Cardioprotective effect of resveratrol in myocardial ischemia/reperfusion injury and myocardial infarction: a pre-clinical meta-analysis in animal studies
Shi-Jie Wei, Qi-Hao Guo, Xin-Yu Wei, Si-Yu Chen, Sheng Deng, Liang An, Wen-Jing Zeng, Yi-Fan Zeng

TL;DR
This study finds that resveratrol may protect the heart in animal models of heart injury, but more research is needed to confirm its effectiveness in humans.
Contribution
A pre-clinical meta-analysis showing resveratrol reduces heart damage in animal models of ischemia/reperfusion injury and myocardial infarction.
Findings
Resveratrol treatment decreased myocardial infarct size in MIRI and MI animal models.
Resveratrol improved cardiac function and reduced oxidative stress and inflammation in heart injury models.
The study highlights the need for standardized protocols and clinical trials to confirm resveratrol's cardioprotective effects.
Abstract
This meta-analysis aimed to assess the cardioprotective effect of resveratrol (RES) against myocardial ischemia/reperfusion injury (MIRI) and myocardial infarction (MI) in the animal. PubMed, Web of Science, and EMBASE were searched. Primary outcomes included myocardial infarct size (IS) and cardiac function. Secondary outcomes included cardiac injury enzyme, oxidative stress level, inflammatory cytokine, and apoptosis rate. Subgroup analysis, publication bias, sensitivity analysis, meta-regression, and dosage-efficacy analysis were used to evaluate the risk of bias. Fifty-seven studies were included involving 1,125 animals. The results showed that RES treatment decreased IS in animal models of MIRI (SMD: −5.44; 95% CI [−6.42 to −4.45]; P < 0.01; I2 = 86%) and MI (SMD: −3.41; 95% CI [−4.44 to −2.38]; P < 0.01; I2 = 75%). Moreover, RES treatment improved cardiac function, decreased…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
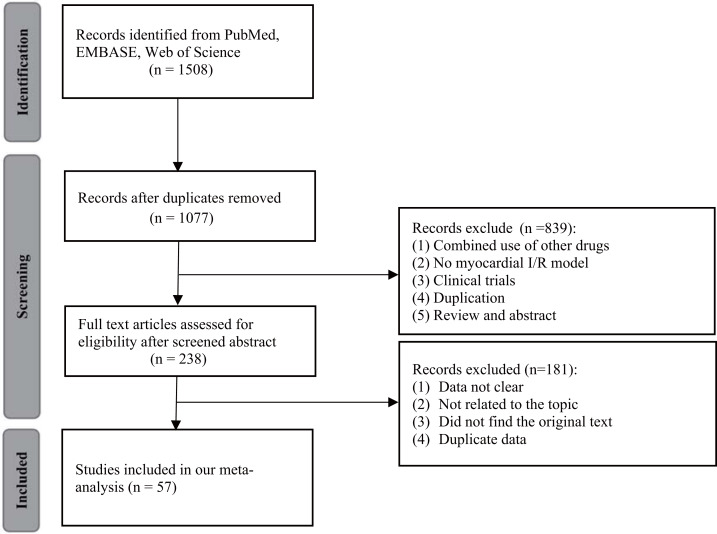 Figure 1
Figure 1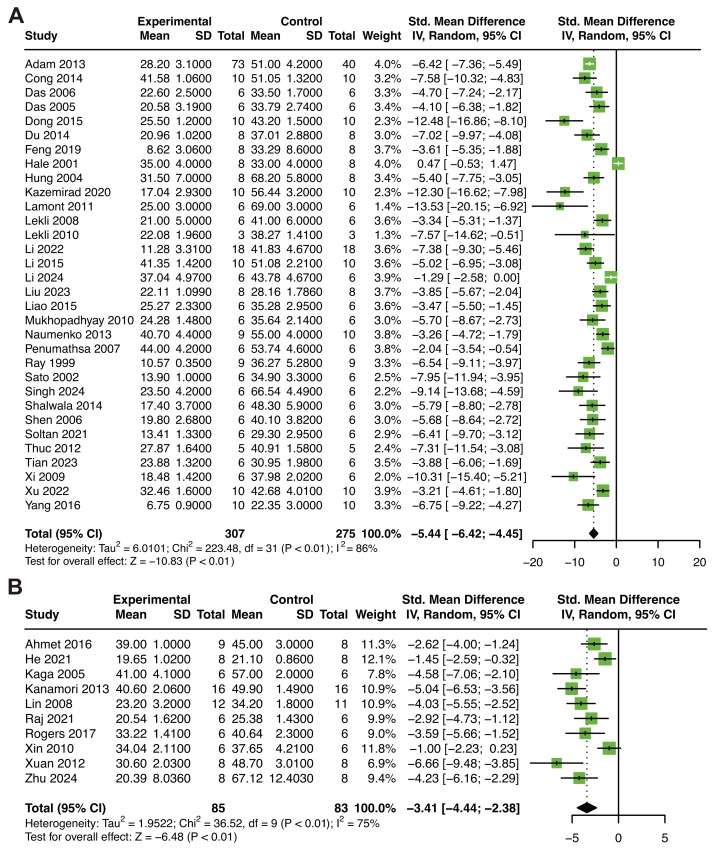 Figure 2
Figure 2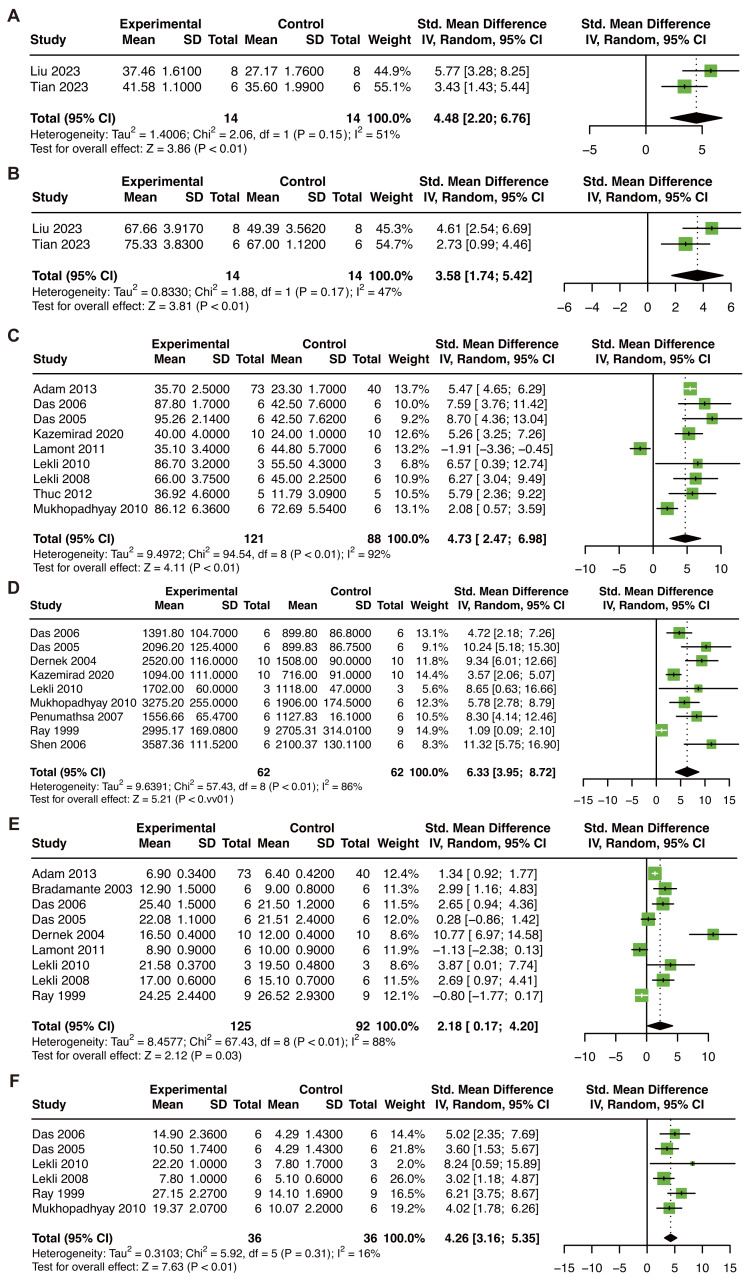 Figure 3
Figure 3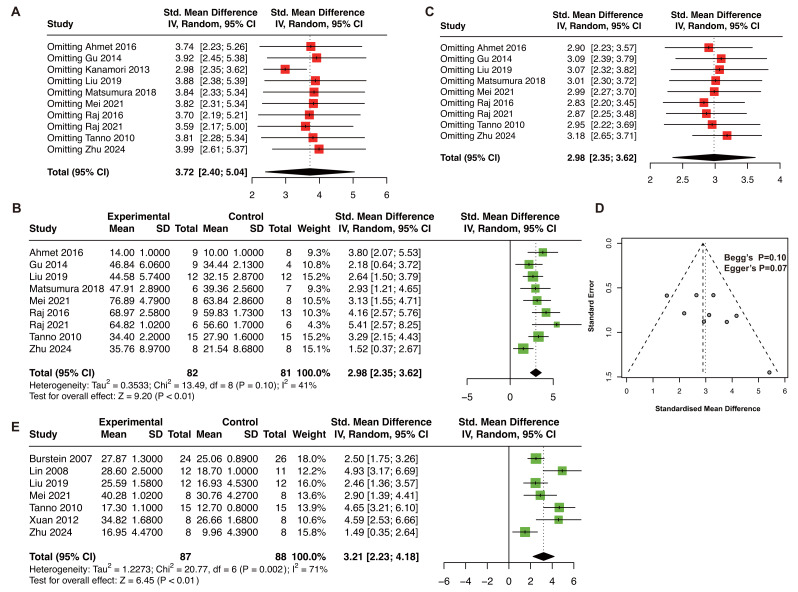 Figure 4
Figure 4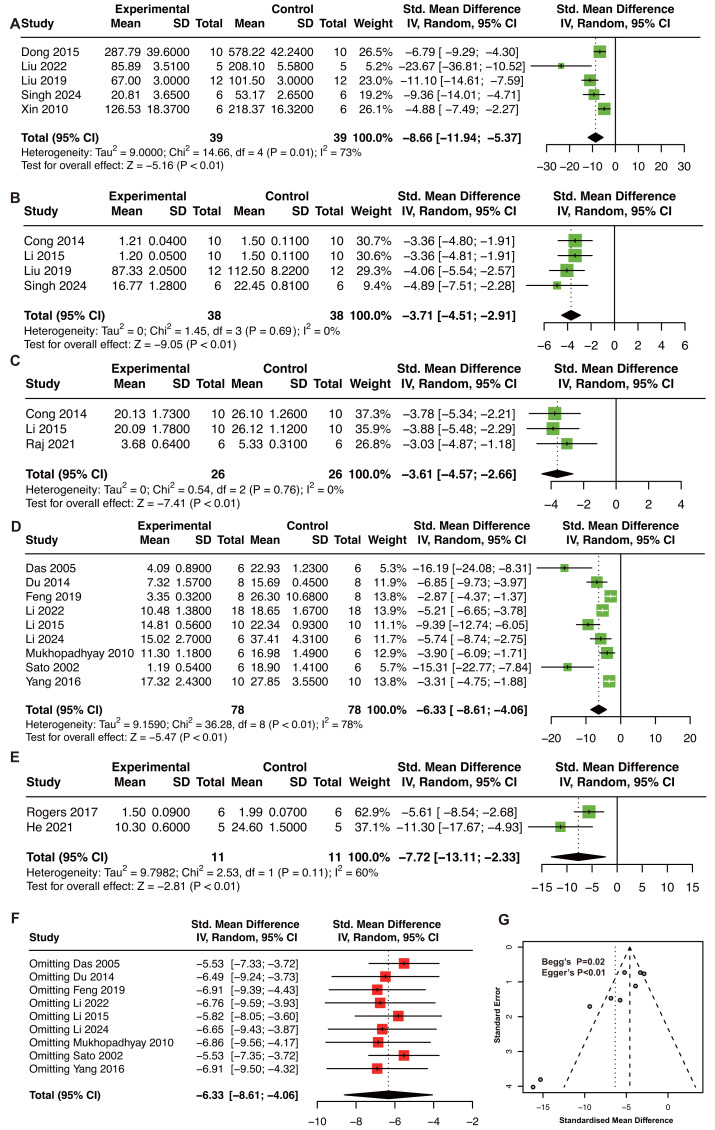 Figure 5
Figure 5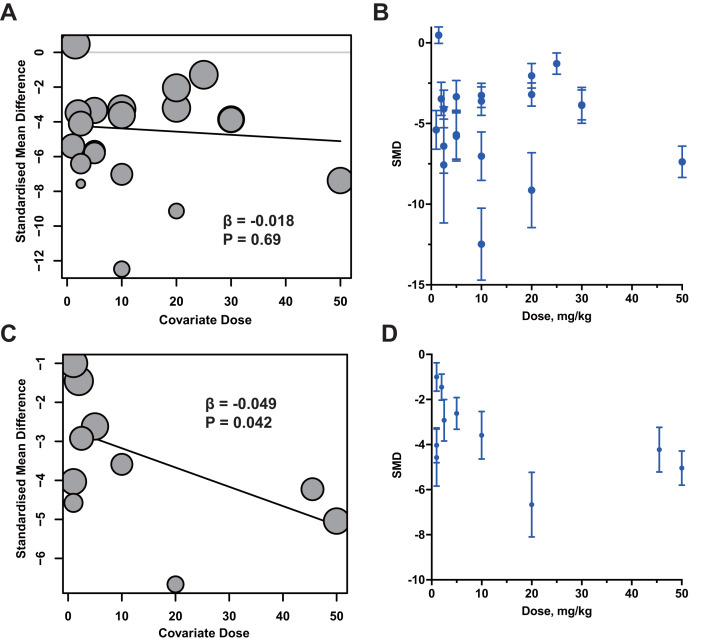 Figure 6
Figure 6- —The Hunan Provincial Natural Science Foundation of China
