Human Papillomavirus Vaccination Policies and Discourse on Social Media
Lanyue Zhang, Shouchuang Zhang, Siqi Liu, Weiyan Jian

TL;DR
This study examines how HPV vaccination policies in China influenced public discussions on social media, finding that policies reduced access concerns and increased awareness and gender equity conversations.
Contribution
The study provides new insights into how national HPV vaccination policies in China affect public discourse and engagement on social media platforms.
Findings
After policy implementation, discussions on vaccine accessibility decreased substantially.
Conversations about health awareness and gender equity increased significantly.
Social media data can offer timely insights into public responses to health interventions.
Abstract
This cross-sectional study explores whether the 2 national human papillomavirus (HPV) vaccination policies were associated with increased public discourse related to the policies on a social media platform in China. Were the 2 national human papillomavirus (HPV) vaccination policies in China associated with changes in public responses and engagement? In this cross-sectional study using 3-year interrupted time-series analysis of 353 530 online posts (2021-2024), discussions on vaccine accessibility decreased substantially after policy implementation, while conversations about health awareness and gender equity issues increased. Results of this study suggest that national HPV vaccination policies in China significantly influenced public perceptions and discussions, supporting efforts to achieve equitable vaccine uptake and cervical cancer elimination. Cervical cancer remains a major…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
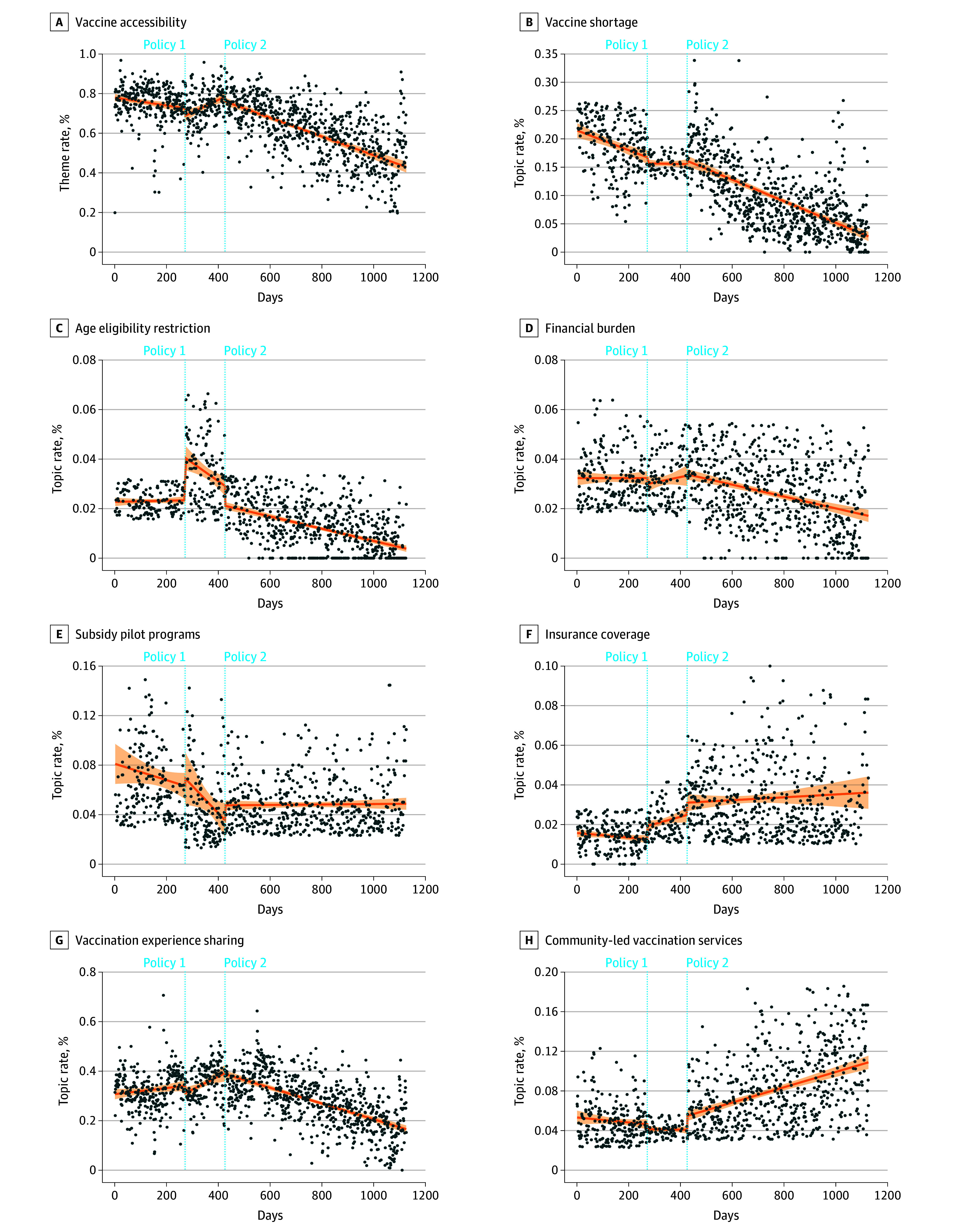 Figure 1
Figure 1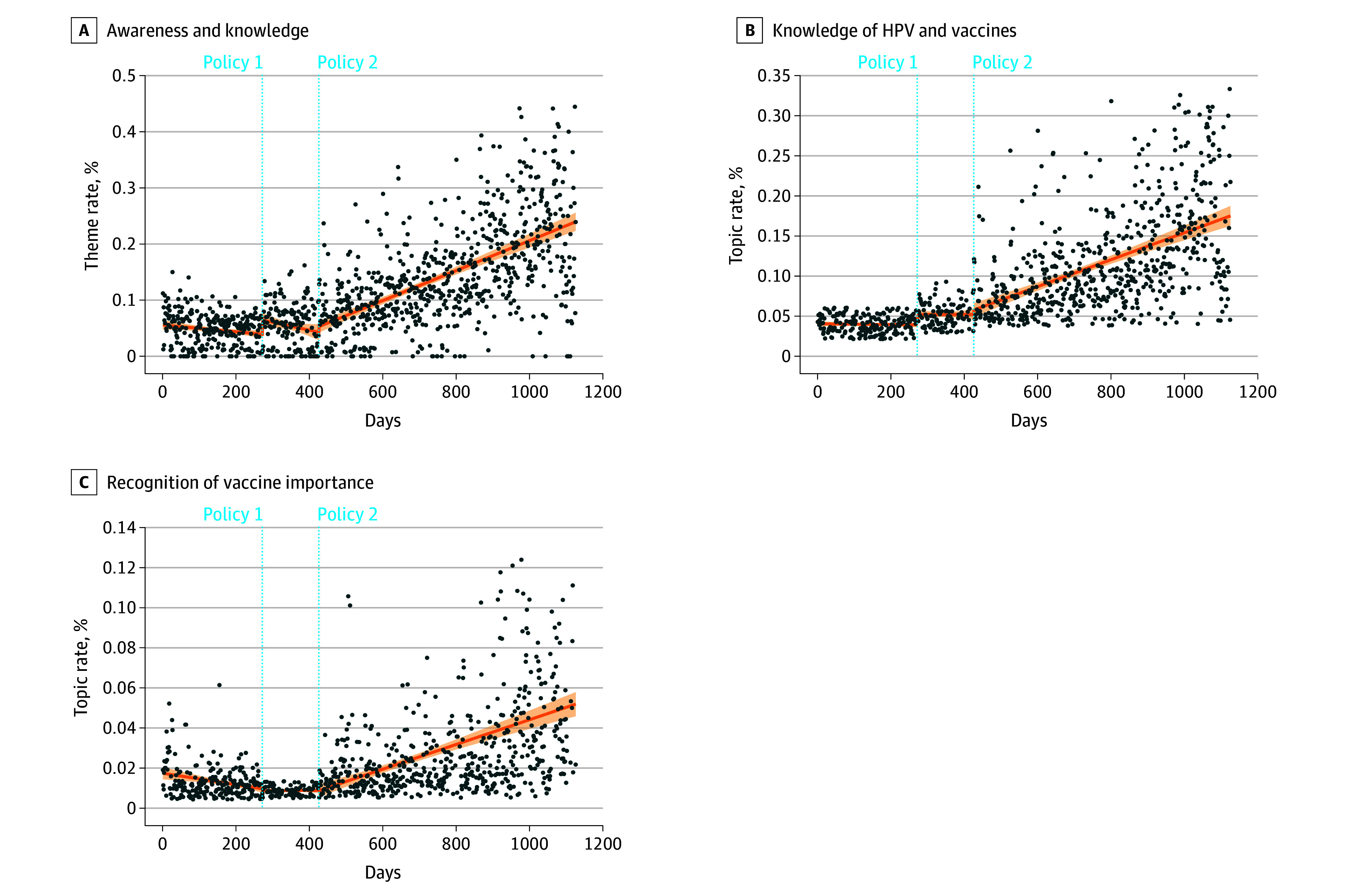 Figure 2
Figure 2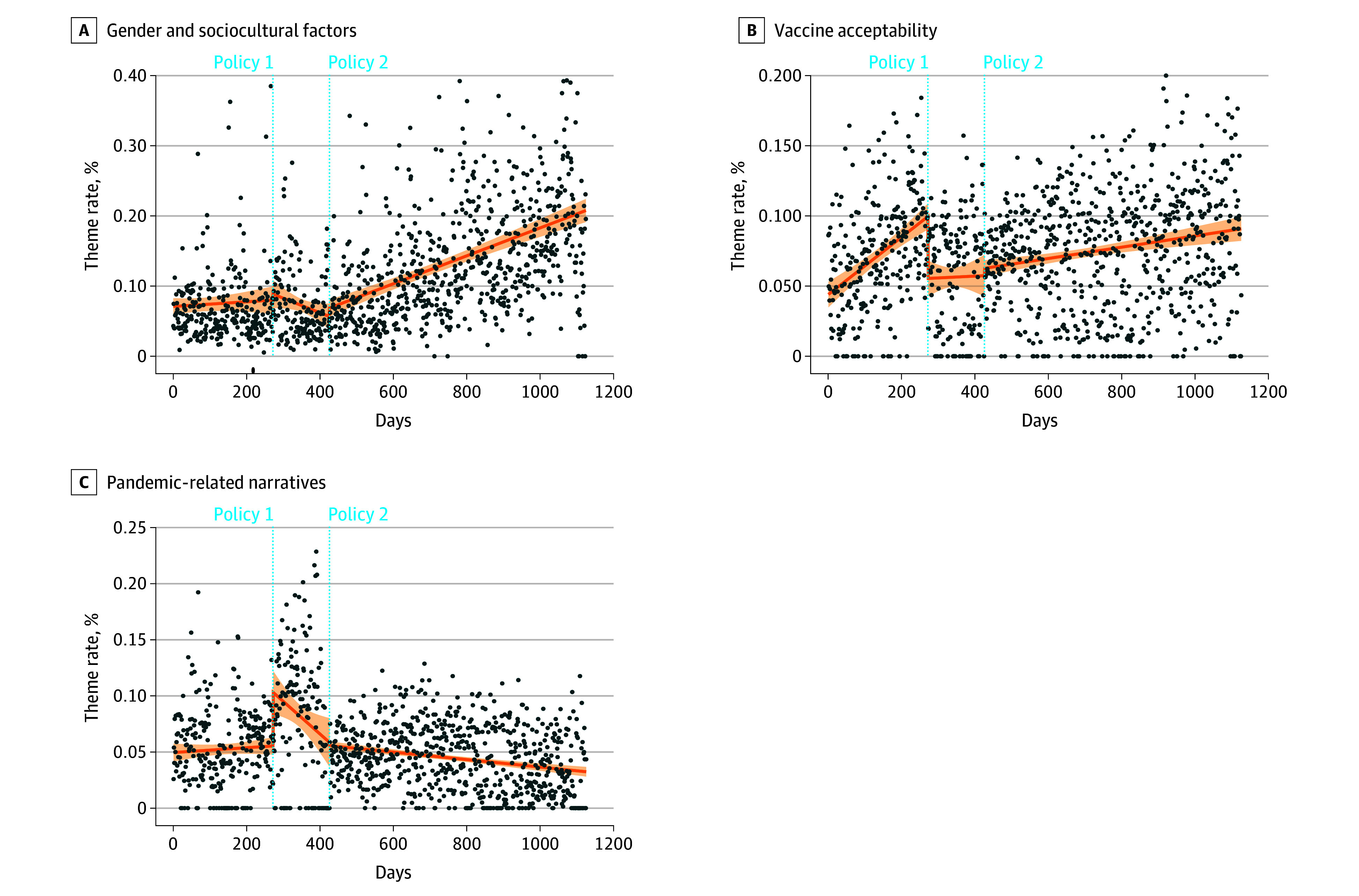 Figure 3
Figure 3| Themes and topics | Posts (n = 353 530), No. (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Policy | Sex | Region | ||||||
| Before policy 1 | After policy 1 before policy 2 | After policy 2 | Male | Female | Eastern | Central | Western | |
| Theme 1: vaccine accessibility | 87 784 (24.8) | 27 752 (7.9) | 104 902 (29.7) | 42 572 (12.0) | 177 343 (50.2) | 145 231 (41.1) | 38 113 (10.8) | 37 048 (10.5) |
| Vaccine shortage | 16 263 (4.6) | 2323 (0.7) | 21 014 (5.9) | 7502 (2.1) | 32 002 (9.1) | 24 961 (7.1) | 7502 (2.1) | 7408 (2.1) |
| Age eligibility restriction | 1758 (0.5) | 1256 (0.4) | 2299 (0.7) | 1012 (0.3) | 4285 (1.2) | 3627 (1.0) | 1012 (0.3) | 876 (0.3) |
| Financial burden | 3657 (1.0) | 1239 (0.4) | 4598 (1.3) | 2226 (0.6) | 2253 (0.6) | 6247 (1.8) | 2226 (0.6) | 1667 (0.5) |
| Subsidy pilot programs | 10 335 (2.9) | 2348 (0.7) | 5737 (1.6) | 4551 (1.3) | 13 844 (3.9) | 13 107 (3.7) | 4551 (1.3) | 2642 (0.8) |
