Shared Decision-Making in Children’s Healthcare by Parents’ Immigrant Status: Findings from the 2021–2022 U.S. National Survey of Children’s Health
Sawsan Salah, Lori Anne Francis

TL;DR
Immigrant parents in the U.S. are more likely to report lower shared decision-making in their child's healthcare compared to U.S.-born parents.
Contribution
This study identifies disparities in shared decision-making by immigrant status and highlights factors that may contribute to these disparities.
Findings
Immigrant parents reported lower levels of shared decision-making in their child's healthcare.
Needing extra help arranging care was associated with significantly higher odds of low shared decision-making among immigrant parents.
Abstract
The increasing immigrant population in the U.S. faces unique challenges in navigating the healthcare system, including language and cultural barriers, and knowledge of services. Immigrant parents may face additional challenges as they attempt to navigate the healthcare system on behalf of their children. This study investigated associations between parents’ immigrant status and their perceptions of shared decision-making (SDM) in their child’s healthcare. Participants included 27,082 parent respondents from U.S. households in the 2021-22 National Survey of Children’s Health. Measures included parents’ immigrant status and reports of shared decision-making in their child’s healthcare. Potential moderators of the association between immigrant status and SDM included time spent providing or arranging children’s healthcare, household economic strain, parenting support, needing extra help to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
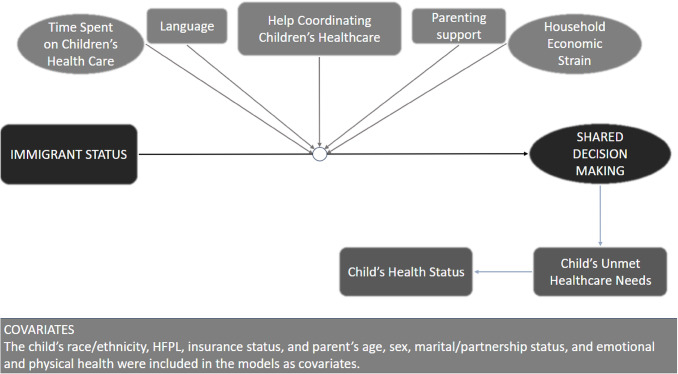 Figure 1
Figure 1- —http://dx.doi.org/10.13039/100006108National Center for Advancing Translational Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPatient-Provider Communication in Healthcare · Migration, Health and Trauma · Palliative Care and End-of-Life Issues
Background
Between 2022 and 2023, the immigrant population in the United States rose from 13.9% [1] to 14.8% [2], accounting for 47.8 million people in 2023; children comprised 6.0% of the immigrant population [2]. Because the U.S. is becoming increasingly diverse, it is important to consider the sociocultural factors affecting children’s access to healthcare [3, 4]. Huang et al. [5] found that U.S.-born children with immigrant parents utilize fewer healthcare services despite being in overall poorer health. This may occur because immigrant families face unique healthcare barriers, including language, and limited knowledge of available services, which may increase health disparities between children with immigrant parents and children with U.S.-born parents [3–6].
Shared decision-making (SDM) in healthcare is a process that involves at least one physician and one patient who discuss and implement an agreed-upon treatment plan [7, 8]. Research showed that SDM and effective patient-provider communication are crucial in influencing healthcare compliance [9–12]. Studies have also shown that SDM is associated with positive health outcomes and patient satisfaction – even among immigrant groups [11, 13]. Yet, disparities exist in SDM. Whites are more likely to engage in SDM than ethnic minority groups [10, 14, 15]. Moreover, ethnic minorities who have lower English proficiency are less likely to receive sufficient information regarding their medical needs and feel empathy from their providers [16–18]. For example, Hispanic and Asian patients report poor communication with their providers [19, 20]. Language barriers may amplify this issue, limiting opportunities for SDM and the quality of care received [21, 22]. While most studies on SDM and its effect on health outcomes were conducted on U.S.-born adults, little is known about SDM in immigrant populations and its impact on children’s health outcomes.
