Assessment of sealing ability, antibacterial effect and marginal adaptation of bioactive materials in pulpotomized primary molars: an in-vitro study
Reham Ahmed El-Nemr, Wedad M. Nageeb, Noha El-Sayed Fathi Abdou

TL;DR
This study compares three bioactive materials for their ability to seal, prevent bacteria, and fit well in treated baby molars.
Contribution
The study provides a direct comparison of MTA, Biodentine, and NeoPUTTY in terms of antibacterial effect, sealing, and marginal adaptation in primary molars.
Findings
MTA showed higher bacterial leakage compared to Biodentine and NeoPUTTY.
Biodentine and NeoPUTTY demonstrated superior antibacterial activity and marginal adaptation.
Microgap width was significantly larger for MTA compared to NeoPUTTY but not Biodentine.
Abstract
The success of pulpotomy depends on the restorative material’s ability to provide an effective seal, preventing bacterial penetration and growth within the root canal. This study was performed to compare three different types of calcium silicate-based cement in pulpotomized extracted primary molars considering antibacterial effect, sealing ability and marginal adaptation. Recently extracted second primary molars were randomly categorized into three experimental groups (n = 10 each). Pulpotomy cavity preparations were made and pulp dressing materials were placed as follows: MTA (group I), Biodentine (group II) and NeoPUTTY (group III). All teeth were contaminated with Enterococcus faecalis and incubated for 21 days. One half of each molar was stained with the LIVE/DEAD BacLight Bacterial Viability Kit and evaluated using Confocal Laser Scanning Microscopy (CLSM) for observing live and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
