An Unusual Complication at an Unusual Site: Internal Jugular Vein Thrombosis Revealing Celiac Disease
Meriem Mouharir, Zakaria Chahbi, Hassan Qacif, Said Kaddouri, Mohamed Zyani

TL;DR
A 63-year-old woman with unexplained vein clot in her neck was found to have celiac disease, showing it can cause unusual blood clots.
Contribution
Highlights celiac disease as a rare cause of unusual-site venous thrombosis without classical risk factors.
Findings
Celiac disease was confirmed in a patient with internal jugular vein thrombosis and no traditional risk factors.
The patient showed improvement with anticoagulation and a gluten-free diet.
This case suggests celiac disease should be considered in unexplained thrombosis cases.
Abstract
Celiac disease is now recognized as a common disorder that can be diagnosed at any age and affects many organ systems. Its clinical expressions can appear as digestive or extra-digestive; among these, thromboembolic events are the focus of our study. We report a case of a 63-year-old woman who presented with left-sided cervical swelling associated with edema of the left upper limb, with generalized weakness and weight loss. The clinical examination revealed a tender cervical mass in the region of the internal jugular vein. Doppler ultrasound demonstrated thrombosis of the left internal jugular vein extending into the subclavian vein, in the absence of classical risk factors for venous thrombosis. Laboratory investigations showed iron deficiency microcytic anemia and a biological malabsorption profile. Celiac disease was suspected and confirmed by positive serology and duodenal biopsies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
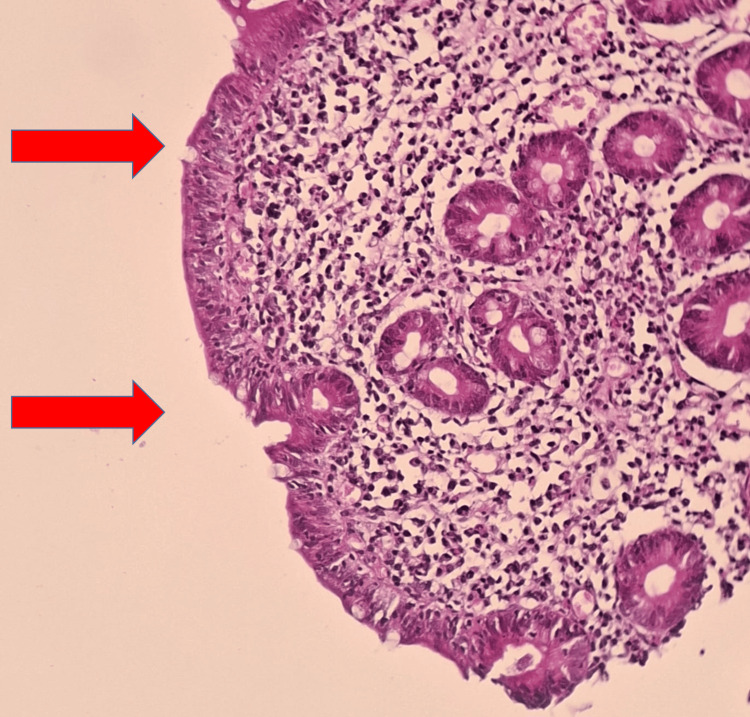 Figure 1
Figure 1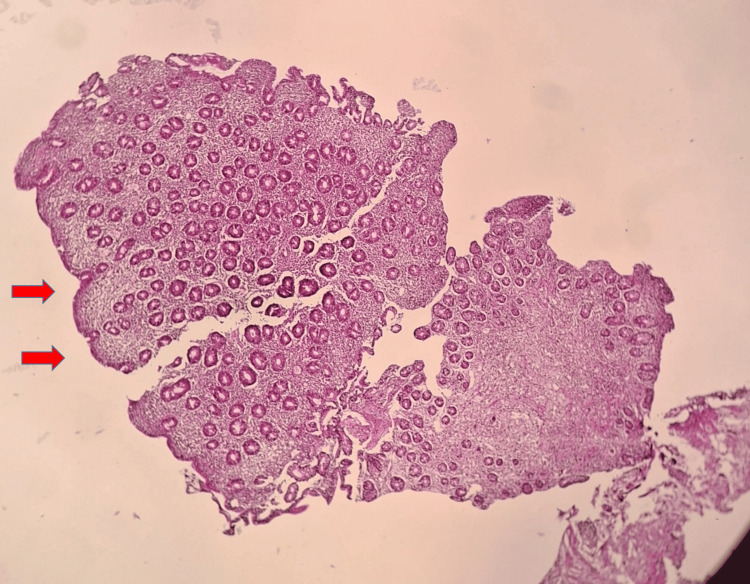 Figure 2
Figure 2| Laboratory tests | Patient laboratory values | Reference values |
| Hemoglobin (g/dL) | 9.1 | 13.0-17.0 |
| Mean corpuscular volume (%) | 61 | 80.0-98.0 |
| Mean corpuscular hemoglobin (pg) | 23 | 26.0-34.0 |
| Neutrophil polynuclear/mm3 | 5160 | 1400-7700 |
| Lymphocyte/mm3 | 800 | 1000-4800 |
| Platelets/mm3 | 249000 | 150000-450000 |
| Hypocalcemia (mmol/L) | 1.58 | 2.12-2.55 |
| Hypoalbuminemia (g/L) | 27 | 35-50 |
| Hypoproteinemia (g/L) | 57 | 62-87 |
| Ferritinemia (ng/mL) | 10 | 30-400 |
| Hypocholesterolemia (g/L) | 1.18 | 1.4-2.0 |
| Vitamin B12 (pg/mL) | <141 | 165-489 |
| Folates (ng/mL) | 2.36 | 4.8-17.0 |
| Anti-transglutaminase IgA antibody (U/mL) | 245 | <4 |
| Anti-endomysial IgG antibody | Positive | <1/40 |
| Protein C (%) | 72 | 70-140 |
| Protein S (%) | 83 | 70-130 |
| Anti-cardiolipin antibodies IgM (U/mL) | 0 | <10 |
| Anti-cardiolipin antibodies IgG (U/mL) | 0 | <10 |
| β2-glycoprotein I antibodies IgM (U/mL) | 0 | <10 |