Figure 1 presents this study’s conceptual framework. The study examined the association between parents’ immigrant status and their perceptions of SDM in their children’s healthcare. Associations between SDM children’s general health status and unmet healthcare needs were also examined. Lastly, we examined the extent to which this association was moderated by: (1) time spent providing or coordinating their child’s healthcare, (2) household economic strain, (3) parenting support, (4) needing help arranging or coordinating care, and (5) primary household language.
Fig. 1A conceptual model of the associations between immigrant status and shared decision making, and their relation to child health, healthcare outcomes, and respective moderators
Methods
Study Sampling
Data were drawn from the 2021–2022 waves of the National Survey of Children’s Health (NSCH), a cross-sectional, nationally representative study of children’s health and well-being in households with children < 18 years [23]. Data were collected between June 2021 and January 2023 by the U.S. Census Bureau. Utilizing population-level data provides an opportunity to address healthcare outcomes in a representative sample of immigrant parents, and to generalize findings to the broader U.S. population. This cross-sectional study design allowed us to assess population characteristics and prevalence of immigrant parents, SDM, and unmet children’s health care needs, over a two-year period in the U.S. A stratified sampling frame was used to be representative of households with children across the 50 U.S. states and the District of Columbia. Adult respondents completed surveys in English or Spanish, tailored for children in three age groups: 0–5 years, 6–11 years, or 12–17 years. The response rate for the 2021 survey was 40.3% and 39.1% for 2022. Further information on study methodology and confidentiality protection can be accessed at www.childhealthdata.org. Institutional Review Board approval was received from The Pennsylvania State University (protocol #13946); consent to participate was implied.
Participants
Participants included biological or adoptive parent respondents of children ages 0–17 years living in the same household. Respondents will be referred to as parents from here on. Parents with missing data or reported “No” on whether decisions needed to be made regarding their child’s health were excluded. Lastly, parents were included if they answered one or more follow-up questions about SDM. After applying these inclusion and exclusion criteria, 27,082 parents were included in the analytical sample. Outcome variables have different levels of missingness, leading to different sample sizes. However, those cases were kept to not impact weighting. Children’s race/ethnicity, household federal poverty level, and parent education status, have particularly high levels of missingness in the larger sample and were imputed by the National Center for Health Statistics.
Measures
*Immigrant Status. *Parents reported whether they were born in the U.S. and were categorized as either being U.S.-born or immigrants. Immigrant parents answered a follow-up question: “When did you/this caregiver come to live in the U.S.?” The response was a 4-digit year of migration; time spent in the U.S. was calculated by subtracting the year each parent reported to have arrived in the U.S. from the year the survey was administered. Immigrant parents were categorized into one of the following groups to indicate living in the U.S. between 0 and 4 years, 5–9 years, 10–14 years, or 15 + years, following procedures used by Nwankwo and Wallace [24] and Antecol and Bedard [25].
Shared Decision Making (SDM). SDM is a construct generated from parent responses to three questions. Parents were initially asked whether their children needed decisions to be made regarding their health. If the parent answered “Yes,” three follow-up questions asked the extent to which the child’s doctors/healthcare providers did the following in the past 12 months: discussed a range of healthcare or treatment options, made it easy for parents “to raise concerns or disagree with recommendations,” and worked with the parent on decisions regarding “which healthcare and treatment choices would be best.” Response options were “always,” “usually,” “sometimes,” and “never.” Responses were averaged to create a subscale indicating parents’ reported perceptions of SDM in their child’s healthcare (α = 0.89). The subscale was reverse-coded such that higher scores indicate higher levels of SDM.
Child Unmet Health Care Needs. Parents responded yes/no to the question, “During the past 12 months, was there any time when this [child] needed health care but it was not received?”
Child General Health Status. Parents were asked, “In general, how would you describe this child’s health?” Response options were “excellent,” “very good,” “good,” “fair,” and “poor.” These response options were reverse coded such that higher numbers indicate better general health status and were then dichotomized to indicate children rated with excellent/very good/good health and poor/fair general health.
Language. Parents reported on the primary language used in their home. Options were “English,” “Spanish,” or “Other.” Responses were dichotomized to include “English,” and “Language other than English”.