| Insurance coverage | 1681 (0.5) | 735 (0.2) | 4460 (1.3) | 1819 (0.5) | 5042 (1.4) | 4595 (1.3) | 1819 (0.5) | 1106 (0.3) |
| Vaccination experience sharing | 49 564 (14.0) | 19 012 (5.4) | 52 877 (15.0) | 20 150 (5.7) | 100 979 (28.6) | 80 082 (22.7) | 20 150 (5.7) | 20 463 (5.8) |
| Community-led vaccination services | 4526 (1.3) | 839 (0.2) | 13 917 (3.9) | 5312 (1.5) | 13 938 (3.9) | 12 672 (3.6) | 5312 (1.5) | 2886 (0.8) |
| Theme 2: vaccine acceptability | 6439 (1.8) | 1988 (0.6) | 15 448 (4.4) | 6830 (1.9) | 17 005 (4.8) | 15 824 (4.5) | 4411 (1.3) | 3640 (1.0) |
| Affirmative vaccine perception | 1486 (0.4) | 414 (0.1) | 6969 (2.0) | 2760 (0.8) | 6101 (1.7) | 6134 (1.7) | 2760 (0.8) | 1173 (0.3) |
| Hesitancy and adverse concerns | 4953 (1.4) | 1574 (0.5) | 8479 (2.4) | 4070 (1.2) | 10 904 (3.1) | 9690 (2.7) | 4070 (1.2) | 2467 (0.7) |
| Theme 3: awareness and knowledge | 5232 (1.5) | 1703 (0.5) | 32 824 (9.3) | 12 983 (3.7) | 26 723 (7.6) | 26 193 (7.4) | 7757 (2.2) | 5807 (1.6) |
| Knowledge of HPV and vaccines | 3727 (1.1) | 1399 (0.4) | 24 942 (7.1) | 9849 (2.8) | 20 175 (5.7) | 19 534 (5.5) | 9849 (2.8) | 4546 (1.3) |
| Recognition of vaccine importance | 1505 (0.4) | 304 (0.1) | 7882 (2.2) | 3134 (0.9) | 6548 (1.9) | 6659 (1.9) | 3134 (0.9) | 1261 (0.4) |
| Theme 4: gender and sociocultural factors | 10 371 (2.9) | 2637 (0.8) | 40 382 (11.4) | 15 928 (4.5) | 37 992 (10.8) | 34 098 (9.7) | 10 992 (3.1) | 9263 (2.6) |
| Women’s health and rights | 4416 (1.3) | 1031 (0.3) | 14 697 (4.2) | 6300 (1.8) | 13 823 (3.9) | 13 124 (3.7) | 6300 (1.8) | 3121 (0.9) |
| Male vaccination debate | 1493 (0.4) | 344 (0.1) | 4126 (1.2) | 2215 (0.6) | 3739 (1.1) | 4023 (1.1) | 2215 (0.6) | 963 (0.3) |
| Stigma and moral judgment | 4462 (1.3) | 1262 (0.4) | 21 559 (6.1) | 6783 (2.0) | 20 430 (5.8) | 16 951 (4.8) | 6783 (1.9) | 5179 (1.5) |
| Theme 5: pandemic-related narratives | 5418 (1.5) | 2729 (0.8) | 7921 (2.2) | 4875 (1.4) | 11 158 (3.2) | 10 335 (2.9) | 2992 (0.9) | 2741 (0.8) |
| Vaccination disruption | 3174 (0.9) | 1715 (0.5) | 1476 (0.4) | 1313 (0.4) | 5040 (1.4) | 4081 (1.2) | 1313 (0.4) | 1132 (0.3) |
| Pandemic-induced vaccine distrust | 2244 (0.6) | 1014 (0.3) | 6445 (1.8) | 3562 (1.0) | 6118 (1.7) | 6254 (1.8) | 3562 (1.0) | 1609 (0.5) |
| Total | 115 244 (32.6) | 36 809 (10.4) | 201 477 (57.0) | 82 558 (23.4) | 270 221 (76.4) | 231 681 (65.5) | 63 350 (17.9) | 58 499 (16.6) |
| Themes and topics | Level change (policy 1) | Slope change (policy 1) | Level change (policy 2) | Slope change (policy 2) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Regression coefficient (95% CI) | Newey-West SE | Regression coefficient (95% CI) | Newey-West SE | Regression coefficient (95% CI) | Newey-West SE | Regression coefficient (95% CI) | Newey-West SE | |||||