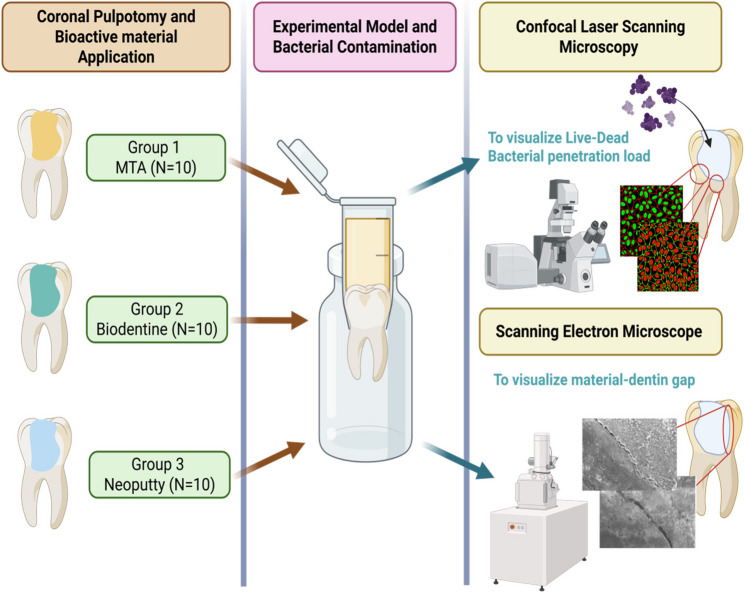 Figure 1
Figure 1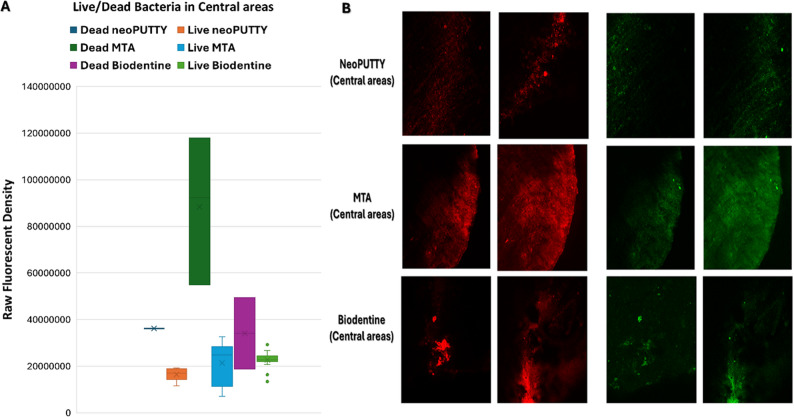 Figure 2
Figure 2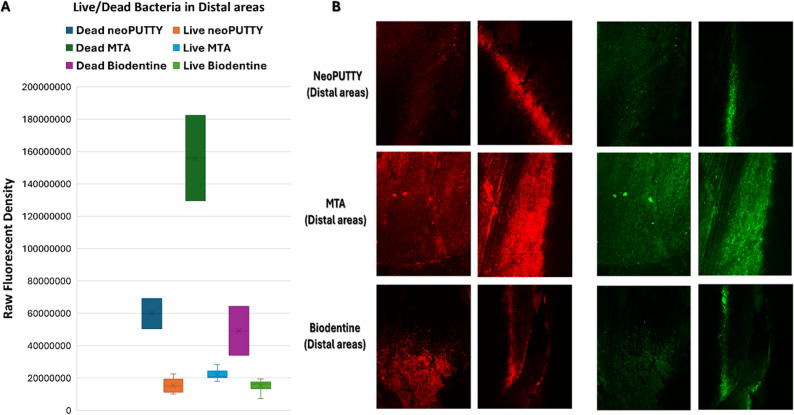 Figure 3
Figure 3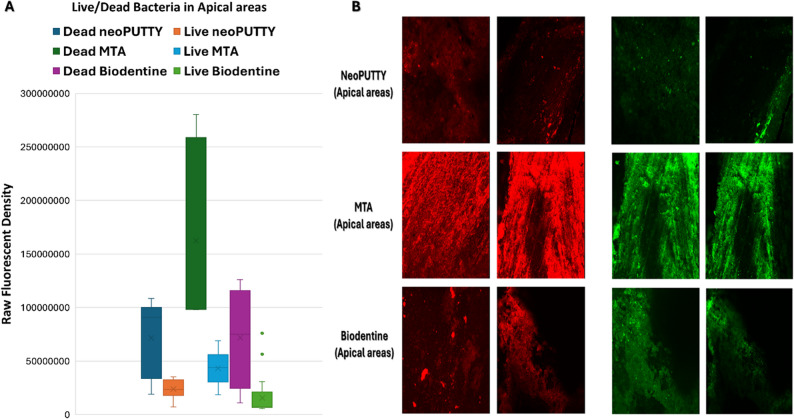 Figure 4
Figure 4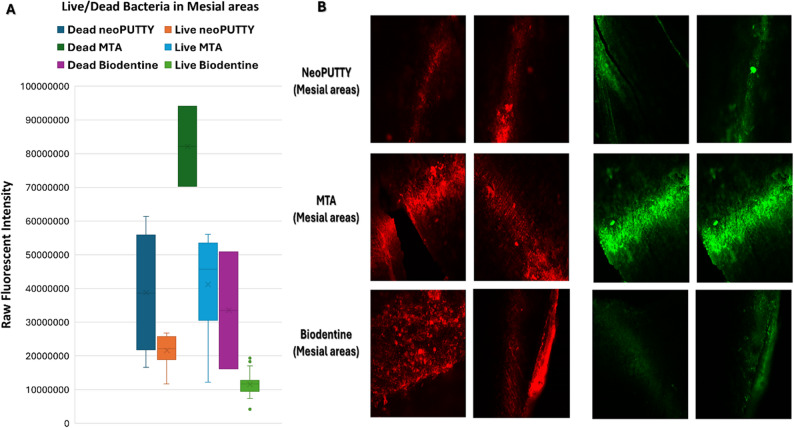 Figure 5
Figure 5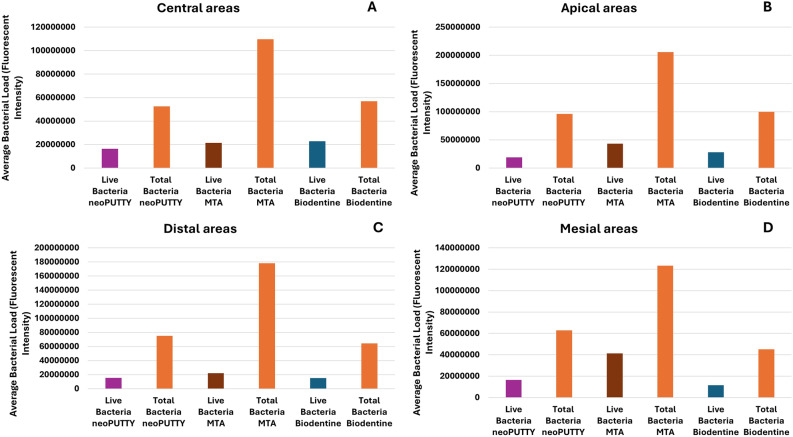 Figure 6
Figure 6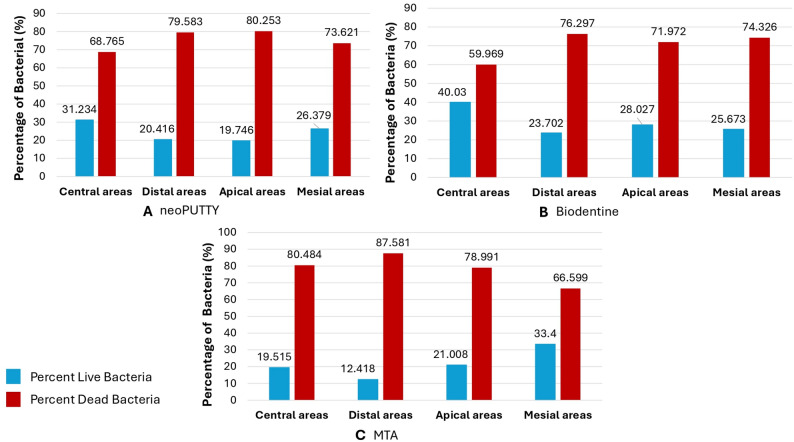 Figure 7
Figure 7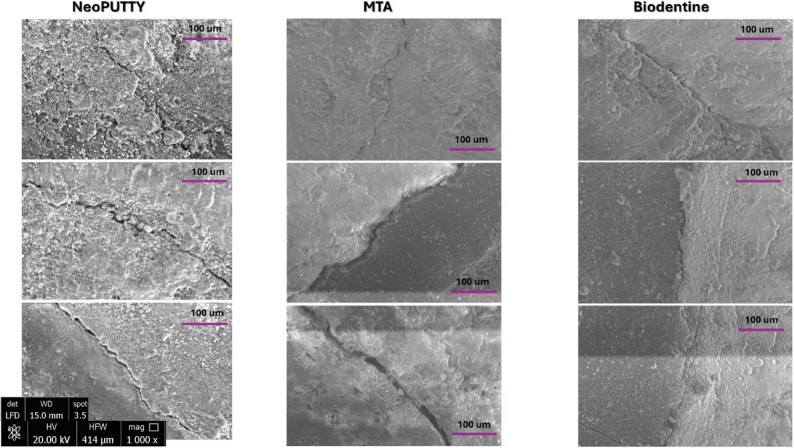 Figure 8
Figure 8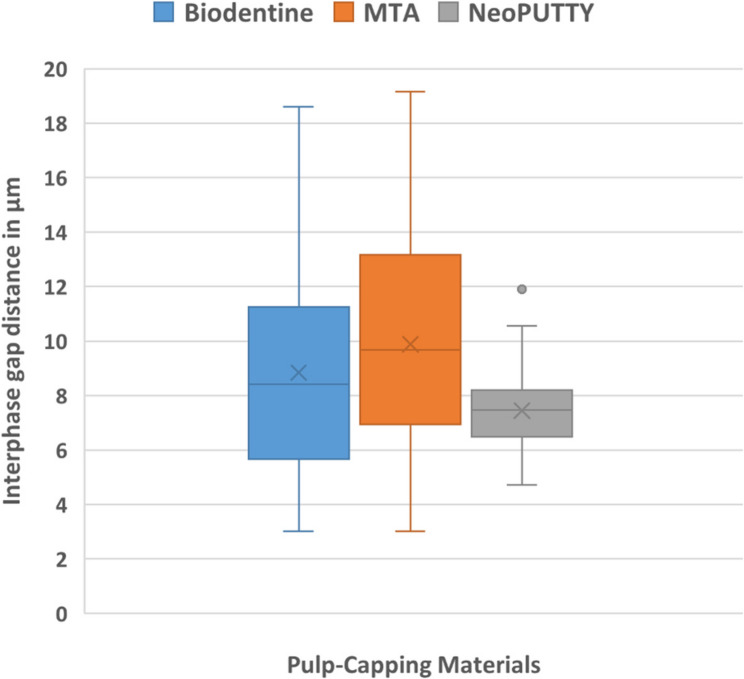 Figure 9
Figure 9- —Suez Canal University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Dental materials and restorations · Dental Erosion and Treatment
Introduction
The premature loss of primary teeth may result in adverse consequences, including compromised masticatory function, loss of space, malocclusion, unusual tongue habits, speech impediments, psychological issues and consequently affecting the growth and development of the child. Therefore retention of primary teeth until natural exfoliation is crucial [1, 2].
Pulpotomy is the preferred treatment for severely carious primary teeth or following iatrogenic pulp exposure in asymptomatic primary teeth or those with reversible pulpitis, which would otherwise necessitate extraction. The procedure aims to preserve the vitality of the