Posterior Splenic Abscess Leak Causing Salmonella Group B Peritonitis in an Immunocompetent Young Adult
Michael W Alchaer, Paul Farag, Insoon Park, Thomas A Abbruzzese

TL;DR
A rare case of a splenic abscess caused by Salmonella in a healthy young adult led to peritonitis and was successfully treated with laparoscopic surgery and antibiotics.
Contribution
This case report documents an extremely rare occurrence of Salmonella Group B splenic abscess rupture in an immunocompetent adult.
Findings
Salmonella enterica serogroup B was isolated from blood, peritoneal fluid, and splenic drainage.
The patient was successfully treated with laparoscopic washout, adjusted antibiotics, and image-guided drainage.
The case emphasizes the importance of considering splenic pathology in Salmonella bacteremia with peritonitis, even in immunocompetent individuals.
Abstract
Splenic abscess is an uncommon intra-abdominal abscess, typically associated with immunocompromised states. This report highlights a case where the abscess was caused by Salmonella species in an immunocompetent individual, which is a very rare occurrence with limited prior documentation. We report a previously healthy 24-year-old male who presented with high-grade fever and diffuse abdominal pain. Preoperative CT imaging demonstrated hepatosplenomegaly and a 5.6 × 3.8 cm posterior splenic lesion. Exploratory laparoscopy revealed four-quadrant purulent peritonitis without hollow-viscus perforation and a posterior splenic capsular tear with oozing. Cultures from blood, peritoneal fluid, and a subsequent percutaneous splenic drain all grew Salmonella enterica serogroup B. Spontaneous leak of a splenic abscess causing diffuse peritonitis without gastrointestinal perforation is extremely…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1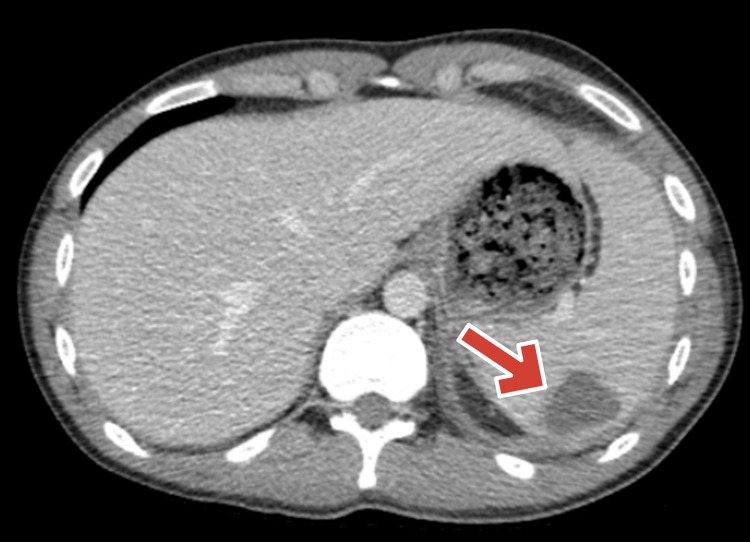 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Appendicitis Diagnosis and Management · Abdominal vascular conditions and treatments
Introduction
Splenic abscesses are uncommon, representing less than 1% of all intra-abdominal abscesses [1,2]. They typically occur in patients with underlying immunocompromised conditions such as diabetes, end-stage renal disease, or malignancy [3]. Salmonella species are an unusual etiology and are most often reported in individuals with significant comorbidities [4,5]. Splenic abscesses most commonly arise from hematogenous seeding during bacteremia, with Staphylococcus, Streptococcus, and Escherichia coli among the most frequently isolated organisms [1-5].
Spontaneous rupture of a splenic abscess leading to diffuse peritonitis is exceptionally rare and can clinically mimic hollow-viscus perforation [6-8]. Although Salmonella peritonitis more commonly arises from gastrointestinal perforation or peritoneal dialysis [9,10], cases of splenic abscess rupture in otherwise healthy, immunocompetent adults have been documented [11,12].
Case presentation
A 24-year-old male with no significant past medical or surgical history presented with a two-day history of high-grade fever (maximum temperature 40.5°C) and progressively worsening diffuse abdominal pain involving all four quadrants. The pain was constant, severe, and associated with generalized abdominal tenderness. He denied nausea, vomiting, diarrhea, hematochezia, or recent abdominal trauma.
On physical examination, the patient was febrile and tachycardic, with diffuse abdominal tenderness and guarding. Initial laboratory evaluation demonstrated stable hemoglobin levels, no leukocytosis, and an otherwise unremarkable metabolic panel. Blood cultures obtained on preoperative day 1 later grew Salmonella enterica serogroup B.
Contrast-enhanced CT of the abdomen and pelvis on pre-op day one demonstrated hepatosplenomegaly and a 5.6x3.8 cm posterior splenic lesion (Figure 1).
Contrast-enhanced CT abdomen/pelvis (pre-op day 1) showing a 5.6x3.8 cm posterior splenic lesion with hepatosplenomegaly.Arrow pointing at the splenic lesion.
Empiric broad-spectrum intravenous antibiotics were initiated preoperatively upon suspicion of intra-abdominal infection. On pre-op day 0, worsening abdominal pain and rebound tenderness prompted exploratory laparoscopy. Intraoperative findings included four-quadrant purulent peritonitis without evidence of hollow viscus perforation. A posterior splenic capsular tear with localized oozing was identified; the tear was associated with localized oozing without evidence of fibrosis, scarring, or chronic inflammatory changes, suggesting a recent capsular disruption likely related to abscess expansion rather than prior trauma. A 19 Fr Jackson-Pratt (JP) drain was placed in the left upper quadrant adjacent to the posterior splenic capsule. Peritoneal fluid cultures obtained intraoperatively grew Salmonella Group B.
