Cardioprotective medications and the incidence of cardiovascular events in patients treated with radiotherapy: a systematic review and meta-analysis
Vishwa Pakeerathan, Ravi Marwah, Abdul Rahman Mohammed, Justin Smith

TL;DR
This study reviews how cardioprotective medications affect cardiovascular events in patients receiving radiotherapy, finding some benefits for stroke risk but limited evidence overall.
Contribution
The study provides a meta-analysis of cardioprotective medication use in radiotherapy patients, highlighting gaps in guideline adherence.
Findings
Statin therapy reduced cerebrovascular event risk in radiotherapy patients.
No significant effect of statins on major adverse cardiac events was found.
Many radiotherapy patients not on statins had indications for their use.
Abstract
The purpose of this systematic review and meta-analysis is to explore the utilization of cardioprotective medications in patients treated with RT and assess their impact on cardiovascular and cerebrovascular events. A literature search of PubMed, Embase and Scopus was performed in March 2025. Studies of adult patients treated with RT to the head and neck or thoracic regions which investigated the effects of cardioprotective medications (defined as anti-hypertensives, lipid-lowering therapies or anti-thrombotic medications) on the incidence of cardiovascular or cerebrovascular events were eligible for inclusion. Studies that reported the proportion of patients treated with RT who were utilizing cardioprotective medications as recommended by CVD guidelines were also included. Meta-analysis was performed using R with a random effects model. There were 10 retrospective studies which were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
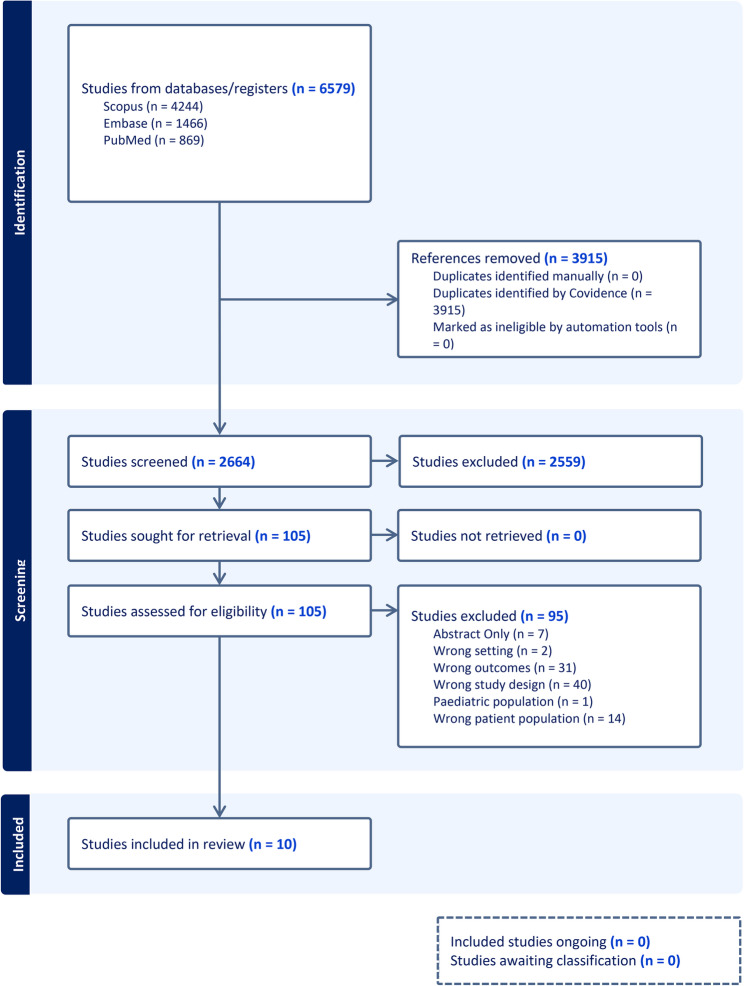 Figure 1
Figure 1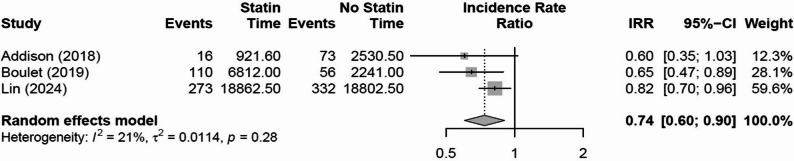 Figure 2
Figure 2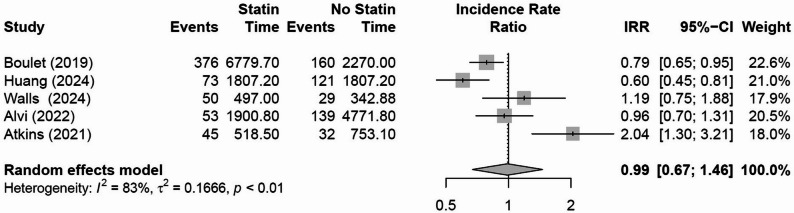 Figure 3
Figure 3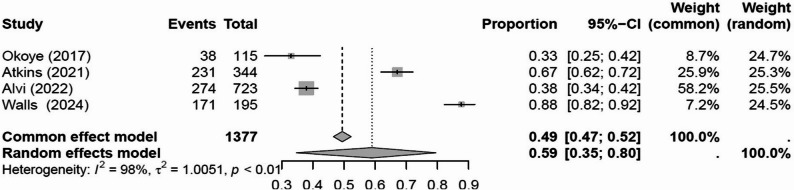 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-induced cardiotoxicity and mitigation · Effects of Radiation Exposure · Brain Metastases and Treatment
Introduction
Approximately 30–50% of all cancer patients require radiation therapy as part of their management [1]. However, radiotherapy increases the risk of cardiovascular and cerebrovascular disease (CVD) amongst cancer survivors [2], particularly those with head and neck cancer [3], lung cancer [4], and esophageal cancer [5]. Proposed pathogenic mechanisms include accelerated endothelial damage and atherosclerosis, as well as increased inflammation and fibrosis of myocardial, pericardial, valvular and conduction tissues [6].