| β2-glycoprotein I antibodies IgG (U/mL) | 6 | <10 |
| Lupus anti-coagulant | Negative | - |
| Homocysteine (μmol/L) | 60 | 6-17 |
| Anti-nuclear antibodies | Negative | <80 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Celiac Disease Research and Management · Diagnosis and Treatment of Venous Diseases
Introduction
Celiac disease (CD) is a chronic, immune-mediated enteropathy triggered by gluten in genetically predisposed individuals. It can present with a broad spectrum of intestinal manifestations (chronic diarrhea, weight loss, and malabsorption syndrome) and extra-intestinal complications, including oral aphthous stomatitis, articular symptoms, amenorrhea, and thromboembolic events [1-3]. Although an increased risk of venous thromboembolism has been reported in patients with CD, venous thrombosis rarely represents the initial presentation, especially when it occurs at an unusual site [3,4]. We report a case of internal jugular vein thrombosis revealing previously undiagnosed CD in an adult woman.
Case presentation
We present a case of a 63-year-old woman with a medical history of unexplored iron deficiency anemia. She was admitted for left-sided cervical swelling associated with edema of the left upper limb. She was afebrile with generalized weakness and weight loss. She had no identifiable thrombotic risk factors, including no history of recent surgery, no immobilization, no trauma, no central venous catheterization, no use of estrogen-progestin contraceptives, no smoking, or known malignancy. On physical examination, she presented with mucocutaneous pallor and a non-pulsatile, tender left cervical swelling, associated with edema of the ipsilateral upper limb. The vital signs were stable, she was afebrile, and her body mass index was 17 kg/m².
Doppler ultrasound demonstrated thrombosis of the left internal jugular vein extending into the ipsilateral subclavian vein. There were no signs of local neck infection or mass. Laboratory investigations showed iron deficiency microcytic anemia with hemoglobin at 9 g/dL and ferritin at 10 ng/mL, as well as lymphopenia at 800/mm³. The remainder of the malabsorption workup revealed hypocholesterolemia, hypoproteinemia, hypoalbuminemia, hypocalcemia, and vitamin B12 and folate deficiency (Table 1). Renal and liver function tests were normal.
As part of the etiological assessment of this unusual-site venous thrombosis, breast ultrasound and mammography were normal. Screening for inherited and acquired thrombophilia did not reveal any abnormality, except for elevated plasma homocysteine levels consistent with hyperhomocysteinemia (Table 1). An autoimmune workup for anti-phospholipid syndrome, including lupus anticoagulant and anti-cardiolipin/β2-glycoprotein I antibodies, was negative.
