaterally. OCT of the optic disc and retinal nerve fiber layer revealed increased thickness (301 µm in the right eye and 288 µm in the left eye). Bilateral intraocular pressure was elevated (27-29 mmHg). The findings were suggestive of grade 1 papilledema, raising suspicion of IIH, with associated bilateral ocular hypertension.
Similarly, CT venography (Figure 1) showed a linear, eccentric thrombus along the superior wall of the right sigmoid sinus.
CT venogram showing a linear, eccentric thrombus against the superior wall of the right sigmoid sinus.Thin linear filling defects are present in the bilateral sigmoid sinuses, possibly representing chronic sinus thrombosis. The blue arrow indicates the linear eccentric thrombus.
MRI head with contrast (axial T2) at the level of the sigmoid sinus showed a chronic thrombus (Figure 2).
MRI head with contrast (axial T2) at the level of sigmoid sinus showing a chronic thrombus (linear hyperintensity). The white arrow indicates the chronic thrombus.
Routine laboratory investigations revealed persistent thrombocytosis. Further hematological evaluation was undertaken to exclude secondary causes, including iron deficiency, and to assess for primary causes through flow cytometry, paroxysmal nocturnal hemoglobinuria screening, and mutational analysis for JAK2, CALR, and MPL genes. The JAK2 mutation was detected, confirming an underlying myeloproliferative neoplasm (Table 1).
Lumbar puncture demonstrated an opening pressure of 29 mmHg, with normal cerebrospinal fluid composition. On examination, the patient was alert and oriented, with intact cranial nerves and no focal neurological deficits. There were no cerebellar signs, and gait was normal. Fundoscopic examination confirmed grade 1 bilateral papilledema with preserved visual acuity and visual fields.
Based on these findings, she was commenced on low-molecular-weight heparin following discussion with the hematology team and was subsequently started on cytoreductive therapy after the diagnosis of a myeloproliferative neoplasm. She remained under ongoing hematology follow-up, with improvement in headache symptoms, platelet counts, and stable vision.
Discussion
CVST is a rare manifestation of venous thromboembolism (VTE), as the cerebral venous system is an uncommon site of thrombosis. Although its risk factors overlap with those of other thrombotic disorders, the presentation and consequences can be distinct. Anticoagulation remains the mainstay of treatment, aiming to prevent thrombus propagation and promote recanalization. CVST typically affects young adults, with a median age of approximately 35 years, and is more common in women [5]. Reported risk factors include pregnancy, postpartum period, oral contraceptive use, thrombophilia, inflammatory disease, infection, malignancy, dehydration, and head trauma [5]. Due to its unusual location, CVST warrants thorough investigation to identify the underlying precipitating factors and guide long-term management [6]
This patient presented with chronic headache and grade 1 bilateral papilledema, a presentation often initially considered as IIH. The clinical and radiological similarities between chronic or recanalized CVST and IIH can make differentiation challenging. Studies suggest that up to 10% of presumed IIH cases have an underlying CVST, though reports of chronic CVST presenting this way remain rare [7]. Recognition is important, as treatment with anticoagulation differs from standard IIH management. The presence of thrombocytosis on laboratory testing should prompt further evaluation, particularly when thrombosis occurs at an atypical site such as the cerebral venous sinuses.
A study reported that a subset of patients presumed to have IIH were later found to have CVST after detailed neuroimaging, highlighting the risk of misdiagnosis and potential for serious complications such as stroke or death [7]. Identifying the underlying cause of CVST is essential for preventing recurrence. In this patient, persistent thrombocytosis - unexplained by reactive causes - led to the discovery of an underlying JAK2-positive myeloproliferative neoplasm.
This case emphasizes the importance of maintaining a high index of suspicion for CVST in patients presenting with raised intracranial pressure and papilledema. Venous imaging should be performed in all patients before diagnosing IIH. Furthermore, persistent thrombocytosis should prompt evaluation for an underlying myeloproliferative disorder to enable early treatment and reduce the risk of recurrent thrombosis [8].
Conclusions
This case highlights the diagnostic overlap between IIH and chronic recanalized CVST. In patients presenting with features of raised intracranial pressure, including headache and papilledema, neuroimaging with venous studies is essential to exclude CVST, even when symptoms appear chronic or mild. The presence of persistent thrombocytosis should alert clinicians to the possibility of an underlying myeloproliferative neoplasm, particularly when thrombosis occurs at an unusual site. Even partially recanalized CVST can continue to produce symptoms, highlighting the importance of recognizing both the vascular and hematological components early to guide treatment, prevent recurrence, and reduce long-term complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and treatment of cerebral venous thrombosis: a review Front Aging Neurosci Luo Y Tian X Wang X 102018 https://www.frontiersin.org/journals/aging-neuroscience/articles/10.3389/fnagi.2018.00002/full 10.3389/fnagi.2018.00002 PMC 579762029441008 · doi ↗ · pubmed ↗
- 2Epidemiology and risk factors for cerebral venous sinus thrombosis: insights from leading centres in the i-Reg Ve D registry, India Sci Rep Aggarwal S Kumar A Deo V Tabassum H 152025 https://www.nature.com/articles/s 41598-025-07599-x 10.1038/s 41598-025-07599-x PMC 1221661440594714 · doi ↗ · pubmed ↗
- 3Thrombocytosis Hematology Am Soc Hematol Educ Program Skoda RC 1591672009 https://ashpublications.org/hematology/article/2009/1/159/19826/Thrombocytosis 2000819510.1182/asheducation-2009.1.159 · doi ↗ · pubmed ↗
- 4Idiopathic intracranial hypertension: consensus guidelines on management J Neurol Neurosurg Psychiatry Mollan SP Davies B Silver NC 10881100892018 https://jnnp.bmj.com/content/89/10/10882990390510.1136/jnnp-2017-317440 PMC 6166610 · doi ↗ · pubmed ↗
- 5Cerebral venous sinus thrombosis J Thromb Haemost Capecchi M Abbattista M Martinelli I 19181931162018 https://www.sciencedirect.com/science/article/pii/S 15387836220237652992336710.1111/jth.14210 · doi ↗ · pubmed ↗
- 6Cerebral venous sinus thrombosis: clinical features, long-term outcome and recanalization J Clin Neurosci Gazioglu S Eyuboglu I Yildirim A Aydin CO Alioglu Z 248251452017 https://www.sciencedirect.com/science/article/abs/pii/S 09675868173080562880279710.1016/j.jocn.2017.07.028 · doi ↗ · pubmed ↗
- 7Clinical profile of cerebral venous sinus thrombosis and the role of imaging in its diagnosis in patients with presumed idiopathic intracranial hypertension Indian J Ophthalmol Agarwal P Kumar M Arora V 153155582010 https://journals.lww.com/ijo/fulltext/2010/58020/Clinical_profile_of_cerebral_venous_sinus.14.aspx 2019504210.4103/0301-4738.60092 PMC 2854450 · doi ↗ · pubmed ↗
- 8Cerebral venous sinus thrombosis associated with JAK 2 V 617F mutation-related pre-primary myelofibrosis: a case report and literature review BMC Neurol Song J Huang C Jia L 242024 https://link.springer.com/article/10.1186/s 12883-024-03913-810.1186/s 12883-024-03913-8PMC 1147054239395952 · doi ↗ · pubmed ↗