radicular pulp after surgical removal of the infected coronal pulp by placing a pulpotomy base material (PBM) followed by permanent restoration [3, 4]. A major cause of failure is coronal microleakage, which allows bacterial penetration. For successful outcomes, PBMs should have good bonding with the pulp dentin complex and the upper final restoration, ensuring an effective seal to prevent postoperative sensitivity, secondary caries, and bacterial proliferation [5, 6].
Tricalcium silicate-based cement has been used in pulpotomy due to their ability to integrate with host tissues and promote favorable biological responses [7]. Among these, mineral trioxide aggregate (MTA) has demonstrated excellent biocompatibility, sealing capability, and antibacterial properties. It can activate fibroblasts in primary teeth, stimulating cytokines secretion that facilitate hard tissue formation, hence possessing the potential to enhance tissue regeneration during pulp therapy [8, 9]. Reported success rates of MTA pulpotomy range from 88.2% to 100% [10–12]. Biodentine has been marketed as a “bioactive dentin substitute” with superior biological and physical properties compared to MTA [13]. NeoPUTTY, a premixed bioceramic putty, was introduced to overcome some drawbacks of MTA such as prolonged setting time, potential discoloration, and handling difficulties. It contains tantalum oxide, dicalcium silicate, and tricalcium silicate, which promote hydroxyapatite formation and healing, and sets upon contact with moisture [14].