While statin therapy has been associated with reduced all-cause mortality, cardiovascular death, and incidence of myocardial infarction in the general population [7, 8], the prescription of statins is primarily guided by traditional CVD risk stratification scores including the Framingham Risk Score [9]. Importantly, prior research suggests that patients treated with radiotherapy are at higher risk of CVD than indicated by these scores [10]. Therefore, there are concerns that cardioprotective medications including statins are being underutilized in this population with an increased CVD risk. Notably, a recent prospective study found that early cardio-oncology review in patients treated with high-dose thoracic radiotherapy resulted in a change in clinical management in more than 60% of patients, predominantly in the form of statin therapy initiation or intensification [11].
The aim of this review was to evaluate cardioprotective pharmacotherapies, including lipid-lowering therapy (statins), antihypertensives, and antithrombotic agents in patients treated with radiotherapy, and to assess their impacts on cardiovascular and cerebrovascular outcomes, as well as to quantify the uptake of cardioprotective medications in this group of patients.
Methods
This systematic review and meta-analysis was performed as per PRISMA guidelines.
Eligibility criteria
Studies that met the criteria below were included.
Inclusion criteria
- Included patients who have previously received external beam radiation therapy for cancer in the head and neck or thoracic regions (including mediastinum/breast/esophagus/lung cancers).
- Reports the incidence of cardiovascular events in a group that received radiotherapy and a group that did not, or the incidence of patients treated with RT who were prescribed cardioprotective medications.
- Cardiovascular events defined as ischemic stroke, transient ischemic attack (TIA) or myocardial infarction.
- Cardioprotective medications defined as anti-hypertensives, lipid lowering therapies or anti-thrombotic medications.
Exclusion criteria
- Studies with a pediatric patient population.
- Included patients with haematological malignancies.
- Pre-clinical studies.
Search strategy
A literature search was performed in March 2025 on PubMed, Scopus and Embase. The PubMed search strategy is demonstrated below, with appropriate adjustments made for Scopus and Embase (Supplementary 1). The databases were searched from inception to March 2025.
(“cancer” OR “malignancy” OR “carcinoma” OR “neoplasm” OR “tumour” OR “tumor”) AND (“radiation therapy” OR “radiotherapy” OR “irradiation”) AND (“statin” OR “lipid lowering” OR “cholesterol lowering” OR “antihypertensive” OR “anti-hypertensive” OR “blood pressure medication” OR “antithrombotic” OR “anti-thrombotic” OR “antiplatelet” OR “anti-platelet” OR “aspirin” OR “cardiovascular medication”).