- —The Changsha Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSirtuins and Resveratrol in Medicine · Cardiac Ischemia and Reperfusion · Cardiac Fibrosis and Remodeling
Introduction
Cardiovascular diseases (CVDs) have become the leading cause of mortality throughout the world, with acute myocardial infarction (AMI) being the deadliest (Roth et al., 2020). AMI results from sudden coronary occlusion that causes severe and prolonged myocardial ischemia. The standard treatment strategy for rescuing ischemic myocardium is timely reperfusion therapy (such as PCI or thrombolysis) (Rao et al., 2025). Myocardial reperfusion therapy can timely and effectively restore the blood supply function of ischemic myocardial tissue, save ischemic myocardial cells, reduce myocardial infarction area, preserve left ventricular systolic function, and prevent heart failure (Jensen, Hjortbak & Bøtker, 2020; Wang et al., 2022). However, the restoration of blood flow itself may induce additional cellular injury, known as myocardial ischemia/reperfusion injury (MIRI), which aggravates irreversible apoptosis and necrosis of cardiomyocytes through Ca^2+^ overload, oxidative stress, mitochondrial dysfunction, inflammation, and cell acidosis (Ou et al., 2021; Jin et al., 2022; Shi et al., 2022; Xie et al., 2022; Chang et al., 2019). During the chronic phase, the necrotic myocardium is gradually replaced by fibrotic scar tissue, leading to chronic myocardial infarction (MI) characterized by irreversible loss of viable myocardium, ventricular remodeling, and progressive cardiac dysfunction (Frantz et al., 2022). Thus, AMI, MIRI, and chronic MI represent a continuous pathological spectrum from acute ischemia and reperfusion-induced injury to chronic structural remodeling and heart failure progression (Frantz et al., 2022; Schäfer et al., 2022). Experimental and clinical evidence highlights that the pathophysiology of acute MIRI and chronic MI differs substantially, and these differences are critical for interpreting preclinical studies and designing therapeutic interventions (Buja, 2023). Despite significant advances in reperfusion therapy and conventional pharmacological management, there is still no effective treatment specifically targeting MIRI or MI. Therefore, developing novel therapeutic strategies that can protect the myocardium from acute MIRI and chronic MI.