Several methods have been used to assess leakage, bacterial leakage test is considered more clinically relevant than dye or fluid-based techniques [15, 16]. Furthermore, various microscopic methods, including stereomicroscopy, scanning electron microscopy (SEM), and transmission electron microscopy (TEM), have been used to assess bacterial colonization on dentin, however, these methods primarily serve descriptive functions, being indirect and non-quantitative, and are incapable of assessing bacterial viability. Thus, confocal laser scanning microscopy (CLSM) has been employed to provide a direct, non-destructive, three-dimensional evaluation of bacterial viability within dentinal tubules by dead/live staining techniques, offering more clinically relevant results than conventional microleakage models [17–19]. In addition, in the present study, environmental scanning electron microscopy (ESEM) was employed to detect interfacial gaps between dentin and pulp capping materials.
To date, no study has evaluated the bacterial sealing ability and viability of Enterococcus faecalis in pulpotomized primary molars treated with NeoPUTTY using advanced imaging techniques including CLSM and ESEM. Unlike previous research on MTA and Biodentine, which relied mainly on conventional microbiological methods, this study provides the first comprehensive histological assessment of NeoPUTTY, Biodentine and MTA under controlled bacterial challenge within the central, mesial, distal, and apical areas of the pulp chamber following pulpotomy, filling a key gap in the literature. This study aimed to compare the sealing ability and antibacterial efficacy of NeoPUTTY, Biodentine, and MTA using a bacterial leakage model with E. faecalis. CLSM was employed to assess bacterial colonization and viability across different pulp chamber regions. This dual-method approach offers new insights into the biological and structural sealing behavior of these materials under standardized conditions. Our null hypothesis stated that there would be no significant differences in total bacterial loads, viability, or interfacial gaps between the three materials.
Materials and methods
Ethical clearance was obtained from the Research Ethics Committee (REC) of the Faculty of Dentistry at Suez Canal University, with permission number (881/2024), in accordance with the principles of the Helsinki Declaration. Informed consent was obtained from parents/legal guardians for the use of extracted teeth. Forty freshly extracted second primary molars (for orthodontic purposes) were collected. Only mandibular second primary molars with sufficient tooth structure, an intact pulpal floor, and at least three intact axial walls were included. Teeth must not have undergone any previous pulp therapy and were required to have at least one-third of the root structure remaining. Molars with extensive caries, cracks or restorations were excluded [20].
Sample size calculation
Using G*Power 3.1.9.6, a minimum of 30 samples was required to detect an effect size of 0.27 with α = 0.05 and β = 0.2 (power = 80%, partial eta²=0.07). To ensure validity, 40 teeth were included [21].
Sample preparation
Teeth were cleaned, polished with pumice, autoclaved at 121 °C for 20 min to ensure internal sterility prior to cavity preparation, and stored in sterile saline until the commencement of the experiment [22].
Standardized pulpotomy cavities were prepared using #330 and #6 carbide burs (Komet,* Lemgo*,* Germany)* under water spray. The teeth were then air dried, and a digital caliper was employed to verify a standardized access cavity diameter of 3 mm x 3 mm [16]. Pulp remnants were removed with K-files up to size 30 (Mani, Japan). During preparation, 5 ml of 2.5% sodium hypochlorite (NaOCl; JK-Dental, Egypt) was used as an irrigant for 1 min, followed by 5 ml of 17% EDTA (Promega, USA) for 1 min to eliminate residual chemical debris [23]. Teeth were disinfected in 2.5% NaOCl for 24 h to eliminate potential surface contamination introduced during handling or preparation, then rinsed and dried with size 30 paper points (Meta Biomed, South Korea) and a small cotton pellet (Roeko, Coltene, Germany) [16].
Sample allocation
Thirty primary mandibular second molars indicated for pulpotomy were sequentially numbered from 1 to 30 and randomly allocated into three groups (n = 10 each) using an online randomization tool (www.randomizer.org), according to the type of base material applied; Group I (n = 10): MTA (Dentsply, USA), Group II (n = 10): Biodentine (Septodont, France) and Group III (n = 10): NeoPUTTY (NuSmile, USA). Additionally, ten teeth served as controls: negative (intact, n = 5) and positive (pulpotomized but unfilled, n = 5). Materials were prepared per manufacturer’s instructions and placed to half of the coronal height. All teeth were preserved in a sterile incubator (Memmert GmbH + Co. Schwabach) at 37 °C and 100% humidity for 24 h to ensure complete material setting, subsequently stored in distilled water at 37 °C for an additional 24 h to simulate clinical conditions and allow continued hydration, maturation, and development of desirable microstructure/sealing ability [16, 24].