Study selection process
Initial title and abstract screening were performed by the first author and relevant articles were identified for full text review. These manuscripts were then screened independently by two authors (VP and JS) to assess eligibility for inclusion.
Data extraction
One author (VP) extracted relevant data from included manuscripts. This data was checked for accuracy by a second author (RM). Extracted data included study methodology, sample size, study outcomes and participant characteristics.
Risk of bias assessment
Eligible studies were assessed using the Newcastle Ottawa for cohort studies. The checklist scored eight items as responses, ‘yes’, ‘no’ or ‘unclear’. A maximum score of nine indicated that all criteria were addressed in the study. This process was conducted independently by two authors (VP and RM).
Statistical analysis
A meta-analysis was performed if three or more studies reported the same outcome. Meta-analyses were conducted using R version 4.3.1 and a random effects model was used. Statistical significance was defined as p < 0.05 and study heterogeneity was assessed using I^2^ values. A meta-analysis of incidence rates was performed to compare the risk of cerebrovascular and cardiovascular events between the two groups (RT and control groups). Cerebrovascular events were defined as ischemic stroke alone, with TIA events excluded for the purposes of pooled meta-analysis. Major adverse cardiovascular events (MACE) were defined as a pooled measure of any cardiovascular (e.g. myocardial infarction, atrial fibrillation, heart failure) and cerebrovascular events (stroke or TIA). Person years were used to assess the follow-up time for each study. If a study did not report follow up in person years then this was estimated using median follow up time. If median follow up time was not reported for the two groups separately it was assumed to be the same follow up time in both groups. A meta-analysis of proportions was used to estimate the percentage of patients treated with RT who were not prescribed cardioprotective medications but had indications to commence them.
Results
Study selection
There were 2664 articles screened by title and abstract (Fig. 1). 105 articles were then screened in full text, and 10 studies were deemed to meet eligibility criteria. There were 95 studies excluded in the full text screening, with 40 because of wrong study design, 31 due to wrong outcomes and 15 had the incorrect patient population. Seven were abstract only and 2 were deemed to be in the wrong setting.
Fig. 1PRISMA flow diagram
Study characteristics
Study characteristics for the 10 included studies are summarized in Table 1. There was significant variability within the included studies, with varying patient populations, tumor subsites and outcome measures. There were five studies which included patients with head and neck cancer only [12–16], two studies reported outcomes in lung cancer alone [17, 18], whilst one study included patients with breast cancer [19], one with esophageal cancer [16] and one with patients receiving thoracic and/or head and neck RT [12–16, 20]. Although the eligibility criteria included lipid-lowering, antihypertensive, and antithrombotic therapies, the majority of eligible studies assessed statin exposure, with nine of the ten studies exploring statin therapy use during or after RT. Conversely, there were only three studies which explored the effectiveness of anti-thrombotic treatment (Table 2).