Natural nutraceuticals are primarily derived from foods and are considered less toxic than synthetic derivatives. Numerous studies have shown that natural nutraceuticals such as resveratrol (RES), curcumin, and anthocyanins have physiological benefits and protective effects against chronic diseases, which has also driven a surge in the use of nutritional foods and dietary supplements worldwide in recent years (Zeng et al., 2023; Cai et al., 2020; Li et al., 2024). RES, 3-4′-5-trihydroxystilbene, is a plant polyphenol found in multiple foods, including grapes, berries, plums, and peanuts (Acipreste Hudson et al., 2022; Raj et al., 2014). It is easy to be absorbed orally and excreted in urine and feces after metabolism. Studies have found that RES has multiple pharmacological effects, including anti-inflammatory, antioxidant, anticancer, cardiovascular protection, and neuroprotective effects (Gál et al., 2023). The prevention and treatment of MIRI and MI by RES are related to its anti-oxidative stress effect (Goh et al., 2007; Ananthakrishnan et al., 2009; Xing et al., 2021; Mao et al., 2019; Teimouri et al., 2022; Xuan et al., 2012). RES protects myocardial cells from MIRI not only by inhibiting superoxide levels and activating potassium channels (Goh et al., 2007), but also by significantly reducing the generation of reactive oxygen species (ROS) and inhibiting the opening of mitochondrial permeability transition (MPT) pores in the mouse heart (Ananthakrishnan et al., 2009). In addition, recent studies have found that RES may have a protective effect on MIRI through anti-oxidative stress and anti-inflammation mechanisms by analyzing various signaling pathways and serum biochemical substances of experimental animals (Rodrigo et al., 2022).
Therefore, to assess the role of RES against MIRI and MI, reconcile inconsistencies in preclinical findings, and advance its clinical translation potential, this study aimed to evaluate the cardioprotective effect of RES against MIRI and MI in animal studies.
Materials & Methods
This meta-analysis has been registered in PROSPERO with identifier CRD42022383786.
Search strategy
We searched PubMed, EMBASE, and Web of Science for relevant literature from inception to October 2025. The search strategy in PubMed was (“myocardial ischemia” OR “myocardial I/R” OR “myocardial I/R injury” OR “myocardial ischemia-reperfusion injury” OR “myocardial ischemia-reperfusion” OR “myocardial infarction”) AND (“resveratrol”). Additionally, the keyword above was used to modify the search strategy in EMBASE and Web of Science. This section was conducted by Yi-Fan Zeng and Qi-Hao Guo. The difference was resolved by Wen-Jing Zeng.
Inclusion criteria
Inclusion criteria included: (1) Experimental models: blocking the left anterior descending (LAD) coronary artery, cardioplegia, or intravenously injecting vasoconstrictor, such as isoprenaline (ISO); (2) Treatment: RES was the only intervention compared with a control group, and (3) Data: detailed record the data on myocardial infarction size (IS) and/or other outcomes.
Exclusion criteria
Exclusion criteria included: (1) abstracts or meeting posters, (2) review, (3) meta-analysis articles, (4) case report, (5) repeated literature, (6) no detailed data, (7) no animal model, and (8) without a control group.
Data extraction
Two authors (Shi-Jie Wei, Xin-Yu Wei) independently screened eligible articles according to inclusion and exclusion criteria and extracted data using a standardized data extraction form. The authors then compared the results and resolved any differences after group discussion. The referee was Wen-Jing Zeng. Information extracted includes the authors, publication year, country, characteristics of the animal, sex of the animal, sample size, methods of anesthetic, model method, drug delivery method, and duration of the drug.
Primary outcomes include IS, dP/dT max, left ventricular ejection fraction (LVEF), left ventricular developed pressure (LVDP), and left ventricular fractional shortening (LVFS). Secondary outcomes included aortic flow (AF), coronary flow (CF), cardiac troponin T (cTnT), creatine kinase (CK), creatine kinase-MB (CK-MB), lactate dehydrogenase (LDH), tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), superoxide dismutase (SOD), malondialdehyde (MDA), and apoptosis rate. Engauge Digitizer was used to extract data from the figures in the included research.
Quality assessment
Two authors independently assessed the quality of included studies using SYRCLE’s RoB tool, which consists of ten categories (Hooijmans et al., 2014).
Statistical analysis
The standard mean difference (SMD) was used to calculate the summary statistics and 95% confidence interval (CI) of RES in the primary and secondary outcomes. I^2^ statistics were used for the heterogeneity assessment. Generally, heterogeneity was divided into low (0–25%), moderate (25%–75%), and high (>75%) by I^2^ value. Subgroup analysis was conducted to probe the source of the heterogeneity. When more than eight studies were conducted publication bias analysis by sensitive analysis, funnel plot, Begg’s test, and Egger’s test. Univariate meta-regression was conducted to explore the heterogeneity of IS in MIRI model. The dosage-efficacy analysis was plotted by GraphPad Prism 10.2.0. R (Version 4.2.2) software and its packages ‘meta’ and ‘metafor’ were used to conduct all the analysis above. P < 0.05 was considered statistically significant.
Results
Studies selection
Figure 1 showed the flow diagram. A total of 1,508 studies were involved in initial searching in PubMed (n = 247), Web of Science (n = 616), and EMBASE (n = 645). Duplicate articles (n = 431) were removed by EndNote. After reading the title and abstract, 238 articles were selected. Subsequently, 181 studies were excluded when screening the full text. Ultimately, this meta-analysis included 57 studies with 1,125 animals (Xuan et al., 2012; Adam et al., 2013; Ahmet et al., 2016; Boshra, 2020; Bradamante et al., 2003; Burstein et al., 2007; Cong et al., 2014; Das et al., 2005; Das et al., 2006; Dernek et al., 2004; Dong et al., 2015; Du et al., 2014; Feng et al., 2019; Gu et al., 2014; Hale & Kloner, 2001; He et al., 2021; Hung et al., 2000; Kaga et al., 2005; Kanamori et al., 2013; Kazemirad & Kazerani, 2020; Lamont et al., 2011; Lekli et al., 2010; Lekli et al., 2008; Li, Duan & Shen, 2022; Li et al., 2015; Li et al., 2024; Liao et al., 2015; Lin et al., 2008; Liu et al., 2022; Liu et al., 2019; Liu et al., 2023; Manjunatha et al., 2020; Matsumura et al., 2018; Mei, Liu & Sun, 2021; Mukhopadhyay et al., 2010; Naumenko et al., 2013; Penumathsa et al., 2007; Raj et al., 2016; Raj et al., 2021; Ray et al., 1999; Rogers & Otis, 2017; Salian et al., 2024; Sato, Maulik & Das, 2002; Shalwala et al., 2014; Shen et al., 2006; Shen et al., 2012; Singh et al., 2024; Soltan et al., 2021; Tanno et al., 2010; Thuc et al., 2012; Tian, Xiong & Xia, 2023; Xi et al., 2009a; Xin et al., 2010; Xu et al., 2022; Yang et al., 2016; Zhu et al., 2024; Hung, Su & Chen, 2004).
