Correction of Nasolabial Folds Using Polydioxanone Cog Threads Combined With Botulinum Toxin Type A: A Prospective Comparative Clinical Study
Swapnil U Shinde, Samir Mansuri, Neelam Choudhary, Prashant Pillai, Arun Deepak, Rahul VC Tiwari, Heena Dixit, Seema Gupta

TL;DR
This study shows that combining PDO cog thread lifting with botulinum toxin A improves and prolongs the results of nasolabial fold correction compared to thread lifting alone.
Contribution
The study introduces a combined treatment protocol of PDO cog threads and botulinum toxin A for enhanced and longer-lasting nasolabial fold correction.
Findings
The combination group showed significantly greater wrinkle depth reduction and higher patient satisfaction at 3 and 6 months.
Combined treatment demonstrated sustained superiority over monotherapy, with no serious adverse events.
Mild complications like bruising and swelling were comparable between the two groups.
Abstract
Introduction Nasolabial folds (NLFs) remain one of the most common concerns that drive patients toward minimally invasive facial rejuvenation. This prospective observational study aimed to compare the clinical efficacy and durability of polydioxanone (PDO) cog thread lifting alone and in combination with botulinum toxin type A (BoNT-A) for the correction of moderate NLFs. Materials and methods Thirty-two patients aged 40-65 years with Modified Fitzpatrick Wrinkle Scale (MFWS) grades 2-3 nasolabial folds were divided into two groups. Group A (n = 16) received PDO cog thread lifting alone, using bidirectional barbed threads inserted along the midfacial lifting vectors. Group B (n = 16) underwent an identical thread-lift procedure, followed by targeted BoNT-A injections into the perioral and nasolabial musculature 1h later. Standardized outcomes were assessed at baseline, 15 days, 3…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
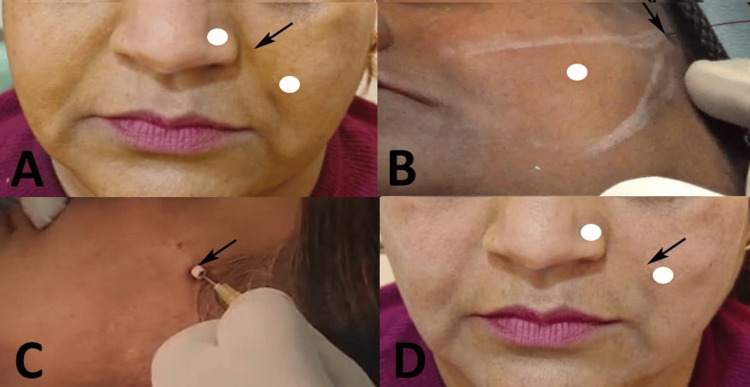 Figure 1
Figure 1 Figure 2
Figure 2| Parameters | Group 1 | Group 2 | Test statistics | p-value | |
| Age | Years (Mean ± SD) | 35.02 ± 5.75 | 32.56 ± 7.34 | 1.05 | 0.299 |
| Sex | Male N (%) | 6 (37.50) | 7 (43.75) | 1.12 | 0.285 |
| Female N (%) | 10 (62.50) | 9 (56.25) | |||
| Parameter | Group | N | Baseline | 15 days | 90 days | 180 days |
| Wrinkle depth (mm) | A | 16 | 2.0 ± 0.3 | 1.2 ± 0.2 | 1.5 ± 0.3 | 1.8 ± 0.3 |
| B | 16 | 2.0 ± 0.3 | 1.0 ± 0.2 | 1.1 ± 0.2 | 1.5 ± 0.3 | |
| MFWS (0–4) | A | 16 | 2.5 ± 0.5 | 1.5 ± 0.5 | 1.8 ± 0.4 | 2.2 ± 0.5 |
| B | 16 | 2.5 ± 0.5 | 1.2 ± 0.4 | 1.3 ± 0.4 | 1.8 ± 0.5 | |
| GAIS (0–4) | A | 16 | 0 | 2.0 ± 0.6 | 1.5 ± 0.5 | 1.0 ± 0.4 |
| B | 16 | 0 | 2.5 ± 0.5 | 2.2 ± 0.5 | 1.5 ± 0.5 | |
| PSS (1–5) | A | 16 | NA | 4.2 ± 0.6 | 3.8 ± 0.7 | 3.0 ± 0.8 |
| B | 16 | 4.5 ± 0.5 | 4.2 ± 0.6 | 3.5 ± 0.7 |
| Measure | Baseline | 15 days | 90 days | 180 days | Overall Group × Time** | |||||
| t-value | p-value | t-value | p-value | t-value | p-value | t value | p-value | F-value | p-value | |
| Wrinkle depth | 0.34 | 0.989 | 2.78 | 0.008* | 4.37 | 0.001* | 2.67 | 0.008* | 21.45 | 0.001* |
| MFWS | 0.68 | 0.992 | 1.83 | 0.070* | 3.53 | 0.001* | 2.26 | 0.031* | 18.78 | 0.001* |
| GAIS | NA | NA | 2.56 | 0.015* | 3.95 | 0.004* | 3.12 | 0.003* | 15.92 | 0.015* |