Time Spent Providing or Coordinating Health Care. Parents reported, how many hours in an average week someone in the household spends time “providing healthcare at home for this child” and “arranging or coordinating health or medical care for this child.” Response options for these two questions ranged from “less than 1 hour,” “1–4 hours,” “5–10 hours,” “11 or more hours per week,” or “this child did not need health coordinated [or provided at home] on a weekly basis.” These items were later dichotomized to include 0–4 and 5 + hours per week.
Support with Child’s Care. Parents responded yes/no to a question asking whether they felt they “could have used extra help arranging or coordinating this child’s care among the different health care providers or services” in the past 12 months.
Parenting Support. Parents responded yes/no to the question, “During the past 12 months, was there someone that you could turn to for day-to-day emotional support with parenting or raising children?”
Household Economic Strain. Economic strain was conceptualized using two items. First, parents reported their difficulty in covering “the basics, like food or housing, on your family’s income” since the child was born. Response options were “never,” “rarely,” “somewhat often,” or “very often.” The term financial strain was used to conceptualize this question. Second, parents reported whether they had “problems paying for any of this child’s medical or healthcare bills,” during the past 12 months. Response options were “yes” or “no.”
Sociodemographics. Parents reported their sex and marital/partnership status, along with their children’s race and ethnicity.
Covariates. Household federal poverty level (HFPL) was included as a covariate in all models. Additional covariates included healthcare insurance at the time of the survey (insured/uninsured), parents’ emotional, and physical health status, and parents’ age at interview.
Statistical Analyses
Analyses were performed using SAS 9.4; PROCSURVEY commands and weights were used to account for the complex survey design. Descriptive analyses were used to describe sample characteristics and to examine frequencies of all main independent and dependent variables, stratified by immigrant status. Adjusted logistic regressions were used to examine significant associations between parent immigrant status and SDM. Lastly, potential moderators of the association between parent immigrant status and SDM were examined. Moderators, including time spent providing or coordinating the child’s healthcare, household economic strain, parenting support, needing extra help arranging or coordinating care, and household language were entered as interaction terms in the multinomial logistic regression models. All moderators were re-coded into binary outcomes before analysis. Moderation effects were identified by determining whether each moderator increased or reduced the odds of SDM among immigrant parents. Logistic regression analyses were conducted sequentially, in a stepwise manner, with each model adjusting for a different set of factors. Model 1 examined unadjusted associations between parent immigrant status and outcome variables. Model 2 adjusted for demographic factors: parent sex, child race, and age. Model 3 adds sociodemographic factors: parent’s marital status, HFPL, and insurance coverage. Model 4 adds parents’ self-reported emotional and physical health.
Given the established association between household poverty and healthcare access [26], and differences in healthcare access by insurance status, logistic regression models were adjusted for HFPL and healthcare coverage. Parent physical health was included as a covariate due to its association with child healthcare access [27, 28]. Preliminary analyses showed that there were significant differences in child race, parent sex, marital status, and mental health by parents’ immigrant status (SI Table A1); these variables were included as covariates in all models.
Results
Descriptive Statistics
Descriptives are represented in Table 1. Less than one-fifth (15%) of parents reported being born outside of the U.S. The majority (70.2%) of immigrant parents reported migrating to the U.S. 15 or more years ago. Nearly 6% reported migrating to the U.S. within the last 4 years, 11% within the last 5–9 years, and 13% within the last 10–14 years. The average reported parent age at migration was 20.3 years (SE = 0.6). Parents who reported their sex as female represented 75.2% of the total sample, and 75.8% reported being married at the time of the survey. The average age of U.S.–born parents was 40.7 (SE = 0.1) years and 41.0 years (SE = 0.5) for immigrant parents. About a fifth of immigrant parents (22.7%) reported having a bachelor’s degree, while 19% reported they did not receive a high school diploma or GED. Immigrant parents had lower average HFPL (220.9%, SE = 11.0) as compared to their U.S.-born counterparts (HFPL = 342.9%, SE = 5.6).