Flow diagram of database searches and study selection.
Characteristics of included studies
Of the included studies, 34 studies used Sprague-Dawley (SD) rats, eight studies used Wistar rats, one study used Zucker rats, one study used Long-Evans rats, one study used albino rats, seven studies used C57BL/6 mice, two study used Kun-Ming mice, one study used ICR mice, one study used To-2 hamster, and one study used New Zealand White rabbits. To build experimental animal models, 39 articles used MIRI by LAD ligation, ISO injection, or cardioplegia, and 18 articles used chronic MI by permanent LAD ligation. RES treatment was delivered by multiple routes, including perfused heart in 12 articles, oral administration in 25 articles, intraperitoneal injection in 14 articles, intravenous injection in four articles, subcutaneously embedded osmotic minipumps in one article, and injection surrounding the infarcted heart area in one article. The intervention duration varied between 5 min to 10 months. Studies were reported between 1999 and 2024. The details of the basic information about the trials included in the present meta-analysis were shown in Table 1.
Table 1: Baseline characteristics of included studies.
The methodological quality scores of the included literature ranged from 4 to 7 (Table 2). The potential molecular mechanism of cardioprotective effect of RES from MIRI and MI was summarized in Table 3.
Table 2: Quality assessment of included studies.
Table 3: The molecular and cellular mechanisms underlying the cardio-protection effect of resveratrol treatment in MIRI and MI.
Infarct size
The meta-analysis of IS in animal models of MIRI included 32 publications with 582 animals (Adam et al., 2013; Cong et al., 2014; Das et al., 2005; Das et al., 2006; Dong et al., 2015; Du et al., 2014; Feng et al., 2019; Hale & Kloner, 2001; Hung et al., 2000; Kazemirad & Kazerani, 2020; Lamont et al., 2011; Lekli et al., 2010; Lekli et al., 2008; Li, Duan & Shen, 2022; Li et al., 2015; Li et al., 2024; Liao et al., 2015; Liu et al., 2023; Mukhopadhyay et al., 2010; Naumenko et al., 2013; Penumathsa et al., 2007; Ray et al., 1999; Sato, Maulik & Das, 2002; Shalwala et al., 2014; Shen et al., 2006; Singh et al., 2024; Soltan et al., 2021; Thuc et al., 2012; Tian, Xiong & Xia, 2023; Xi et al., 2009a; Xu et al., 2022; Yang et al., 2016). RES supplementation was correlated with a decline of IS (SMD: −5.44; 95% CI [−6.42 to −4.45]; P < 0.01; I^2^ = 86%; Fig. 2A). Subgroup analysis based on country, IS measure methods, ischemia time, and duration did not show significant differences in heterogeneity between groups (Table 4). However, the drug delivery methods, reperfusion time of RES, and species showed a significant difference between subgroups. RES delivery by perfusion and intravenous, ISO method, and the mice group showed a decrease of heterogeneity within subgroups (Table 4). Sensitivity analysis revealed that our result was stable (Fig. S1A). The funnel plot was asymmetry, Begg’s test (P < 0.01), and Egger’s test (P < 0.01) of MIRI models showed the existence of publication bias (Fig. S1C).
Moreover, 10 researches (168 animals) were included in the analysis of IS in the animal model of MI (Xuan et al., 2012; Ahmet et al., 2016; He et al., 2021; Kaga et al., 2005; Kanamori et al., 2013; Lin et al., 2008; Raj et al., 2021; Rogers & Otis, 2017; Xin et al., 2010; Zhu et al., 2024). The RES treatment decreased IS (SMD: −3.41; 95% CI [−4.44 to −2.38]; P < 0.01; I^2^ = 75%; Fig. 2B). Subgroup analysis of species and drug delivery did not reveal significant differences in heterogeneity between groups (Table 5). In the subgroup of dose, the group of 1–5 mg/kg and >5 mg/kg presented a decrease in heterogeneity within subgroups. Besides, the group of >5 mg/kg was the lowest SMD, which means that the dose >5 mg/kg may have a better therapeutic effect in the animal model of MI. Sensitivity analysis revealed that our result was stable (Fig. S1B). The funnel plot was symmetry, Begg’s test (P = 0.10) and Egger’s test (P = 0.06) of MI models showed the absence of publication bias (Fig. S1D).
Forest plot showing cardioprotective effects of resveratrol on infarction size in animal models of MIRI (A) and MI (B).MIRI, myocardial ischemia/reperfusion injury; MI, myocardial infarction. (Xuan et al., 2012; Adam et al., 2013; Ahmet et al., 2016; Boshra, 2020; Bradamante et al., 2003; Burstein et al., 2007; Cong et al., 2014; Das et al., 2005; Das et al., 2006; Dernek et al., 2004; Dong et al., 2015; Du et al., 2014; Feng et al., 2019; Gu et al., 2014; Hale & Kloner, 2001; He et al., 2021; Hung et al., 2000; Kaga et al., 2005; Kanamori et al., 2013; Kazemirad & Kazerani, 2020; Lamont et al., 2011; Lekli et al., 2010; Lekli et al., 2008; Li, Duan & Shen, 2022; Li et al., 2015; Li et al., 2024; Liao et al., 2015; Lin et al., 2008; Liu et al., 2022; Liu et al., 2019; Liu et al., 2023; Manjunatha et al., 2020; Matsumura et al., 2018; Mei, Liu & Sun, 2021; Mukhopadhyay et al., 2010; Naumenko et al., 2013; Penumathsa et al., 2007; Raj et al., 2016; Raj et al., 2021; Ray et al., 1999; Rogers & Otis, 2017; Salian et al., 2024; Sato, Maulik & Das, 2002; Shalwala et al., 2014; Shen et al., 2006; Shen et al., 2012; Singh et al., 2024; Soltan et al., 2021; Tanno et al., 2010; Thuc et al., 2012; Tian, Xiong & Xia, 2023; Xi et al., 2009a; Xin et al., 2010; Xu et al., 2022; Yang et al., 2016; Zhu et al., 2024; Hung, Su & Chen, 2004).
Table 4: Subgroup analysis of pooled estimates of infarct size in MIRI models of MIRI.
Table 5: Subgroup analysis of pooled estimates of infarct size in animal models of MI.
Cardiac function
Due to the different research designs of MIRI and MI, different indicators of cardiac function were generally used. LVFS, LVEF, LVDP, dP/dT max, AF, and CF were used as indicators in animal models of MIRI. On the contrary, LVEF and LVFS were used as indicators in animal models of MI.