The patient was started on intravenous ceftriaxone; however, he developed an allergic rash on post-op day two, prompting a switch to meropenem. He remained hemodynamically stable but continued to have localized abdominal tenderness.
On post-op day 13, interventional radiology placed a percutaneous drain into the posterior splenic lesion. Culture from this drain also grew Salmonella Group B, confirming the spleen as the source of infection. All other cultures were negative. A CT scan on post-op day 18 demonstrated decreased size of the splenic collection (2.2x1.8 cm) and improved associated inflammation (Figure 2). All drains were removed by post-op day 20, and the patient was transitioned to oral trimethoprim-sulfamethoxazole for completion of therapy. He was discharged in stable condition without complications.
Post-op day 18 CT abdomen/pelvis showing interval decrease in size of splenic collection after drainage (2.2x1.8cm).Arrow pointing at the splenic collection.
Discussion
Splenic abscess is a rare clinical entity, accounting for less than 1% of intra-abdominal abscesses and typically affecting individuals with underlying immunocompromised states such as diabetes, end-stage renal disease, or malignancy [1-3]. Salmonella species represent an uncommon cause, most frequently occurring in patients with comorbidities; however, isolated reports describe splenic abscesses in otherwise healthy adults [4,5,11,12].
Spontaneous rupture or leak of a splenic abscess leading to diffuse peritonitis without gastrointestinal perforation is exceptionally uncommon. Published case reports and small series emphasize the importance of considering splenic pathology when diffuse peritonitis occurs in the absence of bowel perforation [6-8,13]. In the present case, the diagnosis was confirmed microbiologically, as Salmonella Group B was isolated from blood, peritoneal fluid, and percutaneous splenic drainage cultures, confirming the spleen as the infection source [4,12,14].
While most cases described in the literature involve patients with significant comorbidities or immunosuppression, splenic abscesses secondary to Salmonella infection have been reported in immunocompetent individuals [11,12,15]. In such patients, splenic preservation is feasible when adequate source control is achieved through image-guided drainage or minimally invasive washout, supplemented with targeted antimicrobial therapy. This spleen-sparing approach mitigates the lifelong risk of postsplenectomy sepsis while maintaining immune function.
Management strategies for splenic abscesses depend on abscess size, number, and patient stability. Standard treatment involves prompt source control through either percutaneous drainage or splenectomy, coupled with pathogen-directed antibiotics and follow-up imaging to ensure resolution [4,5,15]. Although Salmonella peritonitis more commonly results from gastrointestinal perforation or peritoneal dialysis [9,10,16,17], clinicians should maintain vigilance for splenic involvement when Salmonella bacteremia presents with diffuse peritoneal signs.
Conclusions
This case highlights an unusual presentation of Salmonella Group B peritonitis originating from a posterior splenic abscess leak in an immunocompetent young adult, one of the very few such cases documented in the literature. Prompt recognition, early operative washout, targeted antibiotic therapy after allergy-related regimen adjustment, and image-guided drainage achieved effective source control while preserving splenic function.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management of splenic abscess: Report on 16 cases from a single center Int J Infect Dis Ferraioli G Brunetti E Gulizia R Mariani G Marone P Filice C 5245301320091907052610.1016/j.ijid.2008.08.024 · doi ↗ · pubmed ↗
- 2Splenic abscess: A single institution study and review of the literature Yonsei Med J Lee WS Choi ST Kim KK 2882925220112131934810.3349/ymj.2011.52.2.288PMC 3051211 · doi ↗ · pubmed ↗
- 3Splenic abscess in the new millennium: A descriptive, retrospective case series Open Forum Infect Dis Radcliffe C Tang Z Gisriel SD Grant M 09202210.1093/ofid/ofac 085PMC 892338235299986 · doi ↗ · pubmed ↗
- 4Two cases of salmonella splenic abscess Med J Armed Forces India Piplani S Ramakrishna Ramakrishna Nandi B Ganjoo RK Madan R Chander BN 77786220062740785410.1016/S 0377-1237(06)80167-XPMC 4923292 · doi ↗ · pubmed ↗
- 5Splenic abscess due to Salmonella enteritidis Infect Dis Rep Cabadak H Erbay A Karaman K Sen S Tezer-Tekçe Y 04201210.4081/idr.2012.e 4PMC 389266424470934 · doi ↗ · pubmed ↗
- 6Non-traumatic rupture of voluminous non-typhoid Salmonella splenic abscess presenting with peritonitis: Case report and review of the literature Int J Surg Case Rep Evola G Piazzese E Cantella R Iudica M Veroux G SarvàS 1601637920213347707510.1016/j.ijscr.2020.12.081PMC 7815976 · doi ↗ · pubmed ↗
- 7Generalized peritonitis due to a ruptured splenic abscess Am J Surg Knauer QF Abrams JS 923926112,61966592381310.1016/0002-9610(66)90152-8 · doi ↗ · pubmed ↗
- 8Non-traumatic ruptured splenic abscess presenting with pneumoperitoneum in an immunocompetent patient: A diagnostic dilemma BMJ Case Rep Agarwal N Sharma A Garg G 12201910.1136/bcr-2018-228961 PMC 650605431068349 · doi ↗ · pubmed ↗