| Theme 1: vaccine accessibility | −3.76 (−7.49 to −0.04) | .05 | 1.900 | 0.08 (0.05-0.12) | <.001 | 0.017 | −2.39 (−5.59 to 0.81) | .14 | 1.633 | −0.11 (−0.14 to −0.08) | <.001 | 0.016 |
| Vaccine shortage | −1.07 (−2.45 to 0.31) | .13 | 0.705 | 0.02 (0.01-0.03) | .01 | 0.006 | 0.57 (−0.67 to 1.82) | .37 | 0.634 | −0.02 (−0.02 to −0.01) | <.001 | 0.005 |
| Age eligibility restriction | 1.71 (1.12-2.23) | <.001 | 0.264 | −0.01 (−0.01 to −0.003) | .003 | 0.003 | −0.80 (−1.22 to −0.39) | <.001 | 0.214 | 0.01 (0.000-0.01) | .049 | 0.002 |
| Financial burden | −0.24 (−0.66 to 0.18) | .26 | 0.214 | 0.002 (−0.002 to 0.01) | .34 | 0.002 | 0.05 (−0.41 to 0.52) | .82 | 0.238 | −0.01 (−0.01 to 0.000) | .03 | 0.002 |
| Subsidy pilot programs | 0.62 (−1.75 to 2.98) | .61 | 1.206 | −0.02 (−0.04 to 0.01) | .17 | 0.011 | 1.21 (−0.23 to 2.65) | .10 | 0.733 | 0.02 (0.002-0.04) | .03 | 0.010 |
| Insurance coverage | 0.67 (0.34-0.99) | <.001 | 0.167 | 0.01 (0.001-0.01) | .01 | 0.002 | 0.62 (0.06-1.19) | .03 | 0.288 | −0.003 (−0.01 to 0.001) | .15 | 0.002 |
| Vaccination experience sharing | −2.98 (−6.24 to 0.28) | .07 | 1.663 | 0.04 (0.004-0.08) | .03 | 0.019 | −0.39 (−4.03 to 3.26) | .84 | 1.859 | −0.08 (−0.12 to −0.05) | <.001 | 0.018 |
| Community-led vaccination services | −0.50 (−1.13 to 0.13) | .12 | 0.321 | 0.002 (−0.004 to 0.01) | .47 | 0.003 | 1.40 (0.76-2.04) | <.001 | 0.326 | 0.01 (0.003-0.01) | <.001 | 0.002 |
| Theme 2: vaccine acceptability | −4.41 (−5.99 to −2.84) | <.001 | 0.804 | −0.02 (−0.04 to −0.003) | .02 | 0.008 | 0.52 (−1.07 to 2.11) | .52 | 0.811 | 0.003 (−0.01 to 0.02) | .73 | 0.008 |
| Affirmative vaccine perception | −0.39 (−0.63 to −0.15) | <.001 | 0.122 | 0.001 (−0.001 to 0.003) | .20 | 0.001 | −0.37 (−0.72 to −0.02) | .04 | 0.177 | 0.004 (0.002-0.01) | <.001 | 0.001 |
| Hesitancy and adverse concerns | −2.45 (−3.36 to −1.53) | <.001 | 0.468 | −0.01 (−0.02 to 0.000) | .04 | 0.004 | 0.33 (−0.48 to 1.15) | .42 | 0.416 | −0.01 (−0.02 to −0.002) | .01 | 0.004 |
| Theme 3: awareness and knowledge | 2.52 (1.10-3.93) | <.001 | 0.722 | −0.01 (−0.02 to 0.01) | .33 | 0.008 | 0.98 (−0.78 to 2.73) | .28 | 0.895 | 0.04 (0.03-0.06) | <.001 | 0.008 |
| Knowledge of HPV and vaccines | 1.29 (0.65-1.93) | <.001 | 0.326 | 0.001 (−0.01 to 0.01) | .88 | 0.004 | 0.54 (−0.53 to 1.61) | .32 | 0.545 | 0.02 (0.01-0.02) | <.001 | 0.004 |
| Recognition of vaccine importance | −0.10 (−0.31 to 0.12) | .39 | 0.111 | 0.003 (0.001-0.01) | .01 | 0.001 | −0.02 (−0.37 to 0.34) | .93 | 0.178 | 0.01 (0.004-0.01) | <.001 | 0.001 |
| Theme 4: gender and sociocultural factors | 0.87 (−1.91 to 3.66) | .54 | 1.420 | −0.02 (−0.05 to −0.001) | .04 | 0.012 | 1.18 (−1.00 to 3.35) | .29 | 1.111 | 0.04 (0.02-0.06) | <.001 | 0.011 |
| Women’s health and rights | 0.43 (−0.40 to 1.26) | .31 | 0.423 | −0.01 (−0.011 to 0.000) | .07 | 0.003 | −0.81 (−1.58 to −0.027) | .04 | 0.397 | 0.02 (0.01-0.03) | <.001 | 0.003 |