In animal models of MIRI, the following studies were included for cardiac function analysis: two studies (28 animals) for LVFS and LVEF (Liu et al., 2023; Tian, Xiong & Xia, 2023), nine studies (209 animals) for LVDP (Adam et al., 2013; Das et al., 2005; Das et al., 2006; Kazemirad & Kazerani, 2020; Lamont et al., 2011; Lekli et al., 2010; Lekli et al., 2008; Mukhopadhyay et al., 2010; Thuc et al., 2012), nine studies (124 animals) for dP/dt max (Das et al., 2005; Das et al., 2006; Dernek et al., 2004; Kazemirad & Kazerani, 2020; Lekli et al., 2010; Mukhopadhyay et al., 2010; Penumathsa et al., 2007; Ray et al., 1999; Shen et al., 2006), nine studies (217 animals) for CF (Adam et al., 2013; Bradamante et al., 2003; Das et al., 2005; Das et al., 2006; Dernek et al., 2004; Lamont et al., 2011; Lekli et al., 2010; Lekli et al., 2008; Ray et al., 1999), and six studies (72 animals) for AF (Das et al., 2005; Das et al., 2006; Lekli et al., 2010; Lekli et al., 2008; Mukhopadhyay et al., 2010; Ray et al., 1999). Notably, the LVFS result was derived from two studies, which should be interpreted as exploratory. The results showed that RES treatment significant increase LVFS (SMD: 4.48, P < 0.01, I^2^ = 51%; Fig. 3A), LVEF (SMD: 3.58, P < 0.01, I^2^ = 47%; Fig. 3B), LVDP (SMD: 4.73, P < 0.01, I^2^ = 92%; Fig. 3C), dP/dt max (SMD: 6.33, P < 0.01, I^2^ = 86%; Fig. 3D), CF (SMD: 2.18, P = 0.03, I^2^ = 88%; Fig. 3E), AF (SMD: 4.26, P < 0.01, I^2^ = 16%; Fig. 3F) in animals models of MIRI. The sensitivity analysis of LVDP (Fig. S2A), CF (Fig. S2B), and dP/dt max (Fig. S2C) indicated that our results were stable. The result of the funnel plot, Begg’s test, and Egger’s test in LVDP (Fig. S2D) and CF (Fig. S2E) showed the absence of publication bias. However, publication bias was included in the analysis of dP/dt max (Fig. S2F).
The pooled estimate of LVFS (A), LVEF (B), LVDP (C), dP/dt max (D), CF (E), and AF (F) in MIRI animal model.LVFS, left ventricular fractional shortening; LVEF, left ventricular ejection fraction; LVDP, left ventricular developing pressure; dP/dT max, maximum 1st derivative of developed pressure; AF, aortic flow; CF, coronary flow; MIRI, myocardial ischemia/reperfusion injury. (Liu et al., 2023; Tian, Xiong & Xia, 2023; Adam et al., 2013; Das et al., 2005; Das et al., 2006; Kazemirad & Kazerani, 2020; Lamont et al., 2011; Lekli et al., 2008; Thuc et al., 2012; Mukhopadhyay et al., 2010; Dernek et al., 2004; Lekli et al., 2010; Penumathsa et al., 2007; Ray et al., 1999; Shen et al., 2006; Bradamante et al., 2003).
In the animal model of MI, the pooled estimate of LVEF was 3.72 (P < 0.01; I^2^ = 78%). One study was excluded after the sensitivity analysis of LVEF (Fig. 4A) (Kanamori et al., 2013). Finally, nine studies (163 animals) were included in the meta-analysis of LVEF (Ahmet et al., 2016; Gu et al., 2014; Liu et al., 2019; Matsumura et al., 2018; Mei, Liu & Sun, 2021; Raj et al., 2016; Raj et al., 2021; Tanno et al., 2010; Zhu et al., 2024). The adjusted pooled estimate of LVEF was 2.98 (P < 0.01, I^2^ = 41%; Fig. 4B). Sensitivity analysis after adjustment showed that the result was stable (Fig. 4C). The funnel plot was symmetry, Begg’s test (P = 0.10) and Egger’s test (P = 0.07) revealed no publication bias (Fig. 4D). Moreover, seven studies (175 animals) were included in the meta-analysis of LVFS (Xuan et al., 2012; Lin et al., 2008; Liu et al., 2019; Mei, Liu & Sun, 2021; Tanno et al., 2010; Zhu et al., 2024). The pooled estimate of LVFS was 3.21 (P < 0.01, I^2^ = 71%; Fig. 4E) in the animal model of MI.
(A) Sensitivity analysis of LVEF in animal models of MI before adjustment.(B) The pooled estimate of LVEF in MI animal model. (C) Sensitivity analysis of LVEF in animal model of MI after adjustment. (D) Funnel plot, Begg’s test, and Egger’s test of LVEF in animal model of MI. LVEF, left ventricular ejection fraction; MI, myocardial infarction. (Ahmet et al., 2016; Gu et al., 2014; Liu et al., 2019; Matsumura et al., 2018; Mei, Liu & Sun, 2021; Raj et al., 2016; Raj et al., 2021; Tanno et al., 2010; Burstein et al., 2007; Lin et al., 2008; Xuan et al., 2012; Zhu et al., 2024).
Cardiac injury enzyme
After systematic data extraction from included studies, not enough data on cardiac injury enzymes were found in the MI model. Therefore, only the MIRI model was analyzed in this section. Serum biomarkers of myocardial injury, including LDH (13 studies, 210 animals) (Boshra, 2020; Cong et al., 2014; Dernek et al., 2004; Du et al., 2014; Feng et al., 2019; Hung et al., 2000; Kazemirad & Kazerani, 2020; Liao et al., 2015; Liu et al., 2023; Shen et al., 2012; Singh et al., 2024; Tian, Xiong & Xia, 2023; Hung, Su & Chen, 2004), CK-MB (11 studies, 180 animals) (Boshra, 2020; Dernek et al., 2004; Dong et al., 2015; Feng et al., 2019; Kazemirad & Kazerani, 2020; Liu et al., 2023; Manjunatha et al., 2020; Salian et al., 2024; Singh et al., 2024; Tian, Xiong & Xia, 2023; Xu et al., 2022), CK (three studies, 48 animals) (Cong et al., 2014; Liao et al., 2015; Hung, Su & Chen, 2004), and cTnT (three studies, 60 animals) (Boshra, 2020; Dernek et al., 2004; Dong et al., 2015) were analyzed.
The results revealed that RES treatment significantly reduced serum LDH (SMD: −9.52, P < 0.01, I^2^ = 85%), CK-MB (SMD: −10.96, P < 0.01, I^2^ = 90%), CK (SMD: −5.24, P = 0.01, I^2^ = 88%), and cTnT (SMD: −20.44, P = 0.02, I^2^ = 89%) in animal models of MIRI (Table 6 & Fig. S3). The sensitivity analysis in LDH and CK-MB revealed that the result was stable (Figs. S4A–S4B). The funnel plot of LDH and CK-MB was asymmetry with Begg’s test and Egger’s test, which suggested publication bias (Figs. S4C–S4D).
Table 6: The pooled estimate of cardiac injury enzyme and oxidative stress levels in MIRI and MI animal model.
Oxidative stress levels
To determine the oxidative stress levels of the heart after RES treatment, SOD and MDA were selected as indicators for analysis.