| PSS | NA | NA | 1.53 | 0.134 | 1.73 | 0.092 | 1.88 | 0.069 | 2.57 | 0.061 |
| Complications | Group A | Group B | Chi-square stats | p-value | ||
| Yes | No | Yes | No | |||
| Bruising | 4 (25%) | 12 (75%) | 6 (37.5%) | 10 (62.5%) | 0.582 | 0.445 |
| Swelling | 4 (25%) | 12 (75%) | 6 (37.5%) | 10 (62.5%) | 0.582 | 0.445 |
| Dimpling | 3 (18.7%) | 13 (81.3) | 3 (18.7%) | 13 (81.3) | 0 | 1 |
| Asymmetry | 3 (18.7%) | 13 (81.3) | 4 (25%) | 12 (75%) | 0.183 | 0.669 |
| Thread extrusion | 2 (12.5%) | 14 (87.5%) | 2 (12.5%) | 14 (87.5%) | 0 | 1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Rejuvenation and Surgery Techniques · Botulinum Toxin and Related Neurological Disorders · Facial Nerve Paralysis Treatment and Research
Introduction
Facial aging is a progressive, multifactorial process characterized by structural changes in the skin, soft tissues, retaining ligaments, and underlying skeletal support. Patients commonly notice early manifestations such as dryness, thinning of the dermis, and dynamic lines that gradually evolve into deeper and more permanent wrinkles [1]. Among these, the nasolabial fold (NLF) is one of the most prominent age-related features, and a major reason individuals seek aesthetic correction. The deepening of the NLF occurs due to descent of the malar fat pad, attenuation of midfacial retaining ligaments, repetitive muscular activity, and age-related remodeling of the midfacial skeleton [2]. Together, these alterations produce a heavier midface and sharper fold contour, prompting patients to pursue minimally invasive facial rejuvenation.
Polydioxanone (PDO) cog thread lifting has emerged as an effective and minimally invasive technique for repositioning sagging tissues by engaging the superficial musculoaponeurotic system (SMAS) [3]. This method provides an immediate mechanical lifting effect followed by neocollagenesis, which improves midfacial support over subsequent months. Botulinum Toxin A (BoNT-A) has been widely used to reduce hyperdynamic muscular contraction by inhibiting acetylcholine release at the neuromuscular junction [4]. Relaxing muscle activity in the perioral and nasolabial regions may enhance the longevity of thread-lift outcomes by minimizing downward muscular pull.
While both techniques have independently demonstrated efficacy, there is limited evidence evaluating whether combining PDO thread lifting with BoNT-A offers superior correction of NLF compared to thread lifting alone [5,6]. Although PDO cog thread lifting effectively corrects the static component of nasolabial folds by repositioning sagging tissues, it does not address the dynamic muscular forces that contribute to fold recurrence. BoNT-A temporarily reduces perioral muscle activity, thereby minimizing antagonistic pull on the lifted tissues during the healing and collagen remodeling phase. When used adjunctively, BoNT-A serves to stabilize and prolong the aesthetic outcome of thread lifting rather than act as a redundant or standalone treatment. Considering that NLF is influenced by both gravitational descent and dynamic muscle activity, a multimodal approach could theoretically provide more stable and refined results.