Experimental bacterial leakage model and Enterococcus faecalis bacterial contamination
Two layers of nail varnish were applied to the root surfaces of all samples to inhibit bacterial leakage through lateral canals or other irregularities in the cementum. Subsequently, all teeth were affixed utilizing a sterile microleakage model adopted from previous studies [15, 16, 25]. Each tooth was mounted in a 1.5 ml sterilized plastic microtube and then fitted into a sterilized glass vial and sealed with a cyanoacrylate adhesive (3 M,* US)*, followed immediately by bacterial contamination [15, 25]. Enterococcus faecalis (ATCC^®^ 19433) suspension was freshly prepared and placed in the upper chamber of the microtube on Day 1 and replenished every 48 h. to ensure viability of bacteria. Models were incubated at 37 °C in 100% humidity for 21 days [15, 23, 25].
Preparation of samples for evaluation
After 21 days, teeth were embedded in acrylic resin (Triad VLC resin; Dentsply,* York*,* PA)* and sectioned mesio-distally through the pulp chamber and furcation using a diamond saw (Isomet,* Buehler*,* USA)* rotating at 500 rpm under water cooling [15].
Confocal laser scanning microscopy (CLSM)
Half of the specimens from each group were stained using the LIVE/DEAD BacLight Bacterial Viability Kit L-7012 (Molecular Probes,* Eugene*,* OR*,* USA)*, containing separate vials of the two component dyes; SYTO 9 (green-fluorescent nucleic acid stain) and Propidium Iodide (red-fluorescent nucleic acid stain) in a 1:1 mixture. The excitation/emission maxima were 480–500 nm for SYTO 9 and 490–635 nm for propidium iodide. These dyes selectively stain live (intact membrane) and dead (damaged membrane) bacteria, respectively. Then confocal microscopy evaluation was performed immediately after the staining procedure.
Immediately after staining, the confocal laser scanning microscope (Leica Microsystems DMi 8,* CMS GmbH)* was used to observe the stained bacteria. Each specimen was subjected to deep scans performed in a format of 1024 × 1024 pixels to evaluate the central, mesial, distal and apical areas based on anatomical landmarks. The central region was located at the middle of the pulp chamber floor, mesial and distal regions corresponded to the respective pulp horns, and the apical region was defined adjacent to the root canal orifices. Fluorescence intensity was measured as an average of five random fields within the defined boundaries of each region for each sample to assess the degree and amount of bacterial penetration. The vitality of the bacteria was determined according to percentage of live and dead bacteria, and the type of sealing material were assessed [15, 16, 25]. Image processing and analysis was performed using Fiji (ImageJ 2.x) [26]. All measurements were carried out by a single well trained examiner who was blinded to the type of material used to eliminate bias.
Environmental scanning electron microscope (ESEM)
The remaining half of specimens were immersed in varying concentrations of aqueous ethanol—70%, 80%, 90%, 95%, and 100%—for 5 min each to eradicate any residual bacteria, facilitating the examination of the gap and spaces between materials and tooth structure using an environmental scanning electron microscope [16, 27].
The marginal adaptation between the pulp capping materials and cavity dentin walls was evaluated using a high-resolution ESEM (Quanta FEG 250,* FEI*,* USA)* operated at 20 kV. Images were obtained at 1000× and 2000× magnifications, and multiple points (mesial, pulpal floor and distal) along the material–dentine interface were analyzed using ESEM to assess interfacial gaps and marginal adaptation [28]. All measurements were performed by a single calibrated examiner who was blinded to the type of material used to eliminate bias. Summary of the experimental workflow performed is provided in Fig. 1.
Fig. 1. Workflow showing experimental steps performed
Statistical analysis
Data entry was performed using Microsoft Excel sheets for analysis. Mean and Standard Deviation were used to describe normally distributed data. Shapiro-Wilk test was used to test for normality of data distribution. One-way ANOVA with Tukey Post-hoc comparison was used to compare tested groups to assess the difference in bacterial penetration/leak through pulp capping material and the percent of dead and live bacteria. The difference in gap area measurements between different tested groups was also assessed using One-way ANOVA. A two-way between-groups ANOVA was used to evaluate the fluorescence intensity at the apical/mesial/distal/central areas and to compare between the 3 Bio-active materials. Statistical analysis was performed using SPSS Statistical package for analysis (SPSS^®^ sofware, IBM).
Results
Confocal laser scanning microscopy (CLSM) results
Emission wavelengths of 505–550 nm (green, Syto9) and 650–750 nm (red, PI) were collected to visualize Syto 9 and PI, respectEmission wavelengths of 505–550 nm (green, Syto9) and 650–750 nm (red, PI) were collected to visualize Syto 9 and PI, respectively, by two detection channe.
To assess the difference in bacterial penetration/leak through pulp dressing material, total Bacterial Load inside tooth material, as shown by fluorescent intensity, was compared between different groups of materials used. Shapiro-Wilk test showed that the data were normally distributed. One-way ANOVA showed a statistically significant difference between the three groups of material (p = 0.005). The effect size, calculated using eta squared, was 0.686. Tukey Post-hoc testing showed that MTA demonstrated a statistically significant difference in total bacterial count with the highest Bacterial leakage for MTA when compared to both Biodentine and NeoPUTTY (p = 0.008, p = 0.012) respectively. No significant difference in bacterial leakage was found between Biodentine and NeoPUTTY (p = 0.972). These results are shown in Table 1.