| Male vaccination debate | 0.15 (−0.17 to 0.46) | .36 | 0.160 | −0.003 (−0.01 to 0.000) | .06 | 0.001 | 0.82 (0.49-1.14) | <.001 | 0.167 | 0.004 (0.002-0.01) | <.001 | 0.001 |
| Stigma and moral judgment | −0.23 (−1.84 to 1.38) | .78 | 0.821 | −0.02 (−0.03 to −0.01) | .002 | 0.006 | 2.87 (1.78-3.96) | <.001 | 0.556 | 0.01 (0.003-0.03) | .01 | 0.006 |
| Theme 5: pandemic-related narratives | 4.79 (2.72-6.85) | <.001 | 1.054 | −0.03 (−0.06 to −0.01) | .01 | 0.012 | −0.29 (−2.49 to 1.91) | .80 | 1.122 | 0.03 (0.003-0.05) | .03 | 0.012 |
| Vaccination disruption | 2.13 (1.17-3.09) | <.001 | 0.490 | 0.01 (−0.002 to 0.023) | .10 | 0.006 | −7.16 (−8.40 to −5.91) | <.001 | 0.636 | −0.02 (−0.03 to −0.003) | .01 | 0.006 |
| Pandemic-induced vaccine distrust | 0.45 (0.13-0.78) | <.006 | 0.167 | −0.004 (−0.01 to 0.000) | .03 | 0.002 | 1.14 (0.71-1.58) | <.001 | 0.222 | 0.003 (−0.001 to 0.01) | .11 | 0.002 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Vaccine Coverage and Hesitancy · Health Literacy and Information Accessibility
Introduction
Human papillomavirus (HPV) infection is the most common sexually transmitted infection worldwide and the leading cause of cervical cancer, which remains a substantial global public health challenge.^1,2,3,4^ HPV vaccination, recommended by the World Health Organization, is a highly effective measure to prevent HPV infection and reduce cervical cancer incidence.^5^ To increase HPV vaccine coverage, many countries have introduced various vaccination policies.^6,7,8^ Yet, the success of these policies also depends on how they are perceived and received by the public.^9^ Conventionally, the effectiveness of public health policies is evaluated primarily through metrics such as final coverage rates.^10,11,12^ However, this approach often overlooks a crucial intermediary layer: the dynamic shifts in public discourse, perceptions, and concerns that occur in response to policy implementation.^13,14^ Public reaction actively shapes the social environment in which policies operate, influencing individual vaccine awareness, attitudes, discussions, and ultimately, the policy’s overall effectiveness.^15,16^ Understanding how policies impact public discussions is crucial for ensuring equitable HPV vaccine uptake and advancing progress toward cervical cancer elimination.^17^
In China, understanding public reception is especially crucial. Although HPV vaccines became available in mainland China in 2016, vaccination coverage remains low.^18,19^ The national HPV vaccination program has a narrow scope, with eligibility restrictions by age, sex and gender, and geographic location, alongside disparities in public perceptions of the vaccine. By 2022, only 10.2% of Chinese females aged 9 to 45 years had received at least 1 dose of the HPV vaccine, far below the global average of 20%.