The aim of the present study was to comparatively evaluate the clinical effectiveness of PDO cog thread lifting alone and in combination with BoNT-A for NLF correction. Specifically, this study sought to assess improvements in wrinkle depth, Modified Fitzpatrick Wrinkle Scale (MFWS) scores, Global Aesthetic Improvement Scale (GAIS) ratings, and patient satisfaction across both treatment groups, while also determining whether the adjunctive use of BoNT-A enhances the stability and overall esthetic outcome of the thread lift. Additionally, this study aimed to monitor and document any procedure-related complications to provide a comprehensive understanding of the safety and therapeutic advantages of this dual-modality approach.
Materials and methods
Study design and setting
This study was conducted as a prospective observational clinical study in which the investigator recorded standardized readings on patients undergoing nasolabial fold correction procedures in the Department of Oral and Maxillofacial Surgery, RKDF Dental College and Research Centre, Bhopal, India. This study was conducted over a period of 12 months (Aug 2024 - Aug 2025). No part of the clinical procedure was modified for research purposes; the investigator only observed and documented the pre- and post-treatment findings. Ethical approval was obtained from the Institutional Ethics Committee (RKDF/DC/PG/2024/143), and written informed consent was obtained from all participants before enrolment, including consent for clinical photography and scoring.
Eligibility criteria
Patients aged 40-65 years with visible NLFs graded between 2 and 3 on the MFWS [7] were considered eligible. Only medically stable individuals willing to undergo the procedure and attend all scheduled follow-up visits were included. Patients with unrealistic esthetic expectations; local skin infections; known hypersensitivity to lidocaine, epinephrine, PDO material, or BoNT-A; and those medically unfit for minor esthetic interventions were excluded. Individuals outside the required age group or those with NLF severity outside the MFWS 2-3 range were not included.
The required sample size was calculated using the G*Power software (version 3.1.9.2; Heinrich Heine University, Düsseldorf, Germany). The sample size was determined by using wrinkle depth reduction as the primary outcome measure. Based on an expected mean difference of 0.4 mm, a standard deviation of 0.35 mm [7], an alpha of 0.05, and 80% statistical power, approximately 12 patients were required per group. Accounting for an anticipated 20% dropout rate, the final target enrolment was set at 16 participants per group, or 32 subjects for the study. Eligible patients were consecutively enrolled during the study period and assigned to one of the two treatment groups based on the treatment protocol selected after routine clinical consultation. Patients who consented to undergo PDO cog thread lifting alone were allocated to Group A, while those who consented to receive PDO cog thread lifting followed by adjunctive botulinum toxin type A injections were allocated to Group B. Each group comprised 16 patients.
Clinical assessment tools
The baseline evaluation included measurement of wrinkle depth, MFWS score [8], and GAIS grading [9]. MFWS is a validated wrinkle-severity grading tool that classifies NLFs into five ordered categories based on depth, visibility, and contour changes. Scores range from Grade 0 (no wrinkles) to Grade 4 (deep, severe wrinkles with pronounced fold shadows), allowing consistent and reproducible assessment of wrinkle severity across clinical settings. The scale is simple, clinically intuitive, and free to use for research, without licensing or permission requirements.
Similarly, GAIS is a widely used physician- and patient-reported outcome measure that evaluates overall aesthetic enhancement after treatment. The GAIS uses a 5-point ordinal scoring system ranging from “Very Much Improved” to “Worse,” reflecting the degree of visible improvement relative to the baseline. A score of “Very Much Improved” indicates optimal cosmetic change, whereas “No Change” or “Worse” reflects minimal or negative aesthetic response. GAIS is also free for academic use and requires no special permission.
Pre-procedure preparation
Each patient underwent standardized skin preparation, which included cleansing with a 2% chlorhexidine solution (Hibiscrub®, Mölnlycke Health Care, Gothenburg, Sweden). Topical anesthesia was applied (EMLA® cream, AstraZeneca PLC, Cambridge, UK) for approximately 45-60 min. After cream removal, local anesthesia was administered using 2% lidocaine with epinephrine 1:200,000 (Aspen Pharmacare Holdings Ltd., Durban, South Africa). Prior to the procedure, skin markings were performed with the patient in an upright position to counteract gravitational tissue displacement. Standardized lifting vectors were drawn from the temporal entry point toward the nasolabial fold, following the direction of midfacial soft-tissue descent. These markings guided thread trajectory, ensured symmetry, and helped achieve consistent and reproducible tissue elevation across patients.