Table 1. Estimates (weighted and unweighted) of sociodemographic characteristics by immigrant status and total populationVariablesImmigrant StatusU.S.-bornImmigrantPopulation Estimate (Weighted) n % (SE) n % (SE) N (in millions)% Number of years in the U.S.
23,929
85.0 (0.5)
2617
15.0 (0.5)
15.5
100.0 0–4 years--1286.1 (1.0)0.10.95–9 years--30010.5 (1.0)0.21.610–14 years--34913.2 (1.4)0.32.015 years +--184070.2 (1.8)1.610.5U.S. – born23,929100.0 (0.0)--13.285.0 Relationship to child Biological or adoptive parent22,064100.0 (0.0)2493100.0 (0.0)14.0100.0 Sex of Primary Caregiver Female17,99076.0 (0.5)176070.2 (1.8)11.775.2Male587524.0 (0.5)86529.8 (1.8)3.824.8 Parent Marital Status Married18,71975.7 (0.6)208376.6 (1.8)11.775.8Not married, living with partner11585.6 (0.3)1358.0 (1.3)0.96.0Never married11506.2 (0.3)1003.7 (0.7)0.95.8Divorced, Separated, or Widowed276112.5 (0.4)28911.7 (1.4)1.912.4 Parent Education Level Less than High School2753.3 (0.3)16719.0 (2.0)0.95.7High school graduate or GED172810.2 (0.4)26815.6 (1.6)1.711.0Vocational, trade, business program, or some college, but no degree386017.3 (0.5)34012.9 (1.3)2.616.6Associate degree21728.1 (0.3)1715.2 (0.8)1.27.6Bachelor’s degree814730.9 (0.6)74522.7 (1.5)4.629.7Advanced or Professional Degree (MA, MS, Ph.D., MD, DDS, DVM, JD)774730.2 (0.6)93924.7 (1.6)4.629.3 Financial Strain Very Often6543.3 (0.2)743.3 (0.7)0.53.3Somewhat often239410.9 (0.4)27714.6 (1.7)1.811.5Rarely or never20,79785.8 (0.4)226182.0 (1.8)13.285.2 Problems paying medical bills Yes331918.2 (0.5)31423.4 (2.4)2.218.8No16,29881.8 (0.5)160876.6 (2.4)9.581.2 Hours spent providing health care at home for this child, per week Less than 1 h305448.0 (1.2)21937.5 (4.4)1.746.71–4 h a week166927.8 (1.1)14523.7 (3.6)1.027.35–10 h a week5339.4 (0.8)6014.4 (5.6)0.410.011 or more hours a week82914.8 (0.9)10924.4 (4.4)0.616.0 Time spent arranging health or medical care, per week (ex, making appointments, locating services) Less than 1 h442265.9 (1.2)39563.7 (4.2)2.565.71–4 h a week165626.0 (1.1)16225.0 (3.6)1.025.95–10 h a week2253.8 (0.6)324.6 (1.5)0.13.911 or more hours a week1814.3 (0.6)276.6 (2.0)0.24.6 Support with Child’s Care Yes348818.8 (0.6)47223.4 (1.9)2.319.5No15,23381.2 (0.6)151476.6 (1.9)9.780.5 Parent’s physical health status Excellent or very good15,39363.0 (0.6)169358.4 (2.1)9.662.3Good health668928.2 (0.6)70030.2 (1.9)4.428.5Fair or Poor17158.8 (0.4)21711.4 (1.6)1.49.2 Parent’s mental/emotional health status Excellent or very good14,66161.0 (0.6)175765.5 (2.0)9.561.6Good health686329.2 (0.6)64524.4 (1.8)4.428.5Fair or Poor23009.8 (0.4)20610.1 (1.3)1.59.8 Someone to turn to for parenting support Yes20,74787.0 (0.4)169655.7 (2.1)12.782.3No305013.0 (0.4)90144.3 (2.1)2.717.7 Language English23,64298.8 (0.2)165252.0 (2.1)14.291.8Spanish1110.8 (0.2)46832.8 (2.1)0.95.6Other780.4 (0.1)48015.2 (1.3)0.42.6n = 23,929n = 2630Median95% CISEMedian95% CISE Shared Decision Making 3.7(3.7, 3.7)0.03.6(3.4, 3.9)0.1Age40.7(40.4, 41.0)0.141.0(40.2, 42.0)0.5 Federal Poverty Level 342.9(331.9, 354.0)5.6220.9(199.3, 242.5)11.0 Migration Statistics** n = 2630Age at Migration (Years) -
-
- 20.3(19.0, 21.5)0.6Year of U.S. Migration -
-
- 2000.2(1999.2, 2001.2)0.5Bold indicates construct names or the general category that a variable would fall under*Age of the parent completing the survey and their federal poverty level**Calculated age at migration and the year parents migrated is reported for immigrant parents only