Table 1. Study characteristicsAuthor (Year)CountryStudy designPopulationSample sizeCardioprotective medicationStudy objectivesOutcome measuresEvents in cardioprotective groupEvents in non-cardioprotective groupMedian follow-Up Proportion of patients not receiving cardioprotective mediations with indications to commenceCommentsOkoye (2016) [21]USARetrospective cohortHNC 115Statins and anti-thrombotic (aspirin) To quantify baseline CVD risk and assess use of preventive cardioprotective medicationsProportion of eligible patients not prescribed cardioprotective medicationsN/AN/A2 years38/115 (33%) of patients not receiving statins as recommended by AHA guidelinesHsu (2016) [14]TaiwanRetrospective cohortHNC37,638Oral Anti-thrombotic Therapy (antiplatelet or anticoagulants) Use defined as at least one prescription within 30 days of RT start dateEvaluate efficacy and safety of oral anti-thrombotic therapy for primary stroke prevention in HNC patients after RT.Ischemic stroke or TIAOther - Death and major bleeding21 stroke/TIA(n = 815)600 stoke/TIA(n = 36,823)2.7 years (mean)NRAnti-thrombotics did not increase major bleeding risk Addison (2017) [12]USARetrospective cohortHNC1,011StatinsUse defined as statin utilization at the time of RT start dateDetermine whether statin use at time of RT lowers post-RT stroke/TIA riskIschemic stroke and TIA16 stroke and 1 TIA (n = 288)73 strokes and 12 TIA(n = 723)3.4 yearsNRStatin users had significantly lower risks of stroke/TIA post-RT (adjusted HR = 0.40, 95% CI 0.2–0.8, p = 0.01) Boulet (2019) [20]CanadaRetrospective cohortHNC & Thorax5,718StatinsUse defined as statin prescription 1 year before RT start to event or censureDetermine if post-RT statin use reduced vascular events (stroke, TIA, MI)MACE376 MACE110 strokes(n = 4166)160 MACE56 strokes(n = 1552)1.5 years (mean)NRMACE defined as MI, stroke or death caused by MI or stroke Atkins (2021) [17]USARetrospective cohortNSCLC748StatinsUse defined as statin utilization at RT consultation or priorAssess whether statin therapy predicts overall survival after RT (and impact on cardiac events)MACEProportion of eligible patients not prescribed cardioprotective medications45 MACE(n = 305)32 MACE(n = 443)1.7 years231/344 (67%) of patients not receiving statins had indications to commence as per Framingham riskMACE defined as cardiac death, unstable angina, myocardial infarction, heart failure hospitalization and coronary revascularization Alvi (2022) [13]USARetrospective cohortHNC723StatinsUse defined as statin utilization before or after RTEvaluate performance of cardiovascular risk models in predicting MACE post RTMACEProportion of eligible patients not prescribed cardioprotective medications53 MACE(n = 288)139 MACE(n = 723) 6.6 years274/723 (38%) of patients not prescribed statins had indications to commence as per USPSTF criteria and 32% based on Framingham riskMACE defined as myocardial infarction, coronary heart disease, stroke and cardiovascular deathWalls (2023) [18]United KingdomRetrospectivecohortNSCLC478StatinsUse defined as statin utilization at start of RT. Statin intensity graded as low, medium or high Impact of statins on cardiac events and survival as well as investigating impact of statin intensityMACEProportion of eligible patients not prescribed cardioprotective medications 50 MACE(n = 283)29 MACE(n = 195)1.8 years171/195 (88%) of patients not on statins had at least one guideline indication for statin therapyMACE defined as acute coronary syndrome, heart failure or arrhythmiaHigh intensity and medium intensity statin therapy associated with improved survivalHuang (2024) [19]TaiwanRetrospective cohortBreast cancer1,481StatinsUse defined as patients who utilized statins during or after RTDetermine if statin therapy reduces radiation-induced cardiotoxicity (MACE risk) after RT for breast cancerMACE73 MACE(n = 360)121 MACE(n = 360)5 yearsNRMACE defined as MI, acute coronary syndrome/ischemic heart disease, cerebrovascular accident, heart failure and cardiovascular deathPropensity score matching to balance cohortsA dose-response effect was observedLin (2024) [15]TaiwanRetrospective cohortHNC – Nasopharyngeal only5,022StatinsUse defined as patients who utilized statins during or after RTAssess impact of statin use on ischemic stroke risk in patients receiving RT for nasopharyngeal cancerIschemic stroke273 strokes(n = 2,515)332 strokes (n = 2,507)7.5 yearsNRStatin use during RT was associated with significantly lower stroke incidence (adjusted HR 0.70, 95% CI 0.54–0.92, p = 0.01).Dose–response trend was notedMiller (2024) [16]USARetrospective cohortEsophageal cancer238Baseline cardio-preventive medications (statins, aspirin, beta blockers)Use recorded at diagnosisInvestigate incidence of atrial fibrillation and cardiovascular events after esophageal RTAFMACE (AF, heart failure, ventricular arrythmia, sudden death)NRNR1.9 yearsNR21% of patients developed new AF and 33% had MACE after RT Higher left atrial radiation dose was strongly predictive of AF/MACEHNC Head and Neck Cancer, RT Radiotherapy, TIA Transient Ischemic Attack, MI Myocardial infarction, Non-Small Cell Lung Cancer, NR Not reported, AHA American Heart Association, USPSTF (US Preventative Services Task Force), AF Atrial Fibrillation