In the MIRI models, six researches (108 animals) reported heart SOD (Boshra, 2020; Feng et al., 2019; Kazemirad & Kazerani, 2020; Salian et al., 2024; Shen et al., 2012; Xu et al., 2022), and seven researches (126 animals) reported heart MDA (Boshra, 2020; Dernek et al., 2004; Feng et al., 2019; Kazemirad & Kazerani, 2020; Ray et al., 1999; Shen et al., 2006; Shen et al., 2012). The results demonstrated that RES treatment significantly increased heart SOD (SMD: 7.70, P < 0.01, I^2^ = 87%), and reduced heart MDA (SMD: −4.17, P < 0.01, I^2^ = 94%) (Table 6 & Fig. S5).
In the MI models, two studies (22 animals) reported heart SOD (He et al., 2021; Xin et al., 2010), and three studies (34 animals) reported heart MDA (Liu et al., 2022; Ray et al., 1999; Xin et al., 2010). The results demonstrated that RES treatment significantly increased heart SOD (SMD: 4.30, P < 0.01, I^2^ = 0%), and reduced heart MDA (SMD: −6.89, P < 0.01, I^2^ = 0%) (Table 6 & Fig. S5). However, these findings are exploratory, as they were derived from a limited number of studies with small sample sizes, and should therefore be interpreted with caution.
Inflammatory cytokine levels and apoptosis rate
Due to low heterogeneity within serum IL-1β, serum TNF-α, and heart TNF-α, the animal model of MIRI and MI were analyzed together. RES treatment significantly reduced serum IL-1β (five studies, SMD = −8.66, P < 0.01, I^2^ = 73%, Fig. 5A) (Dong et al., 2015; Liu et al., 2022; Liu et al., 2019; Singh et al., 2024; Xin et al., 2010), serum TNF-α (four studies, SMD = −3.71, P < 0.01, I^2^ = 0%, Fig. 5B) (Cong et al., 2014; Li et al., 2015; Liu et al., 2019; Singh et al., 2024), and cardiac TNF-α (three studies, SMD = −3.61, P < 0.01, I^2^ = 0%, Fig. 5C) (Cong et al., 2014; Li et al., 2015; Raj et al., 2021).
The pooled estimate of serum IL-1β.(A), serum TNF-α (B), and heart TNF-α (C) in MIRI and MI animal model. The pooled estimate of apoptosis rate in animal model of MIRI (D) and MI (E). Apoptosis results in MI models are based on only two studies with high heterogeneity and should be considered as exploratory. (F) Sensitivity analysis of apoptosis rate in animal model of MIRI. (G) Funnel plot, Begg’s test, and Egger’s test of apoptosis rate in animal model of MIRI. IL-1β, interleukin-1β; TNF-α, tumor necrosis factor-α; MIRI, myocardial ischemia/reperfusion injury; MI, myocardial infarction. (Dong et al., 2015; Liu et al., 2022; Liu et al., 2019; Singh et al., 2024; Xin et al., 2010; Cong et al., 2014; Li et al., 2015; Raj et al., 2021; Das et al., 2005; Du et al., 2014; Feng et al., 2019; Li, Duan & Shen, 2022; Li et al., 2024; Mukhopadhyay et al., 2010; Sato, Maulik & Das, 2002; Yang et al., 2016; Rogers & Otis, 2017; He et al., 2021).
For apoptosis rate, nine studies (156 animals) in MIRI (Das et al., 2005; Du et al., 2014; Feng et al., 2019; Li, Duan & Shen, 2022; Li et al., 2015; Li et al., 2024; Mukhopadhyay et al., 2010; Sato, Maulik & Das, 2002; Yang et al., 2016), and two studies in MI (He et al., 2021; Rogers & Otis, 2017) models were included. RES treatment significantly decreased the apoptosis rate in both MIRI (SMD: −6.33, P < 0.01, I^2^ = 78%, Fig. 5D) and MI (SMD: −7.72, P < 0.01, I^2^ = 60%, Fig. 5E) models. Because of high heterogeneity (I^2^ = 60%) and the limited number of MI studies (n = 2), these results should be regarded as exploratory. The sensitivity analysis confirmed result stability (Fig. 5F). However, the funnel plot was asymmetry with Begg’s test (P = 0.048), and Egger’s test (P < 0.01), which indicated publication bias (Fig. 5G).
Meta-regression and dosage-efficacy analysis
To further explore the sources of heterogeneity of IS in the MIRI model, univariate meta-regression analysis was performed (Table 7). Model type, IS measure methods, ischemia and reperfusion time, and duration did not significantly influence the effect sizes of IS. The drug delivery method accounted for 28.81% of between-study heterogeneity, with perfusion showing the largest reduction in IS (β = −2.64, P = 0.02). Animal species also contributed substantially to heterogeneity (R^2^ = 31.64%), with rabbits showing a worse effect size reduction.
Table 7: Meta-regression of infarct size in MIRI animal models.
Due to the different administration methods, the dosage units of the drugs are inconsistent. Therefore, we conducted meta-regression and dosage-efficacy analysis on the oral and intraperitoneal RES dosage in MIRI and MI models. The results showed that the dose was not significantly associated with the overall effect size (β = −0.018, P = 0.69, Figs. 6A–6B) in MIRI models. Although, there is a certain correlation between the dose of RES and the therapeutic effect in the MI model (β = −0.049, P = 0.042, Figs. 6C–6D), a relatively low oral dose of RES appeared to produce comparable (10 mg/Kg in MIRI and 20 mg/Kg in MI models) therapeutic efficacy compared with higher doses in both MIRI and MI models. The meta-regression and dosage-efficacy analysis results further supporting no clear dose–response relationship between RES dosage and treatment efficacy of MIRI and MI.
Meta-regression and dosage-efficacy analysis of oral administration RES in treatment of MIRI (A–B) and MI (C–D) animal models.
Discussion
Summary of evidence
To investigate the role of RES in the fight against MI and MIRI, 57 articles with 1,125 animals were investigated in this meta-analysis. The results indicated that RES treatment lessened the IS, down-regulated serum biomarkers of myocardial injury (CK-MB and LDH), improved cardiac function parameters (LVEDP, dP/dt max, AF, and CF), increased heart SOD level, reduced heart MDA and serum inflammatory cytokines (IL-1β and TNF-α), and alleviated cardiomyocyte apoptosis in animal models of MI and MIRI. Moreover, sensitivity analysis indicated that the cardioprotective effect of RES was stable though with high heterogeneity. In summary, our results demonstrated that RES effectivity ameliorates MI and MIRI in pre-clinical animal studies.
Molecular mechanisms
RES is a natural polyphenol compound, which exerts pharmacological activities such as anti-cardiovascular disease and anti-tumor. Previous studies have found that in the rat MIRI model, RES reduces myocardial cell necrosis by anti-oxidative stress and anti-free radicals and plays a protective role in MIRI by regulating the NO pathway and promoting NO release (Hung et al., 2002). In addition, RES also influences the occurrence and progression of tumors by regulating and controlling signal transduction pathways such as cell division and growth, apoptosis, inflammation, angiogenesis, and metastasis (Jang, Im & Kim, 2022).