^20^ Recognizing these challenges, China has introduced a series of policy interventions to accelerate vaccine coverage. The 9-valent HPV vaccine was initially approved only for females aged 16 to 26 years, with a strictly limited age eligibility. In August 2022, the National Medical Products Administration expanded the approved age range to 9 to 45 years, substantially relaxing the previous restriction.^19,21^ Subsequently, in January 2023, the National Health Commission launched the Action Plan for Accelerating the Elimination of Cervical Cancer (2023-2030).^22^ This action plan outlined comprehensive national goals to eliminate cervical cancer, emphasizing HPV vaccination coverage, encouragement of HPV vaccination pilot programs, public health education and prevention, and cervical cancer screening and treatment as core strategies. It places special attention on girls, women, and disadvantaged populations (individuals in rural areas or with lower socioeconomic status), and emphasizes the principle of equitable access across urban and rural areas.^23,24^ However, previous studies suggest that public perceptions and responses to national HPV vaccination interventions, particularly concerning accessibility, health equity, and awareness, remain poorly understood.^18,25,26^
Traditionally, surveys and interviews have been used to assess public perceptions of vaccination programs, but these methods often have small sample sizes, recall bias, and reporting delays.^27,28,29^ In contrast, social media platforms offer a current and ongoing source of public discourse, enabling researchers to observe population-level responses to health interventions at scale.^30,31,32^ Previous studies also highlighted that digital public health surveillance through social media listening has emerged as a powerful tool for tracking information dissemination, risk perceptions, and community reactions to health policies.^33,34^ In China, Sina Weibo, the country’s largest microblogging platform with more than 580 million active users, has been widely used for understanding public reactions to policy interventions on influenza and COVID-19.^35,36^ Yet, to our knowledge, few studies have leveraged large-scale social media data to evaluate public responses to national-level HPV vaccination policy implementation.
This study aims to investigate impacts of 2 major HPV vaccination policy interventions in China in terms of public discourse and perceptions as expressed on social media. By analyzing 3 years of online conversations, we seek to capture public attitudes and dynamic responses to these policies; explore barriers related to accessibility, equity, and health awareness; and provide insights for promoting equitable and sustained HPV vaccine uptake.