Table 1. Total bacterial Leakage/penetration of the three tested bioactive materials as assessed using fluorescent intensity measured by confocal microscopyMeanStd. DeviationStd. Error95% Confidence Interval for MeanMinimumMaximumLower BoundUpper BoundNeoPUTTY71608167.318642471.49321235.741943835.3101272499.35.26E + 79.59E + 7MTA154226888.545312672.422656336.282124315.1226,329,4621.10E + 82.06E + 8Biodentine66531494.623527674.311763837.229093714.5103969274.64.51E + 79.97E + 7Total97455516.850679448.514629896.665255331.4129655702.24.51E + 72.06E + 8
The live bacterial loads in teeth treated with different pulp-capping materials were compared across the apical, mesial, distal, and central regions, as illustrated in Figs. 2, 3, 4, 5 and 6, while the percentage of dead bacteria compared to live bacteria among the tested materials is shown in Fig. 7.
Fig. 2. Load of Live and dead bacteria for the three studied bioactive material as represented by Fluorescent Intensity in central areas
Fig. 3. Load of Live and dead bacteria for the three studied bioactive material as represented by Fluorescent Intensity in Distal areas
Fig. 4. Load of Live and dead bacteria for the three studied bioactive material as represented by Fluorescent Intensity in Apical areas
Fig. 5. Load of Live and dead bacteria for the three studied bioactive material as represented by Fluorescent Intensity in Mesial areas
Fig. 6. Antibacterial effect of different tested pulp capping material assessed using Confocal Microscopy at different visualized sections of examined teeth
Fig. 7. Percentage of dead bacteria compared to live bacteria among the three tested bioactive materials
A significant overall interaction effect was detected in between tested samples (p < 0.0001). There was a statistically significant main effect for type of pulp dressing material (p < 0.0001) with moderate effect size (partial eta squared = 0.369). Post-hoc comparisons using Tukey HSD test indicated that the mean live bacterial load in MTA group was significantly higher than both Biodentine and NeoPUTTY groups (p < 0.0001 for both). The difference between Biodentine and NeoPUTTY did not show statistical significance (p = 0.97) as illustrated in Table 2; Fig. 7.
Table 2. Mean percentage of bacterial killing by different pulp capping materials, expressed as the ratio of dead bacteria to total bacteriaMeanStd. DeviationStd. Error95% Confidence Interval for MeanMinMaxLower BoundUpper BoundNeoPUTTY75.57505.426092.7130566.940984.209168.8080.30MTA78.40008.722384.3611964.520792.279366.6087.60Biodentine70.65007.314143.6570759.011682.288460.0076.30Total74.87507.386242.1322270.182079.568060.0087.60
Considering the evaluated areas, results showed significant differences (p < 0.0001) with small effect size (partial eta squared = 0.087). Live bacterial load was significantly lower in central part compared to both apical areas (p = 0.05) and mesial areas (p < 0.0001). The mesial areas, particularly with MTA, exhibited a significantly higher live bacterial load compared to the other three regions (central, apical, and distal) (p < 0.0001). Conversely, the distal areas demonstrated a significantly lower live bacterial load than the apical regions (p < 0.0001), as illustrated in Figs. 2, 3, 4, 5 and 6).
Scanning electron microscope (ESEM) results
The mean gap widths and standard deviations (µm) between dentin and the pulp dressing materials for each experimental group are presented in Table 3; Fig. 8, and Fig. 9. One-way ANOVA revealed a statistically significant difference in the mean microgap width between groups (F = 5.046, p = 0.008). In particular, the MTA–dentin interface exhibited the highest mean gap width (9.88 ± 4.12 μm), which was significantly greater than that of the NeoPUTTY–dentin interface (7.44 ± 1.46 μm; p = 0.006), and greater, though not significantly, than the Biodentine–dentin interface (8.84 ± 3.99 μm; p = 0.356) (Fig. 9). The difference between Biodentine and NeoPUTTY was also statistically non-significant (p = 0.124).
Table 3. Values of the interphase between tested material and dentin gap area measurements in µMMeanStd. DeviationStd. Error95% Confidence Interval for MeanMinimumMaximumLower BoundUpper BoundBiodentine8.84303.988780.569837.69739.98883.0218.61MTA9.88574.126680.707728.445911.32563.0119.16NeoPUTTY7.44531.463930.223256.99477.89584.7111.91Total8.64743.500670.311868.03029.26463.0119.16
Fig. 8. Representative SEM scanning micrographs displaying cavities filled with different pulp capping materials and representing the gap interphase between tested material and dentin
Fig. 9. Comparison of interphase gap distance between pulp-filling material and dentin among three tested materials
Discussion
The principal aim of the pulpotomy technique is to maintain a functional primary tooth without symptoms until its natural exfoliation occurs [6]. The procedural success is largely dependent on the effectiveness of the coronal restoration in preventing bacterial penetration [29]. The colonization of bacteria in the root canal can elicit an inflammatory response when bacterial byproducts, including exotoxins or endotoxins, infiltrate the periradicular tissues [19, 30]. Bacterial colonization within dentinal tubules and subsequent biofilm formation remain critical challenges in pulpotomy [31], this emphasizes the necessity of using biocompatible materials that provide both an effective seal and antimicrobial properties [15, 32].