Anti-oxidative stress effects
Oxidative stress plays an important role in MIRI (Bugger & Pfeil, 2020). Previous studies indicated that in the rat model of MIRI, the mitochondrial function of myocardial cells is seriously damaged, and the production of ROS is abnormally increased, leading to the increase of MI area. RES is a kind of antioxidant found naturally in plants. It functions as an antioxidant primarily by decreasing the production of free radicals and lipid peroxidation, and activating the enzymes and other pathways involved in antioxidant defense (Muñoz Bernal et al., 2021). SIRT1, a versatile protein deacetylase, was reported to be down-regulated in the hypoxic-reoxygenation (H/R) injury of cardiomyocytes (Guo et al., 2016). RES protects cardiomyocytes from H_2_O_2_-induced oxidative stress by activating SIRT1 and mitochondrial biogenesis signaling pathways (Li et al., 2013). DJ-1 participates in the regulation of oxidative stress by maintaining the activity of mitochondrial complex I. RES protects H9c2 cardiomyocytes from H/R-induced oxidative stress damage through increased expression of DJ-1, mitochondrial translocation, and the active mitochondrial complex I (Li et al., 2013). RES has been shown to reduce LPS-induced myocardial cell damage by inhibiting nuclear factor erythroid 2-related factor 2 (Nrf2), which could induce endogenous antioxidant enzymes against oxidative stress (Hao et al., 2013). RES preconditioning also significantly improved mitochondrial function and enhanced the activities of antioxidant enzymes SOD and GSH-PX by activating NRF2/ARE signaling pathways to alleviate cardiomyocyte damage (Spanier et al., 2009; Cheng et al., 2015). Especially, myocardial Nrf2 signaling is impaired in diabetic rats, leading to further deterioration of MIRI, and RES preconditioning can relieve MIRI by increasing Nrf2 expression and reducing oxidative stress index in diabetic rats (Xu et al., 2019a). In addition, RES was shown to significantly reduce ROS generation and MPT pore opening in ATG mice hearts to protect cardiomyocytes from MIRI (Ananthakrishnan et al., 2009). In SD rats, chronic myocardial ischemia reduced the protein expression of KLF15, and daily treatment with RES stimulates the expression of the KLF15 gene, which improves cardiac function and enhances cardiac remodeling and facilitates the regulation of redox homeostasis (Rogers & Otis, 2017).
Anti-inflammation effects
The inflammatory response is an important pathophysiological mechanism of MIRI injury (Schäfer et al., 2022). In animal models of MIRI, the levels of inflammatory cytokines were significantly increased, and early RES treatment effectively reduced MIRI by inhibiting the inflammatory response (Buja, 2023). RES preconditioning attenuates serum and myocardial TNF-α production, IS, and myocardial apoptosis in MIRI rats by inhibiting Toll-like receptor 4 (TLR4)/NF-κB signaling pathway (Li et al., 2015). In addition, the cardioprotective effect of RES on MIRI animal models also involves inhibition of the NLRP3 inflammasome pathway (Dong et al., 2015), and activation of the Nrf2/ARE pathway (Hao et al., 2013; Cheng et al., 2015).
Anti-apoptosis effects
Apoptosis induced by MIRI is an important way to lead to myocardial cell death. RES exhibits an anti-apoptotic effect on H/R damage of H9c2 cells, and the specific mechanism is related to restoring SIRT1 activity in a DJ-1-dependent manner, thus reducing the level of p53 acetylation (Xu et al., 2019c). Voltage-dependent anion channel 1 (VDAC1), a protein located in the mitochondrial outer membrane, was downregulated in cardiomyocytes’ H/R injury (Liao et al., 2015). RES was proven to inhibit mitochondria-mediated myocardial apoptosis by deacetylating VDAC1 and increasing VDAC1 protein expression in the H/R cell model (Tong et al., 2017). In MIRI rats, RES treatment prior to the onset of reperfusion significantly improved cardiac systolic function and reduced IS. The specific mechanism is that RES transferred GSK-3beta from the cytoplasm to mitochondria via the cGMP/PKG pathway, and finally interacted with cyclophilin D to regulate MPT pore opening, thereby alleviating reperfusion myocardial injury (Xi et al., 2009b).
Other mechanisms
Increased intracellular free Ca^2+^ plays a crucial role in MIRI. In H9c2 cells, RES preconditioning not only inhibited intracellular calcium aggregation by up-regulating sarcoplasmic reticulum stress protein Grp94 to reduce H/R-induced cell necrosis (Vitadello et al., 2003), but also alleviated H/R-induced calcium overload by inhibiting STIM1, thus inhibiting cardiomyocyte apoptosis and promoting cardiac function recovery after MIRI (Xu et al., 2019b). Moreover, RES can also induce autophagy by activating the mammalian target of the rapamycin complex 2 (mTORC2) pathway, thus protecting cardiomyocytes against H/R injury (Gurusamy et al., 2010).
Implications
Many pharmacological agents have been shown to reduce MIRI in animal models, however, no cardioprotective agent has been routinely used for the treatment of clinical MIRI up to date (Zheng et al., 2017). Among various theories, the features of the pathophysiology of MIRI include vascular leakage, oxidative stress, the loss of energy substrates, leukocyte entrapment, inflammation, apoptosis, and mitochondrial dysfunction (Yang et al., 2019; Liu et al., 2017). RES exerts pharmacological properties including antioxidant, anti-inflammatory, and immuno-modulatory functions (Pannu & Bhatnagar, 2019). The findings of the present study suggested that RES can significantly reduce the IS in MIRI animal models, down-regulate serum CK-MB and LDH, improve cardiac function parameters, reduce inflammatory cytokines, and cardiomyocyte apoptosis rate.
Our meta-regression and dose-efficacy analysis suggest that RES can exert cardioprotective effects even at relatively low doses. The observation of efficacy at lower doses has important translational implications, as it may reduce the risk of potential off-target effects or toxicity associated with higher doses. However, the absorption and metabolism of RES is influenced by age, gut microbiota composition, diet, and co-administered medications, which are rarely considered in preclinical studies but are critical in clinical settings (Silva et al., 2023; McGonigle & Ruggeri, 2014). Therefore, it is important to note that the dose-efficacy relationship observed in animal studies may not directly extrapolate to humans due to differences in pharmacokinetics, bioavailability, and metabolism (Van der Worp et al., 2010). In addition, RES rapidly undergoes glucuronidation and sulfation in the intestine and liver, resulting in low systemic concentrations of the parent compound and significant differences in plasma levels of its metabolites (Yu, Jia & Ren, 2024; De Vries, Strydom & Steenkamp, 2021). The oral bioavailability of RES is low, and its widespread first pass metabolic elimination may severely limit its clinical application. To overcome these limitations, several strategies can be further explored: novel drug delivery systems (e.g., nanoparticles, liposomes), prodrugs or derivatives with improved pharmacokinetics, and co-administration with bioenhancers such as piperine or quercetin to inhibit metabolic enzymes (De Vries, Strydom & Steenkamp, 2021).
In addition to its independent cardioprotective effects, RES may serve as a complementary therapy alongside established interventions such as β-blockers, ACE inhibitors, statins, and reperfusion strategies (Gal et al., 2021). Therefore, combining RES with standard treatments could potentially yield additive or synergistic cardioprotective effects, particularly in complex pathophysiological settings like MIRI or MI. Future studies should explore these combination strategies in clinically relevant models, including animals with comorbidities, to better inform translational potential and guide eventual clinical evaluation.
Limitation
At first, the potential for publication bias cannot be ignored. Positive results within animal studies are more likely to be published, whereas negative findings may remain unpublished (Mlinarić, Horvat & Šupak Smolčić, 2017), leading to an overestimation of the cardioprotective effects of RES. This is supported by the observed asymmetry in funnel plots and statistically significant Egger’s and Begg’s tests, indicating that studies reporting substantial effects are overrepresented. While we attempted to address this by performing sensitivity, subgroup, and meta-regression analysis, residual bias may still influence the pooled estimates. Therefore, the efficacy of RES observed in this meta-analysis should be interpreted cautiously, and further well-designed studies, including those reporting null results, are needed to validate these effects.