Among immigrant parents, 3.3% reported experiencing financial strain “very often.” On average, 23.4% of immigrant and 18.2% of U.S.-born parents reported experiencing problems paying their child’s medical bills. Over one-third of immigrant parents (38.8%) and one-quarter of U.S.-born parents (24.2%) reported spending 5 + hours a week, on average, providing health care at home for their child. Roughly one-tenth of immigrant (11.2%) and U.S.-born (8.1%) parents reported spending 5 + hours a week, on average, arranging healthcare services. Most immigrant (76.6%) and U.S.-born parents (81.2%) reported that they did not need extra help coordinating care for their child. More U.S.-born parents reported they had someone to turn to for parenting support (87%) as compared to immigrant parents (55.7%). The majority of immigrant (58.4%) and U.S.-born (63%) parents reported themselves to be in excellent or very good physical health. Most immigrant parents (65.5%) and U.S.-born parents (61%) reported being in excellent or very good mental or emotional health. English was reported as the primary household language by 52% of immigrant parents and 98.8% of U.S.-born parents.
Associations between Parent Immigrant Status, SDM, and Child Health Outcomes
Table 2 presents stepwise analyses of the associations between immigrant status and reports of SDM, child health status, and unmet healthcare needs. Results showed that compared to U.S.-born parents, immigrant parents had significantly higher odds of reporting lower levels of SDM, after adjusting for demographic, socioeconomic, and parent health factors (p < 0.01). Compared to U.S.-born parents, immigrant parents also had higher odds of reporting that their child was in fair or poor health (p < 0.01). There were no significant associations between immigrant status and reports of children’s unmet healthcare needs (Table 2).
Table 2. Associations between parent immigrant status and SDM, child health status, and unmet health care needsVariableModel 1: UnadjustedModel 2: Demographic Factors^a^Model 3: Socioeconomic Factors^b^Model 4: Health of Parent^c^ n OR (95%CI)p-value n OR (95%CI)p-value n OR (95%CI)p-value n OR (95%CI)p-valueShared Decision Making26,5061.8 (1.6,** 2.2)** < 0.01 26,3781.8 (1.5,** 2.2)** < 0.01 24,2511.7 (1.4,** 2.0)** < 0.01 26,0601.7 (1.5,** 2.1)** < 0.01 Child health status26,49526,36426,17126,041 Fair or poor health 1.7 (1.3,** 2.1)** < 0.01 1.7 (1.4,** 2.1)** < 0.01 1.4 (1.2,** 1.8)** < 0.01 1.5 (1.2,** 1.9)** < 0.01 Unmet healthcare needs26,50426,37426,18126,051 Yes 1.2 (0.9, 1.6)0.191.2 (0.9, 1.6)0.211.0 (0.7, 1.4)0.971.1 (0.8, 1.5)0.63Note: Immigrant parents are compared to the reference group, U.S.-born parents^a^Model 2 adjusted for: sex of parent, race of child, parent age^b^Model 3 adjusted for: sex of parent, race of child, parent age, parent’s marital status, federal poverty level, child insurance coverage^c^Model 4 adjusted for: sex of parent, race of child, parent age, parent’s marital status, federal poverty level, child insurance coverage, parent’s mental and physical healthAssociations significant at α = 0.05 are represented in bold
Table 3 presents associations between immigrant status and potential moderators. Compared to U.S.-born parents, immigrant parents reported significantly higher odds of spending 5 + hours a week providing care at home for their child after adjusting for demographic, socioeconomic, and parental health variables (p < 0.01). Immigrant parents, as compared to U.S.-born parents, also had significantly higher odds of reporting they needed extra help with care coordination (p = 0.04).