The growing importance of calcium silicate in restorative dentistry can be attributed to its excellent biocompatibility, which supports the formation of a high-quality dentin bridge, as well as its ability to create an impermeable barrier over the pulp [28, 33]. In this study, the performance of NeoPUTTY was compared with Biodentine and MTA in pulpotomized mandibular second primary molars, with regard to their sealing ability and antibacterial effects.
In this study, the bacterial leakage model was adopted due to its higher biological and clinical relevance compared to conventional methods such as dye penetration, turbidity, or radioactive tracer tests, which are often influenced by factors like dye molecular size, immersion time, or air entrapment and may not accurately replicate microbial pathways [18, 34–36]. Nevertheless, bacterial leakage models also have limitations, particularly in tracing the exact routes of bacterial invasion. To overcome these drawbacks and enhance the reliability of our findings, CLSM and ESEM were incorporated as complementary techniques. CLSM enabled a direct, non-destructive three-dimensional evaluation of bacterial viability within dentinal tubules, while ESEM allowed detailed visualization of interfacial gaps under hydrated conditions without extensive specimen preparation.
By adopting a bacterial leakage model and integrating confocal laser scanning microscopy (CLSM) and environmental scanning electron microscopy (ESEM), our study offered a more comprehensive and reliable assessment than conventional methods such as dye penetration or turbidity tests, which have well-documented limitations [18, 34–36]. For instance, dye penetration tests are influenced by dye molecular size, pH, immersion time, and the presence of air entrapment, which compromise their reliability [36]. Considering the need for experimental models that accurately replicate microbial colonization pathways, Enterococcus faecalis was selected as the test organism. E. faecalis is the most frequently isolated species in persistent endodontic infections and is well known for its strong capacity for biofilm formation and tissue invasion, making it a highly relevant and an ideal model organism for studying bacterial invasion in the present study [16, 17, 25, 37, 38]. CLSM and ESEM were incorporated as complementary techniques. However, a major limitation of CLSM is that it cannot directly visualize non-fluorescent materials. Therefore, the use of fluorescent dyes, is necessary to visualize the penetration of materials [15].
In the current study, all the positive control samples exhibited fluorescence, confirming the necessity of pulp dressing material, while no fluorescence was observed in the negative control samples, confirmed the reliability of the methodology adopted. The nail polish totally prevented microleakage, with bacterial contamination only penetrating the coronal portion of the teeth. This validates the methodology adopted in the current study [15, 17, 25].Additionally, all experimental procedures were carried out by a single calibrated operator following a standardized protocol to ensure methodological consistency and minimize bias and variability.
According to CLSM analysis, bacterial viability was significantly affected by the type of material used. We found that MTA exhibited the highest bacterial leakage compared to Biodentine and NeoPUTTY (p < 0.0001, for both), with no significant difference between the latter two (p = 0.97), although NeoPUTTY demonstrated the lowest live bacterial load. ESEM further confirmed that NeoPUTTY presented fewer interfacial gaps than both Biodentine and MTA, indicating its superior sealing ability. Therefore, the null hypothesis of this study was rejected.
Our findings are consistent with previous studies [39–45] demonstrated that Biodentine exhibits superior sealing ability and antibacterial properties compared with MTA. This could be attributed to several factors; first, its smaller particle size and lower porosity enable closer adaptation to dentinal walls thus enhancing its marginal sealing, as confirmed by SEM [39, 40] and computed microtomography [41] observations, which demonstrated that Biodentine adapts more closely to dentinal walls than MTA. In another study, it was noted that Biodentine’s sealing ability closely resembled that of apatite crystals when observed under a SEM [42].
Additionally, when Biodentine comes in contact with dentine it leads to the formation of tag-like structures alongside an interfacial layer called the “mineral infiltration zone,” where the alkaline caustic effect of calcium silicate cements hydration products degrades the collagenous component of interfacial dentine. This promotes mineral infiltration into dentin and the subsequent formation of a stable hydroxyapatite layer at the interface, creating a biological seal [43]. Han and Okiji [44] showed that calcium and silicon ion uptake into dentin leading the formation of tag-like structures in Biodentine was higher than MTA. Furthermore, the fast setting time of Biodentine (approximately 12 min) allows for earlier sealing of the dentin–material interface, thereby minimizing the risk of microleakage and bacterial contamination [45].