Cardioprotective medications and risk of cardiovascular and cerebrovascular events
Risk of cerebrovascular events
Meta-analysis of three studies suggested that patients treated with radiotherapy had a reduced risk of cerebrovascular events (stroke) with incidental statin use (IRR 0.74, 95% CI 0.60 to 0.90, p = 0.034, I^2^ = 21%, τ^2^ = 0.011, Fig. 2). There was variability in tumor sites between the studies, with the study by Adison et al.[12] including patients with all types of head and neck cancer, whilst the study by Lin et al.[15] included patients with nasopharyngeal cancer only. Conversely, the study by Boulet et al.[20] included patients with either head and neck cancer (12%) or cancers of the chest or thoracic region (88%).Fig. 2. Effect of statin treatments on cerebrovascular events
Cardiovascular events
There were five studies which investigated the effect of statin therapy on major adverse cardiovascular events (MACE) for patients receiving RT to the thorax. There was no evidence that cardioprotective medications reduced the incidence of MACE in patients treated with RT (IRR 0.99, 95% CI 0.67 to 1.46, p = 0.961, I^2^ = 82.6%, τ^2^ = 0.167, Fig. 3). One study could not be included in the meta-analysis as it did not report the event rates for a statin and non-statin group but performed a univariate analysis which demonstrated no association between statin use and MACE (HR 1.38, 95% CI 0.89 to 2.15, p= 0.15)[16]. There was significant heterogeneity in tumor sites with one study investigating patients with thoracic and head and neck cancers[20], one study investigating breast cancer[19], two studies investigating lung cancer [17, 18] and one study with patients with head and neck cancer [10]. Only one study included in the MACE meta-analysis [19] used statistical methods to account for baseline differences in demographics between the cardioprotective and no cardioprotective groups.
Fig. 3. Effect of statin treatments on major adverse cardiac events
Proportion of patients with indications for cardioprotective medications
A meta-analysis of four studies suggested that 59% (95% CI 35% to 80%, Fig. 4) of patients treated with RT not on statin therapy had established indications for commencement.Fig. 4. Proportion of patients not using statin treatments with indications to commence
Risk of bias assessment
All included studies were retrospective observational studies and were assessed using the Newcastle Ottawa Scale (Table 2). The quality of included studies was variable, with three studies scoring 9 out of 9 [14, 15, 19], whilst six studies were between 6 and 7 [12, 13, 16–18, 20]. One study was rated 3 out of 3 as it had no comparator group but was still eligible for inclusion as it reported the proportion of patients treated with RT who were not on statin therapy but had indications to commence them [21]. There were only 4 studies which followed patients up for greater than a median of 5 years [13–15, 19]. Only 3 studies used propensity score matching to balance the cohorts (cardioprotective medications compared to no medications) [14, 15, 19]. Table 2. Risk of bias assessmentAuthorAddison et al. [12]Alvi et al. [13]Atkins et al. [17]Boulet et al. [20]Hsu et al. [14]Huang et al. [19]Lin et al. [15]Miller et al. [16]Okoye et al. [21]Walls et al. [18]Year Published2017202220212019201620242024202420162023Selection1. Representativeness of exposed cohortRepresentative of the average patient receiving cardioprotective medications in the communityAll RT patients from one institution, somewhat representativeHead & Neck cancer patients from one centre, broadly representativePatients with locally advanced NSCLC treated with thoracic RT at a tertiary centre between 1998 and 2014Population-based provincial database of patients > 65 yrs who had prior cardiac evaluation and had been treated with RT for head and neck or thorax cancerNational wide Taiwanese cohort of HNC patients treated with RT between 1998 and 2008National wide Taiwanese cohort of left-sided breast cancer patients treated with RT from 2016–2019National wide Taiwanese cohort of NPC patients that underwent CCRT from 2012–2018Oesophageal cancer patients treated with RT from 2007–2019 at a single institution.HNC patients treated with curative RT from 2011–2013 at a university cancer centre; typical of tertiary care.Consecutive NSCLC patients treated with curative-intent radiotherapy between 2015–2020 at a single regional centre.2. Selection of non-exposed cohortDrawn from the same community as the exposed cohort?Controls were same hospital RT patients without statinsNon-statin group drawn from same institutional cohortNon-statin patients from same treated cohortNon-statin group from same Quebec cohortNon-Oral Antithrombotic Therapy users from same national cohortNon-statin patients from same national cancer registry databaseNon-statin group from same national NPC cohortPatients not taking cardioprotective medications in the same cohortN/ANon-statin group from same hospital population and timeframe3. Ascertainment of exposure (how was it recorded who had cardioprotective medications?)Statin