Procedure in Group A: PDO cog thread lift alone
In Group A, correction of the NLF was performed exclusively using PDO barbed threads (MINT™ PDO threads; HansBiomed Co. Ltd., Seoul, South Korea). After adequate anesthesia, a small stab incision was made in the temporal hollow, approximately 1 cm lateral to the lateral orbital rim, using an 18-gauge needle. Through this entry site, two precannulated PDO cog threads were introduced into the subcutaneous plane along pre-marked lifting vectors. The cannula was advanced carefully until the barbs were engaged in the deep medial fat pad and SMAS. Once optimal placement was confirmed, gentle superior traction was applied to elevate the sagging midfacial tissue and reduce the depth of the nasolabial fold. The cannula was then withdrawn, excess thread was trimmed, and the entry point was manually compressed to minimize dimpling. The procedure was repeated on the contralateral side using the same technique (Figure 1).
Representative patient from Group A: PDO cog thread lifting monotherapy (A) Baseline frontal view showing bilateral moderate nasolabial folds (MFWS Grade 3), (B) Intraoperative view showing temporal entry point for insertion of bidirectional barbed PDO cog threads, (C) Immediate post-procedure photograph during administration of supplemental local anesthetic (2% lidocaine with 1:200,000 epinephrine) along the thread tracts for enhanced post-operative comfort and hemostasis, (D) 6-month follow-up frontal view demonstrating good initial correction with partial recurrence of the nasolabial folds.Original images of the patient. Used with the patient's permission.PDO: polydioxanone; MFWS: Modified Fitzpatrick Wrinkle Scale
Procedure in Group B: PDO cog thread lift combined with BoNT-A
Group B patients underwent the same standardized thread-lift procedure as described for Group A, using identical thread types, insertion vectors, and lifting maneuvers. Approximately one hour after thread placement, BoNT-A injections were administered (BOTOX®; Allergan Aesthetics, AbbVie Inc., North Chicago, IL, USA). The toxin was reconstituted with 10 mL of preservative-free normal saline and 3 mL of lidocaine with epinephrine, providing a total volume of 13 mL. Injections were delivered at a dose of approximately 1.5 U per cm of thread length, placed 3-4 mm lateral to the thread vector to target the underlying muscles that contribute to NLF formation. Additional focused injections were delivered into the levator labii superioris alaeque nasi muscle using a palpation-guided approach to reduce the vertical pull on the fold. A 31-gauge insulin syringe (BD, Franklin Lakes, New Jersey, USA) was used for precise dosing and to minimize discomfort (Figure 2).
Representative patient from Group B: PDO cog thread lifting combined with botulinum toxin type A (A) Baseline frontal view showing bilateral moderate nasolabial folds (MFWS Grade 3), (B) Intraoperative view showing temporal entry point for insertion of PDO cog threads and botulinum toxin type A injections, (C) 6-month follow-up frontal view demonstrating superior and sustained softening of the nasolabial folds with excellent long-term esthetic outcome.Original images of the patient. Used with the patient's permission.PDO: polydioxanone; MFWS: Modified Fitzpatrick Wrinkle Scale
Follow-up and outcome recording
All clinical outcomes were recorded at 15 days, 3 months, and 6 months, using standardized photography and consistent scoring protocols. Wrinkle depth was assessed through digital measurements, MFWS scores were assigned by clinical grading, and GAIS scores were documented according to recognized descriptors. Any complications, such as bruising, swelling, dimpling, asymmetry, or thread extrusion, were documented systematically and managed according to standard clinical protocols. Post-procedural complications were monitored at all scheduled follow-up visits (15 days, 3 months, and 6 months). For analytical purposes, complications were analyzed cumulatively over the entire 6-month follow-up period. Each complication was recorded once per patient, irrespective of the time point at which it first appeared. Patients experiencing the same complication at multiple follow-up visits were counted only once for that specific complication. This approach was adopted to reflect the overall safety profile of the interventions rather than time-specific event frequency.