In view of the long-standing refractory iron deficiency anemia and biological evidence of malabsorption, celiac disease was suspected. Immunological analysis found positive anti-transglutaminase IgA and anti-endomysial IgG antibodies. Upper gastrointestinal endoscopy showed flattened duodenal folds. Histological examination of duodenal biopsies revealed total villous atrophy and an increased number of intra-epithelial lymphocytes (35%), consistent with celiac disease (Figures 1, 2).
Light microscopy (×100) of duodenal mucosa showing chronic duodenitis with total villous atrophy, crypt hyperplasia, and marked intraepithelial lymphocytosis (arrows).
Light microscopy (×40) of duodenal mucosa showing chronic duodenitis with total villous atrophy, crypt hyperplasia, and marked intraepithelial lymphocytosis (arrows).
The diagnosis of celiac disease, revealed by internal jugular vein thrombosis, was established. The patient was therefore started on anticoagulant therapy with a direct oral anticoagulant (rivaroxaban), with injectable iron and a strict gluten-free diet. She was monitored regularly. Clinical evolution was favorable, with regression of cervical swelling and improvement in general condition. Follow-up laboratory tests showed progressive correction of anemia and improvement of nutritional markers.
Discussion
Internal jugular vein thrombosis (IJVT) is an uncommon but potentially serious manifestation of venous thromboembolism and is most frequently associated with central venous catheterization, head and neck infections (such as Lemierre’s syndrome), trauma, or malignancy [2]. In the absence of these classical local or systemic risk factors, IJVT should prompt a systematic search for underlying prothrombotic conditions, including inherited and acquired thrombophilias, systemic inflammatory diseases, and occult cancer [1,2]. In our patient, none of the usual predisposing factors were identified, and the etiological evaluation ultimately led to the diagnosis of previously unrecognized celiac disease (CD).
CD is now recognized as a common immune-mediated enteropathy that can be diagnosed at any age and may involve multiple organ systems. Beyond its classical digestive presentation, it is increasingly reported to be associated with venous thromboembolism [3]. The association between CD and thrombotic events has been increasingly recognized over the last two decades [3]. More than half of events occur without obvious provoking factors. Thrombosis frequently arises at atypical sites, particularly in the splanchnic circulation and hepatic veins, and may precede the diagnosis of CD in a substantial proportion of patients [3-6]. Venous thromboembolic events appear to be more common than arterial thrombosis in CD; hepatic vein thrombosis (Budd-Chiari syndrome) is among the most frequently reported sites, followed by lower-limb deep vein thrombosis, pulmonary embolism, and cerebral venous thrombosis [3,7,8].
The prothrombotic state in CD is multifactorial [3,9]. Several mechanisms have been proposed as follows: nutritional deficiencies (vitamin K-dependent protein C and protein S deficiency; folate and vitamin B12 deficiency leading to hyperhomocysteinemia), genetic predisposition, such as MTHFR variants, thrombophilic autoantibodies (anti-cardiolipin, anti-β2-glycoprotein I, anti-prothrombin and anti-phosphatidylserine/prothrombin), endothelial dysfunction, and platelet abnormalities [1,4,9,10]. Most patients had at least one acquired prothrombotic abnormality related to malabsorption, including hyperhomocysteinemia and protein C/S deficiency due to vitamin K deficiency, or anti-phospholipid antibodies [4,11].
Hyperhomocysteinemia deserves particular attention. It is a well-recognized prothrombotic factor associated with platelet activation, oxidative stress, endothelial dysfunction, and reduced levels of natural anticoagulants. In CD, hyperhomocysteinemia is typically secondary to malabsorption of folate and vitamin B12, and its prevalence at diagnosis has been reported to be around 20-30% in some adult series [9,10]. In our patient, acquired hyperhomocysteinemia, secondary to vitamin B12 and folate deficiency related to CD-associated malabsorption, was considered a major prothrombotic driver likely contributing to the internal jugular vein thrombosis.
Our observation is noteworthy for the unusual site of thrombosis (internal jugular veins) and for the fact that the thrombotic event revealed previously unrecognized adult CD. Most thrombotic complications reported in CD involve the splanchnic circulation (hepatic, portal, splenomesenteric veins) or cerebral thrombophlebitis; internal jugular vein thrombosis has been much less frequently described [5,7]. In addition, extensive evaluation of our patient did not identify inherited thrombophilia or anti-phospholipid syndrome, making the acquired abnormalities related to malabsorption (iron deficiency anemia, global protein and lipid depletion, hypocalcemia, hyperhomocysteinemia) the most plausible explanation for the prothrombotic state.