use documented via EMR medication listStatin use, and eligibility determined from cohort and risk score criteriaStatin use at RT start confirmed from medication lists or prescriptions in medical recordStatin use from provincial pharmacy claimsAnti-thrombotic use obtained from insurance prescription records.Statin use obtained from National Health Insurance Research Database Pharmaceutical subsidiesStatin use identified via National Health Insurance Research Database Pharmaceutical subsidiesAll baseline characteristics including cardioprotective medication use collected via manual chart reviewCVD risk factors and medications obtained from medical records at diagnosisStatin therapy and dose intensity abstracted from clinical records. Medication use relied on documented prescriptions rather than self-report.4. Demonstration that outcome of interest was not present at start of study-Included patients with prior stroke/TIA ~ 6.9% had CVE at baseline-Patients with prior ASCVD were included - baseline CVD not excluded-No exclusion of baseline CVD events-No exclusion of baseline CVD eventsExcluded any patient with prior stroke/TIA before RTExcluded any prior MACE or cardiac event before RTExcluded patients with any prior stroke, carotid disease, or metastasis before RTExcluded patients with any prior atrial fibrillation; “incident AF” defined as new-onset post-RTN/A-There was no exclusion of baseline CVD events, so prevalent disease could have influenced outcomes.Comparability1. Study cohorts are similar in regard to CVD risk factors-Statin users had more risk factors; groups not initially comparable-Statin eligible vs. non had inherent risk differences by definitionMultivariable cox regression model adjusted for CVD risk factors-Statin users had higher burden of risk factors and comorbiditiesPropensity score-matched analysis achieved no significant baseline differencesPropensity-score matched; statin vs. non-statin groups well balanced across various CVD risk factorsInverse probability treatment weighting used; baseline characteristics balanced between statin vs. non-statin groups-No predetermined groups similar in CVD risk factorsN/AFine-Gray regression model for CVD events adjusted for cardiac risk factors2. Study cohorts are similar in regard to ageMultivariable Cox adjusted for age and CVD risk factors-No separate age adjustment for eligibility groups; adjusted analysis performed for actual statin useMultivariable cox regression model adjusted for age, sex comorbiditiesMultivariate time-dependent Cox regression model adjusted for age, sex and baseline co-morbiditiesCox regression models adjusted for age, sex, and comorbiditiesMultivariable cox regression models adjusted for age, sex, and comorbiditiesMulti-variable fine-gray model adjusted for age, sex, stage, smokingMultivariate predictors of MACE after RT adjusted for age, RT dose, diabetes, aspirin use, beta-blocker useN/AFine-Gray regression model for CVD events includes adjustment for ageOutcome1. Assessment of outcomeOutcomes adjudicated by blinded specialists via recordsASCVD events from records, adjudicated blinded to exposuresMACE and deaths identified via chart review and adjudication by cardiologistOutcomes stroke, MI via linked hospital records and validated ICD codes.Stroke/TIA outcomes identified via claims and ICD codes assigned by physiciansMACE outcomes captured via claims and national death registry, ensuring independent verification.Ischaemic stroke events captured via ICD-9/12 codes assigned by neurologistsAF outcome assessed rigorously: cardiologists blinded to RT dose adjudicated AF from ECGs, monitorsCVD diagnoses confirmed via history; risk calculated by Framingham ScoreClinical records were interrogated for cardiac events with three cardiologists verifying cardiac events2. Was follow-up long enough for outcomes to occur (minimum of 5 year)---**-N/A-What was the median duration of follow-up?Median 3.4 years, ≈ 40 monthsMedian 6.6 yearsMedian 20.4 months follow-up; survivors median 48.1 monthsMean follow-up ~ 1.5 years; short due to data limitsFollow-up up to 11 years; broad range. Median not stated.5.02 years7.5 years22.8 months24 months21.1 months3. Adequacy of follow-up cohortsNo losses reported; retrospective chart follow-up to last visitComplete outcome capture via linked databases; minimal loss-Vital status obtained for all patients, but no statement on other lossesNo loss to follow-up; comprehensive provincial health data capture.No loss to follow-up; 99.9% population coverage in National Health Insurance Research DatabaseComplete follow-up via linked registryComplete follow-up; national cancer registry with follow-up to end of 2020.-High mortality of oesophageal cancer limited long-term follow-upN/A*Good data availability, patient attrition was rare.Total (out of 9)666699963/37
Discussion
This systematic review demonstrates the paucity of evidence exploring cardioprotective medication use in patients treated with RT. Most included studies were retrospective, with no randomized control studies conducted to date. Many patients treated with RT have indications for the commencement of statins although are not currently prescribed them.