Patient satisfaction was assessed using a 5-point Patient Satisfaction Scale (PSS) [10], a simple Likert-type tool widely used in aesthetic outcome research to quantify a patient’s subjective improvement after treatment. The scale ranges from 1 (very dissatisfied) to 5 (very satisfied), providing a direct measure of postprocedural satisfaction. PSS is freely available for academic use and does not require licensing or special permission for incorporation into clinical research.
Statistical analysis
Statistical analysis was conducted using the Statistical Package for Social Sciences (SPSS) version 23.0 (IBM Corp., Armonk, New York, USA). Continuous and ordinal data that followed a normal distribution, as confirmed by the Shapiro-Wilk test, were summarized as the mean ± standard deviation. Categorical complication data were presented as frequencies and percentages. Intergroup comparisons at each time point were performed using independent-sample t-tests. Two-way analysis of variance (ANOVA) was employed to evaluate the effects of group and time simultaneously. Statistical significance was defined as p < 0.05, and p < 0.01 indicated highly significant results.
Results
The demographic variables of the two groups were comparable at baseline. There was no statistically significant difference in age between the groups (Group 1: 35.02 ± 5.75 years vs. Group 2: 32.56 ± 7.34 years). The sex distribution was also similar, with no significant difference in the proportion of males or females between the groups (p = 0.285), as given in Table 1.
The results demonstrated that both treatment groups showed improvement in NLF appearance; however, Group B achieved superior and more sustained outcomes. At all post-treatment intervals (15, 90, and 180 days), Group B exhibited lower wrinkle depth, better MFWS scores, higher clinician-rated esthetic improvement (GAIS), and greater patient satisfaction (PSS) than Group A. The most notable differences were observed at the 90- and 180-day marks, suggesting that the combined protocol provided longer-lasting effects (Table 2).
The results demonstrated a significant Group × Time interaction effect (Two-way ANOVA, p<0.001) for all outcomes except PSS, indicating that the treatment trajectories differed meaningfully between the groups. Independent t-tests revealed that, compared to Group A, Group B achieved significantly greater improvement in wrinkle depth at 15, 90, and 180 days (all p < 0.01). Similarly, patient and physician assessments (MFWS, GAIS) showed significantly better outcomes in Group B from 90 days onward (p < 0.05), with GAIS showing earlier significance at 15 days. However, no significant inter-group difference was found for PSS at any time point. The inference is that the intervention in Group B produced a clinically superior and sustained reduction in wrinkle depth and associated aesthetic scales compared to Group A, although this objective and observer-rated superiority did not translate into a statistically significant difference in the patients' own subjective satisfaction over the 180-day period (Table 3).
**Table 3: Comparison of outcome parameters between groups at different time points using independent samples t-test and two-way analysis of variance (ANOVA).*p < 0.05 considered statistically significant, p < 0.01 indicates highly significant results; Two-way ANOVA used to assess overall Group × Time interaction effect. The independent t-test was used for between-group comparison at each time point.MFWS: Modified Fitzpatrick Wrinkle Scale scores [8]; GAIS: Global Aesthetic Improvement Scale [9]; PSS: Patient Satisfaction Scale [10]; NA: parameters not measured at baseline (GAIS, PSS).
Complication rates, including bruising, swelling, and dimpling, were slightly higher in Group B; however, they were generally transient and manageable. These findings indicate that adjunctive BoNT-A enhanced and prolonged the efficacy of thread lifting for nasolabial folds, with a favorable risk-benefit profile. The analysis of treatment-related complications revealed comparable safety profiles between the groups. Although Group B exhibited numerically higher rates of bruising and swelling, these differences were not statistically significant (p = 0.445). Similarly, the incidences of dimpling, asymmetry, and thread extrusion showed no significant intergroup variation. All chi-squared statistics were low, with p-values exceeding 0.05, confirming that none of the observed differences in complication frequencies reached statistical significance (Table 4).