Secondly, substantial heterogeneity across the majority of pooled analysis (I^2^ > 75%) was observed. High heterogeneity indicates that between-study differences account for most of the observed variability. In this case, the heterogeneity may come from multiple sources, including differences in animal species and strains, model type, RES dose, route and duration of administration, outcome definitions, sampling time points for enzyme and oxidative stress measurements, and methodological quality. Statistically, high I^2^ reduces the confidence one can place in a single pooled estimate and limits generalizability, therefore, we used random-effects models and report prediction intervals to convey the range of effects likely to be observed in new studies. We also performed subgroup analysis, leave-one-out sensitivity analysis, meta-regression, and dosage-efficacy analysis. While some moderators partially explained the heterogeneity, substantial residual heterogeneity remained. Therefore, although the overall direction of effect was consistent across analyses, the magnitude of pooled effects should be interpreted cautiously. Future preclinical studies should standardize key experimental parameters to reduce heterogeneity and strengthen translational inference.
Thirdly, it is important to note that many included studies exhibited methodological limitations, particularly in blinding and randomization. The absence of random allocation and blinded outcome assessment may lead to selection bias and observer bias, potentially exaggerating the apparent cardioprotective effects of RES. These biases could affect both the effect size estimates and the interpretation of heterogeneity. Future preclinical studies should rigorously implement randomization, allocation concealment, and blinding to improve the reliability and translational relevance of findings.
Finally, due to convenience and widely used of rodent models, the majority of included studies were conducted in young, healthy small rodents without other comorbidities. Large-animal models, such as pigs, can better replicate the cardiovascular anatomy, physiology, and pharmacokinetics of humans. Besides, MIRI or MI patients have more complex cardiovascular comorbidities, age-related physiological changes, and potential drug interactions, which may influence treatment responses in clinical practice. Therefore, although our meta-analysis suggested that RES has cardioprotective effects in animal models, these findings may not fully reflect the complex pathophysiology and treatment response of human patients. It is necessary to conduct preclinical studies using comorbidity- and large-animal models under ARRIVE (Percie du Sert et al., 2020), IMPACT (Lecour et al., 2021), and CAESAR (Fernández-Jiménez & Ibanez, 2015) guidelines in the future to validate the cardioprotective effects of RES and improve its clinical applicability.
Conclusions
Our findings suggest that RES appears to confer cardioprotective effects in animal models of MIRI and MI, including reduction of IS and serum cardiac enzymes, and improvement of cardiac function. However, the translational potential of RES remains uncertain, and additional preclinical studies with standardized protocols, comorbid models, and eventual clinical trials are needed to confirm these results.
Supplemental Information
10.7717/peerj.20708/supp-1Supplemental Information 1Sensitivity analysis of infarction size in animal model of MIRI (A) and MI (B). Funnel plot, Begg’s test, and Egger’s test of infarction size in animal model of MIRI (C) and MI (D)MIRI, myocardial ischemia/reperfusion injury; MI, myocardial infarction.
10.7717/peerj.20708/supp-2Supplemental Information 2Sensitivity analysis of LVDP (A), dP/dt max (B), and CF (C) in animal model of MIRI. Funnel plot, Begg’s test, and Egger’s test of LVDP (D), dP/dt max (E), and CF (F) in animal model of MIRILVDP, left ventricular developing pressure; dP/dT max, maximum 1st derivative of developed pressure; CF, coronary flow; MIRI, myocardial ischemia/reperfusion injury.
10.7717/peerj.20708/supp-3Supplemental Information 3The pooled estimate of LDH (A), CK-MB (B), CK (C), and cTnT (D) in MIRI animal modelLDH, lactate dehydrogenase; CK-MB, creatine kinase isoenzyme; CK, creatine kinase; cTnT, cardiac troponin T; MIRI, myocardial ischemia/reperfusion injury.
10.7717/peerj.20708/supp-4Supplemental Information 4Sensitivity analysis of LDH (A) and CK-MB in animal model of MIRI. Funnel plot, Begg’s test, and Egger’s test of LDH (C) and CK-MB (D) in animal model of MIRILDH, lactate dehydrogenase; CK-MB, creatine kinase isoenzyme; MIRI, myocardial ischemia/reperfusion injury.
10.7717/peerj.20708/supp-5Supplemental Information 5The pooled estimate of heart SOD (A) and MDA (B) in MIRI animal model. The pooled estimate of heart SOD (C) and MDA (D) in MI animal modelSOD, superoxide dismutase; MDA, malondialdehyde; MIRI, myocardial ischemia/reperfusion injury; MI, myocardial infarction.
10.7717/peerj.20708/supp-6Supplemental Information 6PRISMA checklist
10.7717/peerj.20708/supp-7Supplemental Information 7Raw Data of this meta-analysis
10.7717/peerj.20708/supp-8Supplemental Information 8The intended audience for this study
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acipreste Hudson E Campos de Paula HM Coelho YL Glanzmann N Da Silva AD Mendes da Silva LH Dos Santos Pires AC 2022 The kinetics of formation of resveratrol-β-cyclodextrin-NH(2) and resveratrol analog-β-cyclodextrin-NH(2) supramolecular complexes Food Chemistry 36613061210.1016/j.foodchem.2021.13061234311236 · doi ↗ · pubmed ↗
- 2Adam T Sharp S Opie LH Lecour S 2013 Loss of cardioprotection with ischemic preconditioning in aging hearts: role of sirtuin 1?Journal of Cardiovascular Pharmacology and Therapeutics 181465310.1177/107424841245872322960148 · doi ↗ · pubmed ↗
- 3Ahmet I Tae HJ Lakatta EG Talan M 2016 Long-term low dose dietary resveratrol supplement reduces cardiovascular structural and functional deterioration in chronic heart failure in rats Canadian Journal of Physiology and Pharmacology 95326827410.1139/cjpp-2016-051228134561 PMC 10542918 · doi ↗ · pubmed ↗
- 4Ananthakrishnan R Kaneko M Hwang YC Quadri N Gomez T Li Q Caspersen C Ramasamy R 2009 Aldose reductase mediates myocardial ischemia-reperfusion injury in part by opening mitochondrial permeability transition pore American Journal of Physiology-Heart and Circulatory Physiology 2962 H 333H 34110.1152/ajpheart.01012.200819060123 PMC 2643894 · doi ↗ · pubmed ↗
- 5Boshra SA 2020 Resveratrol modulates mi R-34a in cardiotoxicity induced by isoproterenol Journal of Medicinal Food 23659359910.1089/jmf.2019.020931794687 · doi ↗ · pubmed ↗
- 6Bradamante S Barenghi L Piccinini F Bertelli AA De Jonge R Beemster P De Jong JW 2003 Resveratrol provides late-phase cardioprotection by means of a nitric oxide- and adenosine-mediated mechanism European Journal of Pharmacology 4651–211512310.1016/S 0014-2999(03)01441-912650840 · doi ↗ · pubmed ↗
- 7Bugger H Pfeil K 2020 Mitochondrial ROS in myocardial ischemia reperfusion and remodeling Biochimica Et Biophysica Acta Molecular Basis of Disease 1866716576810.1016/j.bbadis.2020.16576832173461 · doi ↗ · pubmed ↗
- 8Buja LM 2023 Pathobiology of myocardial ischemia and reperfusion injury: models, modes, molecular mechanisms, modulation, and clinical applications Cardiology in Review 31525226410.1097/CRD.000000000000044035175958 PMC 10399947 · doi ↗ · pubmed ↗