Table 3. Associations with and moderating effects of time spent on healthcare, economic strain, household language, and parenting support on the association between immigrant status and SDM Variable Model 1:UnadjustedModel 2:Demographic Factors^a^Model 3:Socioeconomic Factors^b^Model 4:Health of Parent^c^Moderation EffectSDMnOR (95%CI)p-valuenaOR (95%CI)p-valuenaOR (95%CI)p-valuenaOR (95%CI)p-valuenaOR (95%CI)p-value Time Spent on Healthcare Time spent arranging care71007071702669846979 5 + hours a week 1.4 (0.8, 2.5)0.171.5 (0.9, 2.5)0.161.4 (0.8, 2.4)0.281.4 (0.8, 2.4)0.280.9 (0.4, 2.0)0.84Time spent providing care at home66186592655365126505 5 + hours a week 2.0 (1.2,** 3.2)** < 0.01 2.0 (1.2,** 3.2)** < 0.01 1.8 (1.1,** 2.9)** 0.01 1.8 (1.2,** 2.8)** < 0.01 1.1 (0.5, 2.5)0.77 Support with Child’s Care Needed extra help with care coordination20,70720,60220,46020,36320,335 Yes 1.3 (1.1,** 1.6)** 0.01 1.3 (1.1,** 1.7)** 0.01 1.2 (1.0, 1.5)0.091.3 (1.0,** 1.6)** 0.04 3.2 (2.1,** 4.9)** < 0.01
Economic Strain Financial Strain26,45726,33826,16326,03325,994 Very Often 0.8 (0.6,** 1.0)** 0.04 0.7 (0.6,** 1.0)** 0.02 0.9 (0.7, 1.1)0.330.9 (0.7, 1.1)0.261.5 (0.9, 2.3)0.09Problems paying medical bills21,53921,46121,33521,24021,215 Yes 1.4 (1.1,** 1.8)** 0.02 1.5 (1.1,** 1.9)** < 0.01 1.2 (0.9, 1.6)0.141.3 (1.0, 1.7)0.670.8 (0.5, 1.3)0.36 Household Language 26,43126,30526,11125,98225,940 English 0.01 (0.01,** 0.02)** < 0.01 0.01 (0.01,** 0.02)** < 0.01 0.01 (0.01,** 0.02)** < 0.01 0.01 (0.01,** 0.02)** < 0.01 1.4 (1.0, 1.9)0.06 Parenting Support Someone to turn to for emotional and parenting support26,39426,27326,10325,97625,941 No 5.3 (4.4,** 6.4)** < 0.01 5.2 (4.4,** 6.3)** < 0.01 4.7 (3.9,** 5.7)** 0.01 5.0 (4.1,** 6.1)** < 0.01 1.3 (1.0, 1.8)0.09Note: In Models 1–4, immigrant parents were compared to the reference group, U.S.-born parentsModeration effect comparisons were made within immigrant parents. Parents who reported: spending 5 + hours a week on healthcare, needing extra help with care coordination, experiencing financial strain somewhat or very often, having problems paying medical bills, their primary household language to be a language other than English, and not having parental support were compared to the reference groups, parents who reported spending 0–4 h a week on healthcare, not needing extra help with care coordination, experiencing financial strain rarely or never, not experiencing problems paying medical bills, English as their primary household language, and having parental support, respectively^a^Model 2 adjusted for: sex of parent, race of child, parent age^b^Model 3 adjusted for: sex of parent, race of child, parent age, parent’s marital status, federal poverty level, child insurance coverage^c^Model 4 adjusted for: sex of parent, race of child, parent age, parent’s marital status, federal poverty level, child insurance coverage, parent’s mental and physical healthAssociations significant at α = 0.05 are represented in bold
Compared to U.S.-born parents, immigrant parents had significantly lower odds of reporting that they experience financial strain “Very Often” in the model adjusting for demographic factors (p = 0.02). This association was no longer significant after adjusting for socioeconomic or parent health factors. After adjusting for demographic factors, immigrant parents had significantly higher odds of reporting they experienced problems paying for their child’s healthcare (p < 0.01) compared to U.S.-born parents. This association was no longer significant after adjusting for socioeconomic or parent health factors. Immigrant parents showed significantly lower odds of reporting “English” as their primary household language, as compared to their U.S.-born counterparts (p < 0.01). Lastly, immigrant parents, compared to U.S.-born parents, showed significantly higher odds of reporting that they did not have someone to turn to for parenting support (p < 0.01), after adjusting for all demographic, socioeconomic, and parent health variables.