Discussion
The findings of this prospective observational study highlight the enhanced clinical efficacy of combining PDO cog thread lifting with BoNT-A for NLF correction compared to PDO thread lifting alone. Both treatment groups demonstrated improvements in NLF appearance, but Group B (combination therapy) exhibited significantly greater reductions in wrinkle depth, lower MFWS scores, higher GAIS ratings, and superior patient satisfaction as measured by the PSS at 3 and 6 months post-treatment. These differences were most pronounced at later follow-up points, suggesting that adjunctive BoNT-A contributes to the prolonged stability of esthetic outcomes. Two-way ANOVA further confirmed the findings, underscoring divergent treatment trajectories favoring the multimodal approach.
These results can be attributed to the complementary mechanisms of these two modalities. PDO threads provide immediate mechanical elevation of sagging midfacial tissues by engaging the SMAS and malar fat pad, followed by neocollagenesis, which enhances tissue support over time [3]. However, gravitational descent alone does not fully account for NLF deepening; repetitive contractions of muscles, such as the levator labii superioris alaeque nasi and zygomaticus, contribute to dynamic wrinkling and downward pull, potentially undermining thread longevity [2,11]. BoNT-A inhibits acetylcholine release at the neuromuscular junction, thereby relaxing hyperdynamic musculature and reducing tension on lifted tissues [4]. This synergy likely explains the sustained improvements observed in Group B, as BoNT-A minimizes forces that could otherwise accelerate the fold recurrence.
Our observations align with prior research, emphasizing the benefits of combining thread lifting with neuromodulators for facial rejuvenation. For example, Ziade et al. [12] evaluated a triple combination of barbed threads, hyaluronic acid fillers, and BoNT-A for nonsurgical rhinoplasty in 30 patients and reported superior facial assessment and cosmetic enhancement quality of life questionnaire (FACE-Q) satisfaction scores and minimal efficacy decay over 1 year in the full combination group compared with threads plus BoNT-A alone. Although their focus was on nasal reshaping, the enhanced longevity from BoNT-A muscle relaxation mirrors our findings for NLFs, where dynamic components play an analogous role.
Similarly, Wanitphakdeedecha et al. [4] demonstrated that intradermal BoNT-A injections alone achieved significant facial lifting in 17 patients (77.3%). Their results support BoNT-A's standalone efficacy against dynamic aging; however, our study extends this by showing additive benefits when paired with threads, yielding more comprehensive midface repositioning. Similar to our findings, Binder [13] demonstrated the long-term effects of BoNT-A for facial lines, with no adverse effects even if given regularly for 13 years.
In contrast, studies on monotherapy provided a context for our comparative design. Germani et al. [14] conducted a randomized trial of PDO threads for facial lifting in 22 patients and found no significant difference in outcomes between six and 12 threads per face, with initial volumetric improvements diminishing by 60 days. This echoes the trajectory in Group A, where early gains in wrinkle depth and MFWS waned by six months, highlighting the limitations of threads alone in countering ongoing muscular activity.
The preliminary cranial tissue displacement observed over the initial period, commonly referred to as the lifting effect, is contingent on the primary tension engendered by the traction provided by the PDO threads. Thereafter, a caudal counter-displacement force, influenced by gravitational pull, tissue weight, and facial expressions, became increasingly evident. This caudal counter-displacement phenomenon has the potential to counteract the initial lifting effect, resulting in an outcome that is contrary to the intended effect because PDO threads lack anchorage to a rigid structural entity [3,15].
Regarding safety, complication rates were comparable between the groups, with transient bruising, swelling, and dimpling predominating but resolving without intervention. Group B showed numerically higher incidences, likely due to additional injections, but the differences were not statistically significant, which is consistent with the literature on minimally invasive procedures. Ziade et al. [12] reported higher adverse effect scores in thread-involved groups, attributing them to invasiveness, yet all resolved within a week. Similarly, Germani et al. [14] noted only minor self-limiting pain. These parallels confirm the favorable risk-benefit profile of our combination protocol, with no severe events such as thread extrusion or infection observed.