Methods
Study Design
This cross-sectional study used a dataset that included posts related to HPV, cervical cancer, and HPV vaccination, collected from the Sina Big Data System under a data purchase agreement between the School of Public Health, Peking University, and Sina Corporation. Posts were filtered by geotags to ensure relevance to the study area, and only publicly available information shared by users was analyzed. All data were anonymized to exclude sensitive or private information. Keywords for post identification were determined under the guidance of an HPV vaccination expert, with semantic mapping across Chinese and English to ensure comprehensive coverage (eTables 1 and 2 in Supplement 1). Posts published between December 1, 2021, and December 31, 2024, were included. Latent Dirichlet allocation (LDA) topic modeling was applied to process textual data, followed by manual topic classification. Study protocols were approved by the Medical Research Ethics Committee of Peking University Health Science Center. This study was approved by the relevant ethics committee. A waiver of informed consent was granted because the study used anonymized deidentified datasets. The overview of the study design is shown in eFigure 1 in Supplement 1. This study has been reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) consensus criteria.^37^
Data Collection and Processing
We initially collected 2 906 365 posts from the social media platform using keyword filters combined with temporal and geographic parameters. After excluding 426 015 posts published by nonindividual accounts, 947 818 meaningless information posts (symbols or emojis), 75 446 unknown and overseas posts, 19 013 missing or non-Chinese posts, 44 301 duplicate posts (identical content from the same user), and 471 025 unrelated posts (non-HPV topics), a final dataset of 353 530 posts was retained for analysis. eFigure 2 in Supplement 1 presents the inclusion and exclusion flowchart. Data processing and analysis were conducted using Python version 3.11.7 (Python Software Foundation). Text content was extracted from posts and preprocessed by removing emojis and other nontextual elements. We applied the Jieba Chinese word segmentation library in Python to tokenize each post and removed common stop words with limited analytical value.
Topic Modeling
An LDA model was implemented in the Python Gensim library to identify latent topics within the Weibo dataset. To mitigate the influence of bot-generated posts and highly similar content, we excluded samples with more than 90% textual similarity (retaining only 1 representative post) and iteratively refined the LDA model. This process continued until artificially clustered topics attributable to bots were no longer detected. To determine the optimal number of topics, we calculated the topic coherence score, which quantifies the semantic consistency of a topic by evaluating the co-occurrence strength of high-frequency words within it. Because higher scores indicate more interpretable and semantically coherent topics, we adopted the topic number with the highest coherence score: K = 16 (eFigure 3 in Supplement 1). Finally, each post was assigned to the topic with the highest posterior probability based on all words in the corpus.
Statistical Analysis
We adopted quantitative descriptive analysis to report the themes and topics of HPV discussions on Weibo. The characteristics of posts were calculated using counts and percentage values. This study applied interrupted time-series (ITS) analysis to evaluate public responses to 2 major national HPV-related policies in China (eMethods in Supplement 1). Additionally, to assess the robustness of our findings, a sensitivity analysis was conducted using the daily total number of HPV-related posts as an alternative outcome in the ITS analysis. Data analyses were conducted in Python version 3.11.7. Two-sided P < .05 was considered statistically significant.
Results
General Statistics and LDA Topic Modeling
Using LDA, we automatically identified 16 distinct topics from the corpus of posts based on textual content. These topics were then manually grouped into 5 overarching thematic domains: vaccine accessibility, vaccine acceptability, vaccine awareness and knowledge, gender and sociocultural discussions, and pandemic-related narratives. Table 1 shows a summary of each theme and its constituent topics. Overall, females contributed a larger share of posts (270 221 [76.44%]) compared with males (82 558 [23.35%]). Regionally, post volume was highest in eastern (231 681 [65.53%]) and lowest in western (58 499 [16.55%]) provinces. Thematic framework development is described in the eAppendix in Supplement 1, with representative posts and top terms summarized in eTable3 in Supplement 1.
Among all themes, vaccine accessibility emerged as the most prevalent, accounting for 220 438 of the total posts (62.35%). This theme included 7 topics: vaccine shortages, age eligibility restrictions, financial burdens, subsidy pilot programs, health insurance relief, vaccination experience sharing, and community-led vaccination services. The second most prevalent theme was “gender and sociocultural factors” (53 390 [15.10%]), followed by “awareness and knowledge” (39 759 [11.25%]), “vaccine acceptability” (23 875 [6.75%]), and finally, “pandemic-related narratives” (16 068 [4.55%]).
ITS Analysis Results
We report changes in topic trends following each policy to evaluate their immediate and long-term effects (Table 2). After the implementation of policy 1 (August 2022 age expansion approval for HPV vaccination), overall discussions related to vaccine accessibility showed a decline. However, specific topics such as age eligibility restriction (regression coefficient: 1.71; 95% CI, 1.20-2.23; P < .001) and insurance coverage (regression coefficient: 0.67; 95% CI, 0.34-0.99; P < .001) showed a significant increase in discussion. Similarly, after policy 2 (January 2023 National Action Plan for Accelerating the Elimination of Cervical Cancer) was announced, discussions around insurance coverage increased (regression coefficient: 0.62; 95% CI, 0.06-1.19; P < .05), accompanied by a marked increase in community-led vaccination services (regression coefficient: 1.40; 95% CI, 0.76-2.04; P < .001).
However, over time, the trends in public discourse revealed distinct patterns. In terms of gradual effects, there was a significant upward trend in vaccine accessibility discussions following policy 1, with an additional increase of 0.08 percentage points per day (regression coefficient: 0.08; 95% CI, 0.05-0.12; P < .001). This growth was driven by heightened conversations about vaccine shortages (regression coefficient: 0.02; 95% CI, 0.01-0.03; P < .01), indicating growing demand pressure, and by steady increases in vaccination experience sharing (regression coefficient: 0.04; 95% CI, 0.004-0.08; P < .05). Mentions of insurance coverage also showed a moderate yet significant increase (regression coefficient: 0.01; 95% CI, 0.000-0.01; P < .05).