Moderation Effects
Table 3 also presents estimates for moderation effects. We examined whether moderating variables emerged as risk or protective factors for SDM among immigrant parents. Thus, these findings can be interpreted as the extent to which the moderating variable increased (OR > 1) or decreased (OR < 1) the odds of parents reporting lower levels of SDM. Compared to their counterparts, immigrant parents who reported needing extra help with care coordination had significantly higher odds of reporting lower levels of SDM (p < 0.01). No other variables emerged as significant moderators in the association between immigrant status and SDM.
Discussion
Findings from this study provide evidence of inequities in SDM among immigrant parents. To the best of our knowledge, this is the first study to examine the association between parent immigrant status and SDM with children’s healthcare providers on children’s health outcomes in a nationally representative survey. Immigrant parents had significantly higher odds of reporting (1) lower levels of SDM, (2) higher odds of reporting that their children were in fair or poor health, and (3) that they spent more time providing healthcare at home, compared to U.S.-born parents. A previous study showed that having someone more knowledgeable about the healthcare system assist with appointments increased informed decision-making [29]; however, this was examined among African immigrants. We add to these findings by showing that when immigrant parents felt they had sufficient assistance with their child’s healthcare coordination (i.e., between different healthcare providers), they reported higher levels of SDM, compared to immigrant parents who reported needing extra help with care coordination.
We did not find evidence for emotional support with parenting as a significant moderator of the association between immigrant status and SDM. This finding contradicts what is in the literature, as previous studies show that parenting social support, (i.e., social support from a family/friend) is a facilitator in the SDM process [30, 31], and critical in establishing health-seeking behaviors [29, 32, 33]. However, compared to other sources of support, parental emotional support is a more general form of parenting support, which may explain why it was a less salient moderator, compared to support with care coordination. Together, findings from the present study suggest that programs that provide support with care coordination may be important in improving SDM among immigrant parents, which may reduce inequities in SDM due to immigrant status.
A systematic review found that common barriers to SDM in pediatric clinics include environmental factors, such as time and access to resources [30]. Individuals who resettle to the U.S. have been shown to struggle with seeking help for medical conditions [5, 34]. A previous study found that African mothers would seek medical help only when they believed the benefits outweighed the barriers, including health literacy and the complexity of the healthcare system [29]. As a result, patients who do not receive the support they need in utilizing the healthcare system may be less likely to engage in the SDM process. This may have substantial effects on patient’s healthcare quality and health outcomes [30, 35]. Few studies have examined the effects of parents’ SDM in children’s health care on children’s health outcomes; we are not aware of any such published studies in immigrant parents.
Study Strengths and Limitations
This study included data from a large, nationally representative sample, allowing for the generalization of findings to U.S. households with children. However, this study is not without limitations. The cross-sectional design limits our ability to infer causality. In addition, data collection took place between June 2021 and January 2023, overlapping with the COVID-19 pandemic. Associations reported in this sample may be characteristically different from what may have been reported before the pandemic. Furthermore, the length of the NSCH may have contributed to response bias. The NSCH also may not represent families who do not speak English or Spanish, as the surveys were only offered in those languages. This study may not be fully representative of immigrant parents because (1) our operationalization of “immigrant status” is limited to what was available in the NSCH, which lacks details accounting for residency, visa status, or citizenship, and (2) most immigrant parents in this study reported living in the U.S. for 15 + years making them differ from more recent immigrants as a result of acculturation [25, 36] and insurance status [37]. Future studies should include more detailed emigration data to allow for a more nuanced understanding of the association between SDM and immigrant status.