The Global Aesthetics Consensus Group proposed that the mid and lower regions of the facial structure exhibit the greatest responsiveness to a synergistic intervention involving both dermal fillers and botulinum toxin. It has been observed that a synergistic effect can be attained through meticulously orchestrated individualized treatment protocols. This methodology is not exclusively pertinent to the lower facial area; however, it is also applicable to the upper facial regions, as well as certain segments of the midface. The advocated strategy is personalization, meticulously designed to address the specific requirements of the patient [16].
Clinical implications
The superior outcomes of PDO threads plus BoNT-A suggest that this approach is the preferred first-line option for patients aged 40-65 years with moderate NLFs, particularly for those seeking minimally invasive rejuvenation with enhanced longevity. By integrating mechanical lift with muscle relaxation, clinicians can achieve more natural and stable results, potentially reducing the need for frequent touchups and improving cost-effectiveness. This is especially relevant in oral and maxillofacial surgery settings, where precise knowledge of midfacial anatomy can optimize vector planning and injection sites. Patient counseling should emphasize the additive benefits of screening for BoNT-A hypersensitivity to ensure safety.
Limitations
This study had several limitations. The observational design lacked randomization and introduced potential selection bias despite baseline similarity. The sample size was modest, powered for wrinkle depth, but possibly underpowered for rare complications. As this was a single-center study in India, generalizability to diverse populations may be limited by ethnic variations in facial aging. Follow-up was restricted to 6 months; longer-term assessment (12-24 months) is needed to evaluate durability during ongoing collagen remodeling. Finally, subjective scales are prone to assessor and patient bias, although standardized photography mitigates this bias.
Conclusions
This study demonstrated that combining PDO cog thread lifting with BoNT-A yielded superior, longer-lasting correction of NLFs than thread lifting alone. The adjunctive use of BoNT-A effectively reduced the dynamic muscular pull and enhanced the stability and esthetic outcome of the mechanical lift. Both approaches proved safe with only mild transient complications. The synergistic dual-modality protocol addresses the multifactorial nature of nasolabial fold deepening more comprehensively than monotherapy does. It represents a reliable, minimally invasive option offering enhanced durability and natural results, making it a valuable addition to contemporary esthetic practices for midface rejuvenation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The facial aging process from the "inside out"Aesthet Surg J Swift A Liew S Weinkle S Garcia JK Silberberg MB 110711194120213332549710.1093/asj/sjaa 339PMC 8438644 · doi ↗ · pubmed ↗
- 2Quantitative assessment of nasolabial fold characteristics across age groups Aesthet Surg J Open Forum Quan Y Zhang T Liu L Han B Cao Z Shen Y 07202510.1093/asjof/ojaf 075PMC 1232248540765990 · doi ↗ · pubmed ↗
- 3SMAS repositioning technique utilizing cog thread: anatomical perspectives Skin Res Technol Hong GW Kim SB Park SY Wan J Yi KH 030202410.1111/srt.13650 PMC 1094559238497380 · doi ↗ · pubmed ↗
- 4Intradermal injection of incobotulinumtoxin A for face lifting Dermatol Ther Wanitphakdeedecha R Nokdhes YN Patthamalai P 033202010.1111/dth.1394432614987 · doi ↗ · pubmed ↗
- 5Synergistic facial rejuvenation with PDO threads and Botulinum Toxin A for aging skin Case Reports Plast Surg Hand Surg Aliyeva A 25465281220254080002610.1080/23320885.2025.2546528 PMC 12340935 · doi ↗ · pubmed ↗
- 6Using PDO threads: a scarcely studied rejuvenation technique. Case report and systematic review J Cosmet Dermatol Contreras C Ariza-Donado A Ariza-Fontalvo A 215821652220233702145810.1111/jocd.15709 · doi ↗ · pubmed ↗
- 7Outcomes of polydioxanone knotless thread lifting for facial rejuvenation Dermatol Surg Suh DH Jang HW Lee SJ Lee WS Ryu HJ 7207254120152599361110.1097/DSS.0000000000000368 · doi ↗ · pubmed ↗
- 8The modified Fitzpatrick Wrinkle Scale: a clinical validated measurement tool for nasolabial wrinkle severity assessment Dermatol Surg Shoshani D Markovitz E Monstrey SJ Narins DJ 09134 Suppl 1200810.1111/j.1524-4725.2008.34248.x 18547187 · doi ↗ · pubmed ↗