Whilst this systematic review and meta-analysis suggests that the risk of cerebrovascular events (stroke and TIA) is reduced with statin therapy in patients treated with RT, this finding must be interpreted with caution given the small number of studies in the meta-analysis and the significant between study heterogeneity. All three studies investigating statin use in the HNC population were retrospective in nature and were investigating incidental statin use which introduces inherent biases. Two of the three studies included in the cerebrovascular meta-analysis [12, 20] were of moderate quality (both 6 out of 9 on the Newcastle Ottawa Scale), suggesting that the overall strength of evidence is low. Both these studies [12, 20] did not balance for confounders between the two groups (statin and no statin groups) and they had short follow-up periods (less than 5 years). Addison et al. reported a reduction in the risk of CVE (stroke or TIA) post RT for patients on statin therapy in a multivariable regression analysis (HR 0.41, 95% CI 0.21 to 0.80) [12]. Similarly, Boulet et al. observed a 32% reduction in stroke incidence among post-RT statin users (aHR = 0.68, 95% CI 0.48–0.98) for patients treated with RT to the head and neck or thorax [20]. Utilizing a cohort of patients with nasopharyngeal cancer only, Lin et al. suggested that statin use during RT was associated with reduced risk of ischemic stroke (aHR 0.70, 95% CI 0.54 to 0.92, p< 0.01) [15]. Randomized controlled trials examining the effects of cardioprotective medications, specifically statins, in a population of patients treated with RT would be of high clinical significance. Many important clinical questions remain, such as whether statin therapy needs to be initiated during or after radiotherapy, or whether patients without traditional CVD risk factors but are receiving radiotherapy would benefit from the early introduction of statin therapy. For patients with human papillomavirus associated oropharyngeal cancer or nasopharyngeal cancer this is especially important, as these patients commonly are younger, have improved survival and are less likely to have other pre-existing co-morbidities.
The evidence for the role of cardioprotective medications in reducing risk of major adverse cardiovascular events (MACE) for patients receiving RT to the thorax is more heterogeneous, with this meta-analysis suggesting no benefit. However, this is a varied group of studies comprising different sub-groups of patients. There was only one study which demonstrated a benefit to cardioprotective medications in this population and this was for patients treated with adjuvant RT for breast cancer [19]. This manuscript by Huang et al. suggested statin therapy more than halved the 5-year MACE incidence (12.2% vs. 31.7% in non-statin users), with a hazard ratio of 0.34 (95% CI 0.25–0.44) favoring statin users [19]. In patients with lung cancer, Atkins et al. found that statin users and non-statin users had similar rates of cardiac events (adjusted HR 1.18, P= 0.69) [17]. Walls et al. suggested that patients receiving statin therapy had improved overall survival, however there were no differences in cardiac events between the two groups [18].
Another area of ongoing research is whether the intensity of statin therapy is correlated with cerebrovascular or cardiovascular outcomes in patients treated with RT. Three studies identified in this systematic review investigated the effect of statin intensity, one study in patients with lung cancer [18] one in patients with nasopharyngeal cancer [15] and one in patients who were treated for breast cancer [19]. All three of these studies suggested that there was a dose response relationship for statin therapy. The study by Walls et al.[18] demonstrated that patients receiving high-intensity statin therapy had improved survival. Similar results were demonstrated in the study by Lin et al.,[15] with higher intensity statin therapy associated with a lower hazard ratio of ischemic stroke. The timing of statin therapy is another issue which requires ongoing investigation. This systematic review identified that definitions of statin use were heterogenous (Table 1) with some studies defining use as during or at the time of RT, and others defining statin users as those who were prescribed statins at any time after RT. Future studies to address whether the timing of statin use in relation to RT impacts cerebrovascular or cardiovascular even rates would be of clinical importance.