Conclusions and Implications for Practice
Findings from this study add to the SDM literature by highlighting the need for SDM and support in coordinating children’s health care in immigrant parents. Doing so may improve patient health outcomes and increase healthcare utilization [35, 37]. Culturally appropriate, community-based partnerships between parents and healthcare providers have been shown to assist immigrants in navigating the healthcare system [34, 38, 39]. Future studies should investigate additional factors that may increase SDM in immigrant parents such as using more detailed information on immigrant status and experiences navigating the health care system for children.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary material 1 (DOCX 14.7 kb)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1U.S. Census Bureau. Selected Characteristics of the Native and Foreign-Born Populations [Internet]. American Community Survey; 2022 [cited 2025 Jan 15]. Available from: https://data.census.gov/table/ACSST 1Y 2022.S 0501?q=Native and Foreign-Born&g = 010XX 00US&y = 2022.
- 2U.S. Census Bureau USD of C. Selected Characteristics of the Native and Foreign-Born Populations [Internet]. American Community Survey; 2023 [cited 2025 Jan 15]. Available from: https://data.census.gov/table/ACSST 1Y 2023.S 0501?q=Native and Foreign-Born&g = 010XX 00US&y = 2023.
- 3Betz CL. Immigrant Children: Unmet Needs and a Myriad of Nursing Concerns. J Pediatr Nurs [Internet]. 2008 [cited 2023 Feb 20];23:157–60. Available from: https://linkinghub.elsevier.com/retrieve/pii/S 088259630800118810.1016/j.pedn.2008.02.00118492544 · doi ↗ · pubmed ↗
- 4Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: What does it mean? (or it takes at least two to tango). Soc Sci Med [Internet]. 1997 [cited 2023 Jun 30];44:681–92. Available from: https://linkinghub.elsevier.com/retrieve/pii/S 027795369600221310.1016/s 0277-9536(96)00221-39032835 · doi ↗ · pubmed ↗
- 5Clever SL, Ford DE, Rubenstein LV, Rost KM, Meredith LS, Sherbourne CD et al. Primary Care Patients’ Involvement in Decision-Making Is Associated With Improvement in Depression. Med Care [Internet]. 2006 [cited 2023 Jul 23];44:398–405. Available from: https://journals.lww.com/00005650-200605000-0000310.1097/01.mlr.0000208117.15531.da 16641657 · doi ↗ · pubmed ↗
- 6Fiks AG, Mayne SL, Karavite DJ, Suh A, O’Hara R, Localio AR et al. Parent-Reported Outcomes of a Shared Decision-Making Portal in Asthma: A Practice-Based RCT. Pediatrics [Internet]. 2015 [cited 2023 Jun 30];135:e 965–73. Available from: https://publications.aap.org/pediatrics/article/135/4/e 965/33582/Parent-Reported-Outcomes-of-a-Shared-Decision 10.1542/peds.2014-3167 PMC 437946325755233 · doi ↗ · pubmed ↗
- 7Kaplan SH, Greenfield S, Ware JEJ. Assessing the Effects of Physician-Patient Interactions on the Outcomes of Chronic Disease. Med Care [Internet]. 1989;27. Available from: https://journals.lww.com/lww-medicalcare/Fulltext/1989/03001/Assessing_the_Effects_of_Physician_Patient.10.aspx 10.1097/00005650-198903001-000102646486 · doi ↗ · pubmed ↗
- 8Staiti AB, Hurley RE, Katz A. Stretching the safety net to serve undocumented immigrants: community responses to health needs. Issue Brief Cent Stud Health Syst Change. 2006;1–4.16506345 · pubmed ↗