Clinicians should maintain a high index of suspicion for CD in patients with unexplained venous thromboembolism, especially at atypical sites, who present with chronic anemia, weight loss, or biological signs of malabsorption, even in the absence of overt gastrointestinal symptoms. Once CD is diagnosed, a systematic search for correctable prothrombotic factors (vitamin K, folate, and vitamin B12 deficiency, hyperhomocysteinemia, protein C/S deficiency, and anti-phospholipid antibodies) is warranted [4,12].
Management of thrombosis in CD relies on standard anti-coagulation combined with strict adherence to a gluten-free diet, which usually leads to mucosal healing, correction of malabsorptive deficiencies, and potentially, reduction of thrombotic risk over time [8,13]. The optimal duration of anti-coagulation in this setting remains uncertain and should be individualized, taking into account the presence of persistent thrombophilic factors, the severity of CD, and the site and extent of thrombosis. Decisions must be made on a case-by-case basis [4,8,13].
In summary, our observation illustrates that CD can present with internal jugular vein thrombosis, adding to the growing spectrum of atypical thrombotic manifestations of this disease. In patients with unexplained venous thrombosis, particularly at unusual sites, screening for CD and its associated acquired thrombophilic abnormalities should be systematically considered. Early diagnosis, institution of a gluten-free diet, correction of nutritional deficiencies, and appropriate anticoagulant therapy are essential to prevent recurrence and long-term complications.
Conclusions
The diagnosis of CD should be considered in cases of unexplained thrombotic manifestations, even in the absence of digestive symptoms. In CD, the risk of thrombotic events can be explained by hyperhomocysteinemia, vitamin B12 and folate deficiency, genetic predisposition (such as MTHFR mutations), and acquired deficiencies of natural anticoagulants, including protein C and protein S. These risk factors may be acquired in the course of the disease and should be systematically investigated and corrected. A gluten-free diet remains the cornerstone of treatment for CD, and correction of nutritional deficiencies through vitamin supplementation, as well as thromboembolic prophylaxis, should be considered on a case-by-case basis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence and etiological profiles of atypical localization venous thrombosis: a descriptive multicenter study. [Article in French]Ann Cardiol Angeiol (Paris) Ramanandafy H Ratsimbazafy SJ Randrianarivony MH 1992027120223571855010.1016/j.ancard.2022.05.001 · doi ↗ · pubmed ↗
- 2Risk factor for deep venous thrombosis in internal medicine: a retrospective study of 318 cases. [Article in French]Ann Cardiol Angeiol (Paris) Salah RB Frikha F Kaddour N 11166320142403526010.1016/j.ancard.2013.06.005 · doi ↗ · pubmed ↗
- 3Thromboembolic complications unveiling celiac disease: a report of two cases Sch J Med Case Rep Chakor F Achdami F Handa A 12981301132025
- 4Adult celiac disease with thrombosis: a case series of seven patients. Role of thrombophilic factors. [Article in French]Rev Med Interne Berthoux E Fabien N Chayvialle JA Ninet J Durieu I 6006043220112143969510.1016/j.revmed.2011.02.025 · doi ↗ · pubmed ↗
- 5Association of Budd-Chiari syndrome and celiac disease. [Article in French]Gastroenterol Clin Biol Afredj N Metatla S Faraoun SA 6216243420102093428910.1016/j.gcb.2010.07.007 · doi ↗ · pubmed ↗
- 6Budd-Chiari syndrome associated with celiac disease. [Article in French]Rev Med Interne Hriz FB Habbassi H Maamouri N 1601623120102004522610.1016/j.revmed.2008.12.016 · doi ↗ · pubmed ↗
- 7Cerebral thrombophlebitis complicating coeliac disease Cureus Zouiter S Bensabbahia D Atrassi M Abkari A 16202410.7759/cureus.66267 PMC 1137599839238677 · doi ↗ · pubmed ↗
- 8Celiac disease and thrombotic events: systematic review of published cases Nutrients Pantic N Pantic I Jevtic D 14202210.3390/nu 14102162 PMC 914442835631302 · doi ↗ · pubmed ↗