In contrast, following policy 2, discussions within the vaccine accessibility theme decreased by 0.11 percentage points per day (regression coefficient: 0.11; 95% CI, −0.14 to −0.08; P < .001). Although certain topics such as subsidy pilot programs (regression coefficient: 0.02; 95% CI, 0.002-0.04; P < .05) and community-led vaccination services (regression coefficient: 0.01; 95% CI, 0.003-0.01; P < .010) continued to increase, discussions of vaccine shortages (regression coefficient: −0.02; 95% CI, −0.03 to −0.01; P < .001), financial burden (regression coefficient: −0.01; 95% CI, −0.01 to −0.000; P < .05), and vaccination experience sharing (regression coefficient: −0.08; 95% CI, −0.12 to −0.05; P < .001) declined significantly over time. The temporal dynamics of discussions within the vaccine accessibility theme and its 7 constituent topics are illustrated in Figure 1.
Dot Plots Showing Daily Trends in Public Discussions on Human Papillomavirus Vaccine Accessibility and Its 7 Subtopics on Social Media PostsThe shading indicates the 95% CI around the fitted trend line.
Within the awareness and knowledge theme, policy 1 was associated with a notable but short-lived increase in public discussions after its implementation, with a significant increase in posts related to HPV knowledge and vaccine value recognition (regression coefficient: 2.52; 95% CI, 1.10-3.93; P < .001). However, no significant changes in the subsequent trend were observed following this initial increase. In contrast, policy 2 was associated with a sustained upward trajectory in this theme, as the prevalence of related discussions grew by 0.04 percentage points per day (regression coefficient: 0.04; 95% CI, 0.03-0.06; P < .001). Specifically, mentions of knowledge of HPV and vaccines increased steadily at 0.02 percentage points per day (regression coefficient: 0.02; 95% CI, 0.01-0.02; P < .001), while recognition of vaccine importance also exhibited a consistent increase of 0.01 percentage points per day (regression coefficient: 0.01; 95% CI, 0.004-0.01; P < .001). These temporal trends in discussions around HPV awareness and knowledge, including the 2 constituent topics, are illustrated in Figure 2.
Dot Plots Showing Daily Trends in Public Discussions on Awareness and Knowledge and Its 2 Subtopics on Social Media PostsThe shading indicates the 95% CI around the fitted trend line. HPV indicates human papillomavirus.
Both policy 1 and policy 2 demonstrated gradual but contrasting effects with regard to the gender and sociocultural discussions theme. Following policy 1, discussions showed a significant downward trend (regression coefficient: −0.02; 95% CI, −0.05 to −0.000; P < .05), while policy 2 was associated with a marked upward trajectory, with discussions increasing by 0.04 percentage points per day (regression coefficient: 0.04; 95% CI, 0.02-0.06; P < .001). For the vaccine acceptability theme, only policy 1 showed a statistically significant immediate effect, with discussion prevalence sharply declining by 4.41 percentage points (regression coefficient: −4.41; 95% CI, −5.99 to −2.84; P < .001) after its implementation, although no significant long-term changes were observed in the subsequent trend. With regard to the pandemic-related narratives theme, policy 1 showed a pronounced response, with discussions increasing by 4.79 percentage points (regression coefficient: 4.79; 95% CI, 2.72-6.85; P < .001) after its announcement, but these declined over time (regression coefficient: −0.03; 95% CI, −0.06 to −0.01; P < .010). These temporal trends for gender and sociocultural discussions, vaccine acceptability, and pandemic-related narratives are summarized in Figure 3. eFigures 4-6 in Supplement 1 present further details. Sensitivity analyses yielded results consistent with the primary analyses, with no material changes in the direction or magnitude of the observed associations (eTable 4 and eFigures 7-9 in Supplement 1). Weekly aggregated trends showed similar temporal patterns (eFigures 10-12 in Supplement 1).
Dot Plots Showing Daily Trends in Public Discussions on Social Media PostsThe shading indicates the 95% CI around the fitted trend line.
Discussion
HPV infection and cervical cancer prevention remain global public health challenges. Leveraging machine learning techniques, this study analyzed social media discussions around 2 major HPV policies in China to gain insights into public reactions and concerns regarding these health initiatives. Our findings show a sustained decline in discussions related to vaccine accessibility. Although policy 1 temporarily heightened public attention by expanding eligibility and stimulating demand, policy 2, as a more structural and system-oriented policy, likely alleviated public concerns about immediate access barriers, thereby resulting in a steeper downward trend than that observed prior to policy 1. There was a sustained decline in the vaccine accessibility theme, particularly around 3 key topics: vaccine shortages, financial burden, and vaccination experience sharing. The decline in discussions on vaccine shortages and financial burden could suggest that, as policies were introduced and implemented, these key issues have been progressively addressed and became less central in public discourse. The downward trend of vaccination experience sharing may reflect behavioral and psychological shifts that coincided with the normalization of vaccination over time; the sharing of vaccination experiences, once characterized by informational scarcity and a sense of novelty, gradually lost its demonstrative value and social appeal, and contributed to a decline in motivation for sharing such content.^38^
It is important to note that, despite a declining trend over time, discussions around vaccine accessibility consistently remained the most dominant theme in our dataset, echoing findings from previous studies.^39,40^ In China, HPV vaccines have not yet been incorporated into the National Immunization Program.^20^ Although the 2 policy interventions substantially alleviated public concerns about vaccine shortages and costs, which were accompanied by a gradual decrease in the intensity of related discussions, this does not imply that all potential barriers have been eliminated. As of March 2025, HPV vaccine reimbursement policies remain limited to pilot programs in selected provinces.^18^ These programs vary widely in scope and reimbursement levels, which has hindered their ability to fundamentally address the issues of low vaccine uptake and inequitable coverage across the country. Consistent with our findings, public calls for broader and more uniform insurance coverage have gradually intensified over time.