One of the major findings from this study is that many patients undergoing RT are not prescribed cardio preventative medications, with up to 60% of patients not on statin treatments having an indication to commence one. Whilst there is currently limited high-quality evidence to guide management options in patients treated with RT, it seems plausible that at a minimum clinicians should advocate for commencement of these cardioprotective medications as suggested in existing guidelines. There is also emerging evidence that the risk of CVD in patients treated with RT is higher than predicted by traditional risk scores. For example, the study by Miller et al. highlights RT as a risk factor for the development of arrythmias in a cohort of patients with esophageal cancer, with 21.4% of the cohort developing new-onset AF post-RT, 9-fold higher than predicted by Framingham scores [16]. The multi-disciplinary expert consensus statement from the International Cardio-Oncology Society [22] provides practical guidance to clinicians on the optimal identification and management of CVD risk in this population. For patients previously treated with RT, the recommendation is for regular screening and aggressive treatment of CVD risk factors and disease, although the time intervals for screening are dependent upon individual patient risk.
A major limitation of this systematic review and meta-analysis is the between study heterogeneity with variations in patient populations, tumor subsites and cardioprotective medication use definitions (either before, during or after RT). These heterogeneities limit the interpretability of the meta-analyses findings and suggest that further high quality prospective research is required to determine the impacts of statins in patients treated with RT. Another limitation is that the evidence base for cardioprotective therapies in patients treated with RT is uneven, with most eligible studies evaluating statins and limited data for antihypertensive or antithrombotic therapies. Furthermore, the protocol was not prospectively registered (PROSPERO), however, eligibility criteria, outcomes of interest, and analytic methods were defined prior to full-text screening, and PRISMA reporting was followed.
Conclusion
Many patients undergoing RT are not prescribed cardioprotective medications as suggested by existing CVD guidelines. Future prospective research is needed to explore the impacts of cardioprotective medications specifically in patients treated with RT
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Majeed H, Gupta V. Adverse effects of radiation therapy. Stat Pearls. 2025.33085406 · pubmed ↗
- 2Siaravas KC, Katsouras CS, Sioka C. Radiation treatment mechanisms of cardiotoxicity: A systematic review. Int J Mol Sci Mar. 2023;27(7). 10.3390/ijms 24076272.10.3390/ijms 24076272 PMC 1009408637047245 · doi ↗ · pubmed ↗
- 3O’Regan C, Wu P, Arora P, Perri D, Mills EJ. Statin therapy in stroke prevention: a meta-analysis involving 121,000 patients. Am J Med. Jan 2008;121(1):24–33. 10.1016/j.amjmed.2007.06.033.10.1016/j.amjmed.2007.06.03318187070 · doi ↗ · pubmed ↗
- 4Zhang SC, Gasho JO, Eno C et al. Early cardio-oncology intervention in thoracic radiotherapy: prospective single-arm pilot study. Commun Med. 2025/02/17 2025;5(1):43. 10.1038/s 43856-025-00761-6.10.1038/s 43856-025-00761-6PMC 1183304739962137 · doi ↗ · pubmed ↗
- 5Alvi RM, Quinaglia T, Spahillari A, et al. The prediction of cardiac events using contemporary risk prediction models after radiation therapy for head and neck cancer. Cancers. 2022;14(15). 10.3390/cancers 14153651.10.3390/cancers 14153651 PMC 936737835954315 · doi ↗ · pubmed ↗
- 6Boulet J, Peña J, Hulten EA, et al. Statin use and risk of vascular events among cancer patients after radiotherapy to the thorax, head, and neck. J Am Heart Association. 2019;8(13). 10.1161/JAHA.117.005996.10.1161/JAHA.117.005996 PMC 666234031213106 · doi ↗ · pubmed ↗