The antibacterial action of Biodentine is mainly due to its alkalinity and calcium hydroxide release during cement hydration process, which generates a colloidal gel that raises pH to around 12.5, inhibiting bacterial growth and disinfecting the surrounding dentin [46]. It has also been reported to inhibit microbial adhesion and biofilm formation in vivo [47]. This also comes in agreement with previous studies [17, 39, 48] where Biodentine demonstrated superior effectiveness against Enterococcus faecalis compared to MTA.
Although there was no statistically significant difference between Neoputty and Biodentine regarding microleakage (p = 0.124) and bacterial viability (p = 0.972), the least microleakage and lowest bacterial viability were noted in the Neoputty group could be attributed to its premixed formulation, ultrafine tricalcium and dicalcium silicates, and bioactive organic carrier contribute to hydroxyapatite formation, improved sealing and antibacterial activity. Furthermore, its firm, non-tacky consistency, resistance to washout than Biodentine, and notable bioactivity. This is consistent with the findings of [49, 50], who demonstrated its enhanced penetration into dentinal tubules than Biodentine and NeoMTA. Similarly, Acharya et al. [51], in a study comparing Modified NeoPutty MTA^®^, Biodentine, and Calcium Hydroxide in indirect pulp therapy of deciduous teeth, highlighted the favorable properties and superior clinical performance of NeoPutty MTA compared to the other materials evaluated.
In contrast, Acharya et al. reported limited antibacterial activity of NeoPUTTY in zone of inhibition assays against E. faecalis, which improved when antibiotics [52] were added. While, Eid et al. [53] found that it exhibited greater microleakage than ProRoot MTA and Biodentine in dye penetration tests. These differences appear to be method-dependent, since dye penetration models can overestimate leakage due to the very small molecular size of dye particles.
Previous literature has reported conflicting data regarding MTA’s antibacterial effectiveness. Some studies have shown limited activity [54, 55], while others demonstrated antibacterial effects against E. faecalis [15, 56]. Freshly mixed MTA was shown to possess stronger antibacterial properties, and Biodentine has been found to exhibit comparable activity [57].
On the other hand, MTA has been criticized for its drawbacks, including long setting time, handling difficulties, surface disintegration that may compromise marginal adaptation and relatively high cytotoxicity in its freshly mixed stage [54, 55]. Reports on MTA’s antibacterial activity remain inconsistent, with some studies showing limited effects against E. faecalis [56, 57], while others demonstrate measurable antibacterial activity, particularly in freshly mixed formulations [58, 59].
Anatomical variability appears to significantly influence bacterial infiltration. Higher bacterial loads were consistently observed in the mesial and apical areas, likely due to the complex morphology of the mesial pulp horns and the pulp chamber floor. These regions often contain accessory foramina and irregular surfaces, which hinder effective material adaptation and promote bacterial ingress [60, 61]. These findings highlight the critical importance of selecting materials with superior adaptability and optimizing placement techniques to ensure effective coronal sealing.
The presence of microgaps at the material–dentine interface was found to be clinically significant, as these voids facilitate fluid and bacterial penetration, potentially leading to postoperative sensitivity and secondary caries [16, 28]. ESEM results confirmed CLSM findings, showing that NeoPUTTY had significantly the least microgap formation (7.44 ± 1.46 μm) (p = 0.006) compared to MTA, which displayed the highest gap values (9.88 ± 4.12 μm), followed by Biodentine (8.84 ± 3.99 μm). This further supports the superior sealing ability and marginal adaptation of NeoPUTTY, which may reduce the risk of microleakage-related complications.
Limitations
This study has several limitations that should be acknowledged. First, it was conducted under in vitro conditions that cannot fully replicate the complex biological environment of the oral cavity. Second, only a single bacterial species (E. faecalis) was tested, whereas clinical infections typically involve multispecies biofilms. Third, the relatively small sample size and short-term evaluation; thus, long-term changes in antibacterial activity, sealing, and marginal adaptation were not assessed. Finally, outcomes may have been influenced by variables such as dentin characteristics, smear layer presence, laboratory conditions and sample preparation. Also, variations in crown height could have influenced the final thickness of the applied materials, even though standardized access cavity dimensions were used. Further clinical studies with larger sample sizes, long-term follow-up, and inclusion of first permanent molars —commonly treated with pulpotomy— are required to confirm these findings and optimize material selection in pediatric dentistry.
Conclusion
Within the limitations of this in vitro study, Biodentine and NeoPUTTY have significant antibacterial activity, sealing, and marginal adaptation compared to MTA. CLSM and ESEM imaging confirmed that interfacial gaps were directly associated with higher bacterial penetration and surface irregularities, particularly in the MTA group. The enhanced performance of Biodentine and NeoPUTTY may be related to their bioactive composition and improved adaptability. These results provide valuable guidance for clinical decision-making in pediatric dentistry, emphasizing the importance of material selection and interfacial integrity in achieving long-term success.