Previous studies have shown that, although early efforts such as free vaccination and school-based programs can substantially boost overall HPV vaccine coverage, uptake among low-income groups and young populations in remote areas often remains well below national averages.^41,42^ This situation also suggests that structural interventions alone, such as improving supply and reducing costs, may improve aggregate coverage but are not necessarily sufficient to narrow these disparities between population subgroups. Thus, China’s 2030 Action Plan for Accelerating the Elimination of Cervical Cancer not only seeks to expand insurance coverage and optimize reimbursement standards but also emphasizes multilevel strategies, including health education and community mobilization, to stimulate proactive vaccination uptake. Such integrated approaches are essential to ensure that HPV vaccination policies translate into equitable and sustainable public health outcomes. Our results further highlight that discussions related to HPV awareness and knowledge showed notable increases following the policy interventions. Previous social media–based studies have found a marked lack of public discourse around vaccine and disease knowledge. In contrast, our analysis found that, prior to the launch of policy 2, discussions of HPV awareness and knowledge remained persistently low.^40,43^ Following the policy’s introduction, however, we observed a significant increase in related discussions, associated with heightened public interest and engagement with HPV vaccine information. The results show that the overall level of public discourse regarding vaccine acceptability remained largely unchanged after the 2 policy interventions, emphasizing the necessity of tailored risk communication efforts to supplement structural policy actions.^44,45,46,47^
In addition, our findings showed a large increase in discussions on gender and sociocultural issues following policy 2, including topics related to women’s health rights, male vaccination debate, stigma, and moral judgment. This pattern highlights that cervical cancer prevention is not merely a biomedical challenge but is deeply intertwined with sociocultural factors. On Chinese social media platforms, HPV is frequently associated with cervical cancer and other female-specific diseases, while the seriousness of HPV infection in males and the importance of male vaccination remain largely overlooked.^40,48^ This has contributed to insufficient risk awareness among males and, in some cases, exposed female vaccine recipients to moralistic judgments and stigmatization in public discourse. The experiences of countries such as Australia, Canada, and Austria demonstrate that, when promotion strategies are overly focused on females, male vaccination coverage tends to lag for prolonged periods, limiting the achievement of herd immunity.^49,50,51,52^ In contrast, incorporating males into national immunization programs and adopting gender-neutral health communication frameworks have been shown to reduce these coverage gaps.^53,54,55^ In our study period (up to the end of 2024), HPV vaccination for males had not yet been approved in mainland China. Nevertheless, we observed persistent public inquiries on social media about “when men will be eligible” and “why male vaccination is necessary,” suggesting that policy 2 not only raised awareness of women’s health but also stimulated broader reflections on vaccine equity and gendered health rights. With the approval of China’s first HPV vaccine for males in January 2025, future efforts should simultaneously strengthen health education targeted at males, emphasizing that HPV prevention is a collective societal responsibility.
Limitations
This study has several limitations. First, because the data were derived from social media, they may be subject to demographic and geographic biases, with younger and urban users likely overrepresented. Second, social media discussions reflect online discourse rather than actual vaccination behaviors; increased discussion does not necessarily mean higher uptake. Third, findings are based on Weibo data, which may not represent all population segments or other online platforms. Finally, topic misclassification may have occurred due to the ambiguity and diversity of language use, particularly in metaphorical or implicit expressions. Future studies could integrate vaccination coverage data and advanced natural language models to address these challenges.
Conclusions
By analyzing 3 years of online conversations, our study highlights how national HPV vaccination policies in China were associated with shifts in public discourse on social media related to reducing concerns about vaccine accessibility while fostering greater health awareness and gender-related discussions. Understanding how policies influence public discussions is crucial for promoting equitable HPV vaccine uptake and advancing cervical cancer elimination. As digital communication continues to evolve with emerging technologies, understanding and analyzing social media discourse will become increasingly important for informing responsive and equitable public health strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh D, Vignat J, Lorenzoni V, . Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO Global Cervical Cancer Elimination Initiative. Lancet Glob Health. 2023;11(2):e 197-e 206. doi:10.1016/S 2214-109X(22)00501-036528031 PMC 9848409 · doi ↗ · pubmed ↗
- 2Ginsburg O, Bray F, Coleman MP, . The global burden of women’s cancers: a grand challenge in global health. Lancet. 2017;389(10071):847-860. doi:10.1016/S 0140-6736(16)31392-727814965 PMC 6191029 · doi ↗ · pubmed ↗
- 3Zhang X, Zeng Q, Cai W, Ruan W. Trends of cervical cancer at global, regional, and national level: data from the Global Burden of Disease study 2019. BMC Public Health. 2021;21(1):894. doi:10.1186/s 12889-021-10907-533975583 PMC 8114503 · doi ↗ · pubmed ↗
- 4de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020;8(2):e 180-e 190. doi:10.1016/S 2214-109X(19)30488-731862245 · doi ↗ · pubmed ↗
- 5Brisson M, Kim JJ, Canfell K, . Impact of HPV vaccination and cervical screening on cervical cancer elimination: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020;395(10224):575-590. doi:10.1016/S 0140-6736(20)30068-432007141 PMC 7043009 · doi ↗ · pubmed ↗
- 6Han J, Zhang L, Chen Y, . Global HPV vaccination programs and coverage rates: a systematic review. E Clinical Medicine. 2025;84:103290. doi:10.1016/j.eclinm.2025.10329040547442 PMC 12179740 · doi ↗ · pubmed ↗
- 7Pak L, Rollison J, Rabinowitz M, Faherty LJ. Human papillomavirus vaccine coverage surveys in low- and middle-income countries: current efforts and future considerations for very young adolescents. BMJ Glob Health. 2025;10(6):e 018731. doi:10.1136/bmjgh-2024-01873140514218 PMC 12164605 · doi ↗ · pubmed ↗
- 8Bruni L, Saura-Lázaro A, Montoliu A, . HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010-2019. Prev Med. 2021;144:106399. doi:10.1016/j.ypmed.2020.10639933388322 · doi ↗ · pubmed ↗